Keywords
Oncology, Pediatric clinical trials, Assent, Informed consent, Parental permission
Main Manuscript
In “Family Strategies to Support Siblings of Pediatric Hematopoietic Stem Cell Transplant Patients” [1], we described the 10 strategies used by families to support siblings. One of the strategies was sharing information. Interestingly, only about one third of the parents (Fathers (7/21, 33.3%), and Mothers (8/20, 40%)) indicated that they shared information with the patient about the transplant decision while over half of the children (10/17, 59%) reported that information was shared with them. The four strategies for sharing information are Exclusionary: Children not given information and not included in decision making; Informative: Children are informed but not included in the decision making; Collaborative: Children are at the center of the decision making with parents; Delegative: Children make the decision (See Table 1 and Figure 1) [2].
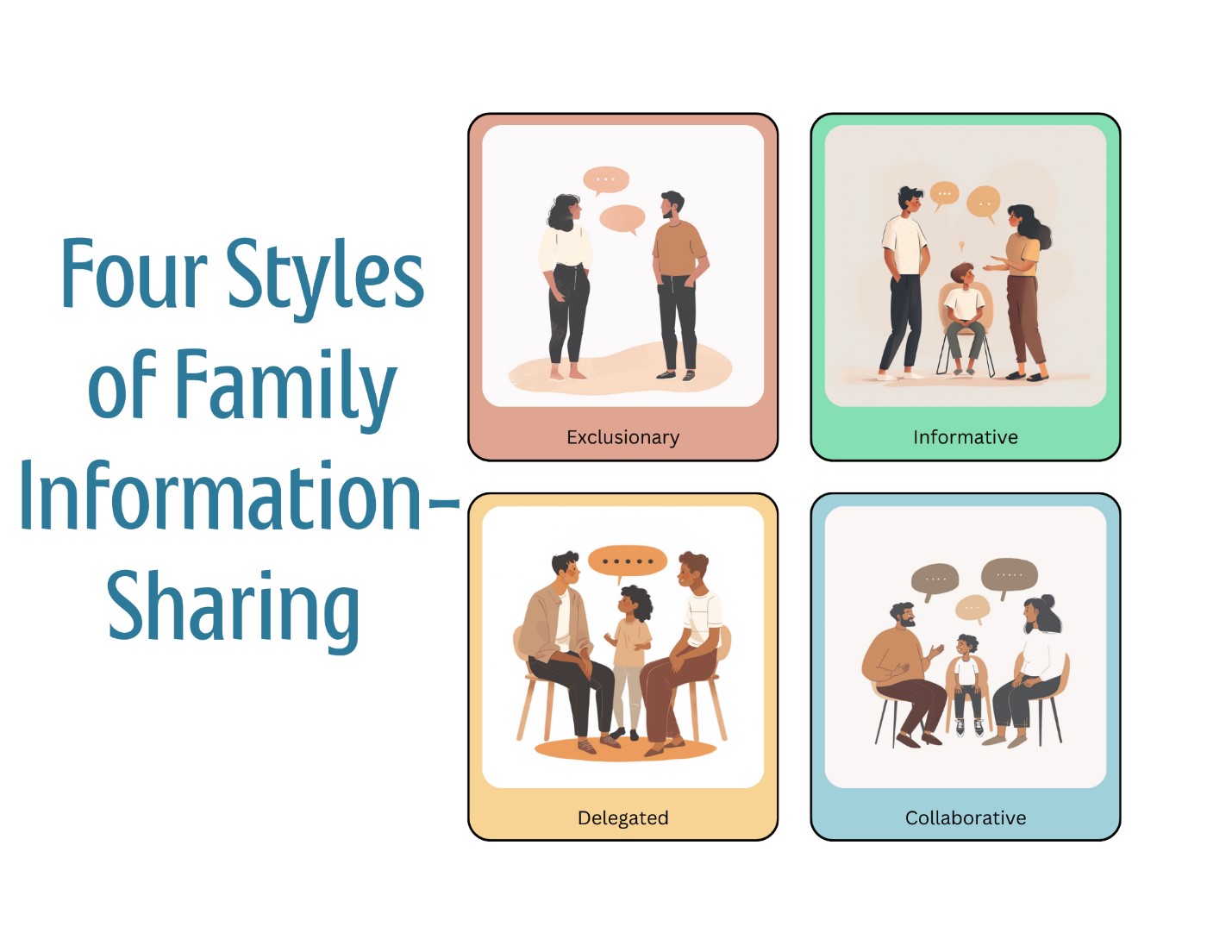
Figure 1. Family Styles of Information Sharing.
|
Family Information-Sharing Style |
Child is informed |
Child is included in the decision making |
Child makes the decision |
|
Exclusionary |
|
|
|
|
Informative |
x |
|
|
|
Collaborative |
x |
x |
|
|
Delegative |
x |
|
x |
One mother, who was very frank that she did not want to share information, said: “We really tried to downplay it. I didn’t want to put too much pressure on xxx, I mean, just in case it didn’t work or anything like that so. We didn’t give our children too much information .... We really tried not to have a lot of sad talks in front of the kids and that sort of thing as well, is a protection thing from a parent’s point of view.” Another patient expressed his anger at not being informed: “And the thing was, when I first developed cancer, my grandparents on that side didn’t want me to know anything about it because, “Oh ... I don’t want him to know that he could die.” What! Seriously! They think of me as a little kid because I’m my brother’s little brother. I’m always going to be the little kid, no matter what. It just pissed me off because I didn’t even know what kind of disease I had!”
Our takeaway from this study is that families should be informative or collaborative and openly share information about the disease with the child. However, our description of the information-sharing strategies is not just useful for families. It can also be useful for physicians who are consenting to pediatric treatments or pediatric clinical trials and trying to tailor the correct assent. Several articles identify difficulties for physicians in obtaining informed consent: providing the right amount of information, assessing patient’s understanding, assessing patient’s information preferences, and translating difficult technical concepts into lay language [3-5]. Given our research, we would add that it is necessary for the physician to the assess the family’s information-sharing style. If the family is exclusionary, the physician must be very careful to discuss with the family how to inform the child patient in the best way, if of assent age, so that the child can truly give assent. If the family is informative or collaborative, few issues should arise. If the family is delegative, the physician must work closely with the surrogate to make sure there is an informed adult involved in the parental permission. In short, the consent process must be tailored to the individual family.
Although our research was focused on pediatric bone marrow or stem cell transplants, information-sharing strategy assessment can also be useful with adults and in other disease types. Knowing whom the patient wants involved when important information is given is important in order to make sure the conversations are respectful of that patient.
In order to assess family information-sharing styes, a simple conversation is all that is needed. The conversation can look something like this; “I know when we are having our conversations, that I give you a lot of complicated medical information all at once and it would be helpful for me to know how you like to share information in your family. Do you prefer that I give you important medical information when you are alone, or do you want family here? If alone, do you like to keep this private or share it later with family? Whom in the family can I share information with if they ask?”
And for parents of pediatric patients, “And how much information do you like to share with your child? Should I talk to you first and then the child or should we have these conversations all together. And do you like the siblings to know what is going on?”
The requirements for proper assent also reveal the importance of assessing the family information-sharing strategy. In the “Ethical Issues in Pediatric Research”, William Bartholme lists four requirements for proper assent: “1) A developmentally appropriate understanding of the condition; 2) disclosure of the nature of the proposed intervention and what it will involve; 3) an assessment of the child’s understanding of the information provided and the influences that impact on the child’s evaluation of the situation; 4) a solicitation of the child’s expression of willingness to accept the intervention [6].” One aspect of assessing the child’s understanding and influences on a child’s evaluation is how much the parents are willing to share information with the child, so knowing the family information-sharing strategy is crucial.
Another study of ours demonstrates why assessing the family’s information-sharing strategy is so important.[7] When a provider does a deep dive into understanding family dynamics and how parents and their children interact and share information, they are on the way to establishing a human connection with the family. In our prior study, we found that establishing a human connection with the family increases clinical trial participation. At Winship Cancer Institute in Atlanta, Georgia, USA, 34% of the participants in Myeloma clinical trials self-report as African Americans, whereas the United States national average is 4.5%. To account for this high enrollment, we interviewed 61 African Americans who had consented to a clinical trial. The interview included the Human Connection scale developed by Mack et al. [8]. What we found was that our trial participants had strong human connections with their physicians. Having a human connection with one’s physician facilitated clinical trial enrollment even though our participants had experienced many clinical trial barriers such as arranging and paying for transportation to the trial, cost of the trial, and concern about side effects.
In the pediatric setting, establishing a human connection with both the parents and the child is important. If the researcher is to get to know both the parents and the children as whole persons whom they care about, they will need to understand the parents’ beliefs about how much information they think it is appropriate to share and how much information the child wants. In short, understanding the family’s information-sharing strategy is a key piece of establishing a human connection, since, while having an informed consent conversation, one cannot interact as one human respecting and caring about another human unless one knows how that person prefers to share important medical information. If they do not like to share information, then those important conversations should happen privately and quite the reverse if they want to have the whole family involved. We have included the human connection scale questions in an appendix to clarify what is involved in establishing a human connection.
In sum, it is important for clinicians seeking parental permission and child assent to assess the family’s information-sharing strategy in order to conduct a respectful and ethical informed consent.
Funding
No Funding was received for this short commentary.
Acknowledgements
I would like to acknowledge the ethics team at Winship for their valuable edits: Margie D. Dixon, Catherine D. Chalmers, Kersten Pierre.
References
2. Snethen JA, Broome ME, Knafl K, Deatrick JA, Angst DB. Family patterns of decision-making in pediatric clinical trials. Res Nurs Health. 2006 Jun;29(3):223-32.
3. Brown RF, Butow PN, Ellis P, Boyle F, Tattersall MH. Seeking informed consent to cancer clinical trials: describing current practice. Soc Sci Med. 2004 Jun;58(12):2445-57.
4. Albrecht TL, Penner LA, Ruckdeschel JC. Understanding patient decisions about clinical trials and the associated communication process: a preliminary report. J Cancer Educ. 2003 Winter;18(4):210-4.
5. Fallowfield L, Jenkins V, Farewell V, Saul J, Duffy A, Eves R. Efficacy of a Cancer Research UK communication skills training model for oncologists: a randomised controlled trial. Lancet. 2002 Feb 23;359(9307):650-6.
6. Vanderpool HY. The ethics of research involving human subjects: facing the 21st century. Frederick, MD: University Publishing Group; 1996.
7. McClary TS, Blee SM, Avinger AM, Dai Q, Switchenko J, Dixon MD, et al. Accounting for the High Enrollment of African Americans on Winship Cancer Institute's Myeloma Clinical Trials. Ethics Med Public Health. 2023 Apr;27:100877.
8. Mack JW, Block SD, Nilsson M, Wright A, Trice E, Friedlander R, et al. Measuring therapeutic alliance between oncologists and patients with advanced cancer: the Human Connection Scale. Cancer. 2009 Jul 15;115(14):3302-11.