Abstract
Purpose: This study aimed to determine the factors affecting Physiotherapists and minority group patients' relationship.
Methods: This study applied a systematic review design and the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guideline was used to conduct this study. Three databases were systematically searched including PubMed/Medline, Scopus, and CINAHL. The studies had to be in the English language and done in the UK from 1995-2022. The studies that met criteria were presented in a data extraction sheet for further thematic analysis.
Results: Of the 44 articles retrieved from the primary search, a total of 2 studies fulfilled the inclusion criteria. Major themes identified were language barriers, affecting understanding, rapport, and trust. Gender preferences and cultural awareness were other themes which emerged. Additionally, many Physiotherapists lack understanding of their patients' beliefs, preferences, and attitudes towards rehabilitation and recovery.
Conclusion: The study has identified gaps and areas for improvement in positively enhancing the relationship between Physiotherapists and minority group patients. Recommendations include increasing employment of Physiotherapist from diverse backgrounds through education initiative and promotion of the profession, promoting single-sex exercise groups and having Ethnic Minority Groups (EMG) focused modules in degree programmes.
Keywords
Physiotherapist, Physiotherapy, Ethnic minority patients, Ethnic minority groups, UK
Introduction
The role of Physiotherapy is focused on rehabilitation, health promotion, and treating conditions which has resulted in issues in movement [1]. Physiotherapy in recent years is seeing an influx of patients being referred due to musculoskeletal, respiratory, and neurological conditions as a drive for healthy lifestyle, exercise, holistic approaches as well as the musculoskeletal expertise of the Physiotherapist takes center stage within the economies globally [2-4]. It is evident that the World Health Organization has produced a fact sheet pertaining to this very subject about Physiotherapy rehabilitation. It shows an estimated 2.4 billion people globally would require Physiotherapy rehabilitation for their health condition [5]. Due to the General Practitioner (GP) retention crisis, there has been a change in mindset in healthcare in the United Kingdome (UK), where Physiotherapists are becoming first contact practitioners alongside other specialties [6]. Also, due to the current National Healthcare Service (NHS) backlog where waiting lists are reaching an all-time high for treatments, many more Physiotherapists are being trained and employed to ensure patients are seen and treated [7,8].
As societies have become more intercultural within the UK, pressures grow on Physiotherapists to understand the cultural attitudes, preferences, and opinions on treatment from different Ethnic Minority Groups (EMGs) as well as having to deal with poor funding, inadequate preparation, and staff shortages within the UK [9]. The six largest EMGs in the UK are Indian, Pakistani, Black Caribbean, Black African, Bangladeshi, and Chinese. The Asian, Asian British, or Asian Welsh group is now the largest EMG at 9.3% of the UK population, up 1.8% since 2011. The second largest group, Black, Black British, Black Welsh, Caribbean, or African, grew by 0.7% to 4%. Mixed or multiple ethnic groups, the third largest, also increased by 0.7% to 2.9%. Additionally, the other ethnic group saw a 1.1% rise from 2011 to 2021 [10]. Overall, EMGs accounted for 18.3% of the UK population in 2021. As the data showed all EMGs are on the rise it is projected to continually increase in the years to come [10]. In the evolving UK’s healthcare system, EMPs are inevitable to encounter Physiotherapists in various setting than ever before [11]. The demand and importance of Physiotherapists in inpatient or outpatient settings has not only increased the inevitability of EMPs to encounter the Physiotherapist for treatment [3,10]. Consequently, UK Physiotherapists must be prepared to address the diverse opinions, attitudes and preferences of EMG patients [12].
As the profession of Physiotherapy continues in attempting to define its professional identity and importance within the healthcare system, it has resulted in a lack of focus being placed upon conducting research, particularly in understanding the relationship influences, barriers, and factors between Physiotherapists and EMPs [14,15]. Physiotherapists follow a person/patient-centred care approach in which they attempt to ensure the patient is looked upon as an individual rather than the diagnosis therefore not being able to understand the EMP’s is going against the whole profession [3,16]. Not being aware and understanding of the EMGs’ beliefs, results in the trust and satisfaction of treatments to be hindered and impacted negatively as well as the profession being under threat in having an untrusted reputation among the EMGs [26]. Current trends show an overwhelming majority of research being conducted from the healthcare professionals’ perspective, particularly doctors and nurses with scarcely any data being produced from the Physiotherapy domain [12,16-19]. Intercultural care is seen as a complex relationship in which EMPs have their own beliefs, values, preferences, and attitudes on how care should be delivered [5,20]. There are various challenges which EMPs are facing daily in healthcare institutions in the UK where consultations feel fast paced and issues pertaining to gender preferences are not met for EMPs requiring this for cultural or religious beliefs. This does not help EMPs who have language barriers as it makes it near enough impossible to understand what is being done or said by the Physiotherapists as many EMPs are not used to being palpated or given exercises as a treatment [11,16,21]. It is important to take into consideration that countries in which the EMGs originate from, may not have encountered a Physiotherapist, or even heard of the profession. This is because the reliance and belief on treatments are heavily placed upon Doctors and Pharmacology within healthcare institutions in countries such as Pakistan which shows the gap between Physiotherapists and one of the largest EMGs in the UK can have a detrimental effect going forward if research and correct understanding cannot be made [9,12]. Due to a shift in healthcare dynamics, this study aimed to determine the factors affecting Physiotherapists and EMPs relationship in order to pave the way for a positive outcome for all parties involved. Being able to develop an understanding of attitudes and preferences between Physiotherapists and EMGs allows for trust and satisfaction to be gained and enhanced allowing for further development for both populations involved.
Methodology
Study design and criteria
The study design was a systematic review. The Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guide was used to identify, screen, scrutinise for eligibility lining it up with the protocol set prior to conducting the search. All types of studies (qualitative, quantitative, and mixed method) in the UK were considered in this review. The studies published from 1 January 1995 to 31 December 2022 and in the English language were examined and included from peer-reviewed journals and published books with full text available. The exclusion criteria set was to not include any review articles, letters to the editor, case reports and case series. Also, studies not conducted in the UK or the English language.
Search strategy
Three databases were used to identify relevant studies which included PubMed/Medline, Scopus, CINAHL and grey literature. Keywords were used to obtain relevant studies through three databases (PubMed, Scopus and CINAHL). (Physiothera* OR "Physical thera*" OR physio) AND ("ethnic group" OR minority OR migrants OR multicultural) AND (trust OR satisf* OR relation*) AND (attitudes OR perceptions OR Knowledge) AND (“UK”). Booleans operators were also employed in the search strategy (AND and OR) to obtain the best information.
Selection process
The process of selection begins by examining the titles and abstracts of the journals to identify relevant articles. These articles were transferred to Refworks® database software to screen journals found according to title, year, and author fields. Furthermore, duplicated articles and those studies not done in the UK were removed during the selection process. The shortlisted journals titles and abstracts were recorded into Refworks® database software according to author, year, title, and abstract. Also, two extra categories were created in which decisions regarding the journal were made according to the decision of the reviewer whether “yes or maybe”, include or “no”, exclude article in accordance with study title. These decisions were made by a single reviewer to prevent bias. The full text of articles which qualified as “maybe” were read for full details to conclude its relevance to this systematic review (See Figure 1). Furthermore, a data extraction sheet was developed to extract appropriate information required in being able to analyze and generate themes for this systematic review. The data extraction sheet shows the aims of the paper, the study population, methodology used, main findings and the quality assessment tool used to scrutinize the study.
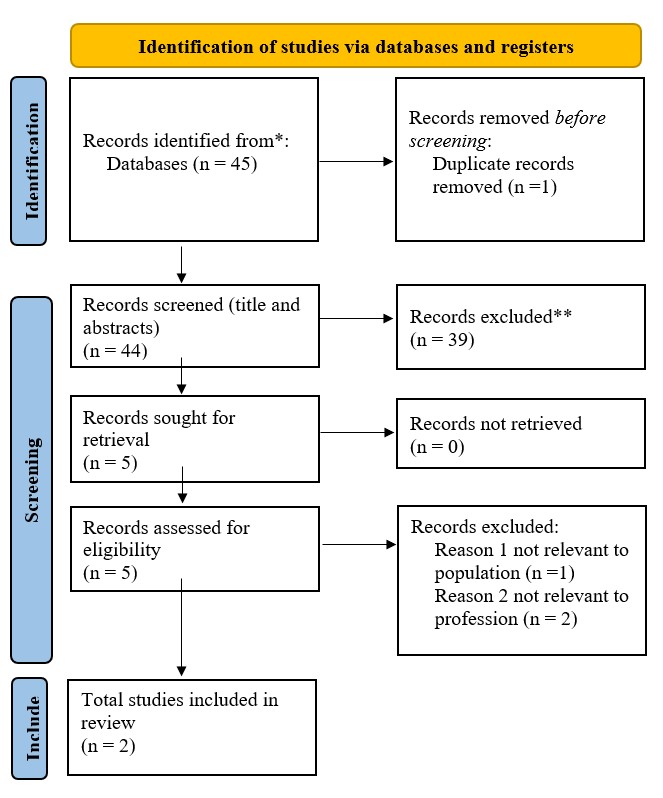
Figure 1. Prisma Flow Diagram.
Quality assessment
The Critical Appraisal Skills Programme (CASP) tool was used for qualitative studies [22]. The study conducted by Yeowell (2010), scored high on the CASP quality assessment tool. The AXIS tool which was for cross sectional studies [23]. This was used for the Jaggi and Bithell (1995) study which scored high on the AXIS tool.
Synthesis the finding
After extracting the relevant data from the included studies, narrative synthesis framework was used for data synthesis as the included studies may not have comparable variables. For narrative synthesis, identification, alignment, and critical review of data was carried out first followed by outcomes and conclusion. A minimum of 2 studies will be included to generate data in this systematic review. The studies were then grouped for synthesis for population groups and study designs. To address the heterogeneity of the differences in methodology, study population, differences in methodology, variability inn study population in different studies, an appropriate subgroup analyses was performed to explore the potential effect of heterogeneous elements. The data found was then presented through a table format. The CASP tool studies was used for qualitative studies [23]. The AXIS tool was adopted to assess the certainty of the synthesized evidence [23].
|
Study Characteristics |
Aim |
Study Population |
Method |
Main Findings |
Quality assessment tool |
|
Yeowell G, 2010 What are the perceived needs of Pakistani women in the Northwest of England in relation to Physiotherapy, and to what extent do they feel their needs are being met? [24] |
To gain an insight into the needs of female Pakistani service users in relation to Physiotherapy |
6 Pakistani women in the Northwest |
Qualitative Interviews |
Four main themes emerged from data analysis: issues of gender; language issues including the subthemes of cross-cultural communication, time, and materials; role of exercise; and acquiescence. |
High CASP tool |
|
Jaggi A, Bithell C, 1995 Relationships between physiotherapists' level of contact, cultural awareness, and communication with Bangladeshi patients in two health authorities [25]
|
The study had three aims: 1. To determine the contact that Physiotherapists in health authorities A and B have with Bangladeshi patients. 2. To assess the physiotherapists’ general knowledge of Bangladeshi culture and customs. 3. To highlight the problems Physiotherapists face in treating Bangladeshi patients and to seek possible solutions. |
Qualified Physiotherapists who are in two health authorities the UK
Total Physiotherapists responding to the questionnaires was Authority A= 46/64 Authority B= 22/36 A total of 68 questionnaires filled out of the 100 distributed between the two authorities |
Quantitative Questionnaires |
The findings indicated that contact with Bangladeshi people increased awareness of their culture and customs, but this did not result in fewer problems in their Physiotherapy management. Communication was found to be the greatest problem and more qualified interpreters and cultural awareness training are suggested as solution |
High AXIS tool |
Results
Themes identified
From the two studies, the themes which were identified to be relevant to the factors affecting the relationship between Physiotherapist and EMPs were summarized and categorized into four themes: Gender preference; Language barriers; Understanding the role of exercise in treatment rather than medication; Cultural awareness from a Physiotherapist perspective.
Theme one: Gender preferences
In terms of gender, both studies agreed that EMPs from Bangladeshi and Pakistani EMGs had a preference in being treated by same gender Physiotherapists. In one of the studies, it had found that “a female physio would be much preferred” [24]. Also, another participant had stated that “she wouldn’t have gone if it was male” as well as further statements pertaining to not wanting to partake in any exercise groups unless they were single-sex exercise groups [24]. This was further supported by the statement made by another respondent who stated, “she didn’t like Physiotherapy at all... as everyone was doing exercise together” [24]. In the second study, it had found similar findings regarding same-sex practitioners to which it stated, “Bangladeshi patients exhibit considerable modesty when removing their clothes or being touched by a Physiotherapist” [25].
Theme two: Language barriers
As communication is understood to be a joint responsibility, it is essential in being able to understand and develop treatments. There were three subthemes in one of the papers regarding language barriers [24]. The first subtheme mentioned was referred to as cross cultural communication which is the desire for EMPs Physiotherapists to be bilingual, so they can express what they are feeling regarding the exercise. One respondent in the study had mentioned “she doesn’t have the vocabulary to explain what she wants to say properly”. The second subtheme from this paper which emerged was the issue of time. Patients had reported that the consultations and explanations were fast paced which resulted in missed instructions, information and understanding of what is being done as English was a second language. A participant in the study had stated “maybe go through with them a little and slowly to make sure they understand what has been said because I tend to find some physios just go on and say everything in two sentences”. The third subtheme within language barriers stated that some Physiotherapists were able to give materials to patients to take home, which was written in the patient's language, but however one participant had responded by saying “A lot of Asian communities don’t read their own language anyway” and “information in English” was appreciated as a child at home was able to translate it to them for them to understand [24]. In addition to this, the second paper found that ten Physiotherapists in the study had blamed themselves in not being able to understand the cultural beliefs of the Bangladeshi patients which resulted in poor consultations and ineffective treatments [25]. Also, in this study the Physiotherapists stated that issues arose for Physiotherapists treating Bangladeshi patients in an outpatient setting where a thorough subjective examination is required for treatment to commence. As Physiotherapists are dependent on the patients report on improvement and treatment satisfaction, not being able to communicate resulted in more than 60% of patients not being able to discuss the effectiveness of treatment [25].
Theme three: Understanding the role of exercise in treatment rather than medication
Understanding the role of exercise became another apparent theme which stated that all the patients stated that exercise was not part of their Pakistani culture [24]. One of the respondents stated that due to living in “larger family homes” and “their background is agriculture and farming” they have not really had the time to do structured exercise as they are somewhat doing it in the fields [24]. Also, the same respondent mentioned that due to technological advancements such as dishwashers, washing machines and more mechanical equipment, it has resulted in a further sedentary lifestyle for themselves and their communities [24]. This ties in well with the theme of communication and language barriers where the role of exercise cannot be explained to EMP’s who have difficulties in understanding. This further complicates the trust element of Physiotherapist going forward where EMP’s may not trust exercise as a treatment method. The findings from the second study stated that more than half of the Physiotherapists felt that their own communication was ineffective in treating Bangladeshi patients resulting in compliance and understanding to treatment to be hindered further.
Theme four: Physiotherapists and their cultural awareness
There was an interesting finding in which one of the studies also looked at Physiotherapists and their cultural awareness [25]. This study had found that Physiotherapists who were community based were able to be more culturally aware than their hospital colleagues [25]. As community Physiotherapists are treating patients in their own home environment, this allows understanding of the Bangladeshi individuals customs and traditions within their own homes [3,25].
Discussion
The factors affecting Physiotherapists and EMP’s relationship are somewhat a long-term issue which needs to be addressed effectively. Prompted by the findings in this systematic review, it is evident that there is a lack of research being produced on this subject, even though the profession of Physiotherapy is becoming crucial in today's healthcare infrastructure within the UK [3]. Due to lack of research being conducted, an imbalance in understanding EMPs’ beliefs, attitudes and preferences are swept under the carpet or never understood by the Physiotherapists. This further increases tensions as explained in the literature review between EMP’s trusting the role of exercise as a means for treatment rather than medication [9,12]. In this systematic review, results show that four themes were identified between the two studies which were the underlying factors affecting the relationship between Physiotherapists and EMP’s. The themes identified were language barriers, cultural awareness and gender preferences from a Physiotherapist perspective [12,24].
The studies discussed language barriers extensively which demonstrated the crucial importance of communication, as this allows for a formation of meaningful relationships, trust, and rapport between Physiotherapist and EMPs to be developed [24,25]. If a Physiotherapist is unable to communicate effectively, the subjective examination which is conducted to direct the treatment will have reduced capability in being able to deliver the correct treatment further complicating the process in developing rapport and delivering person/patient centred care [27]. If this is to continually occur and interventions are not put in place to educate to create friendly relations, many EMGs will develop further animosity and distrust in the profession hindering the professions attempt in creating a professional identity for itself [15]. Also, if these issues are not resolved in being able to communicate and build an understanding of EMGs’ beliefs results in further tensions which will ripple through the healthcare infrastructure, resulting in additional reliance on medications and surgical treatments which could be managed through conservative Physiotherapy management. This will again create a downfall of the profession in losing its identity within communities in which EMGs are located, resulting in further complications for next generations not wanting to work or get involved within the profession, which ultimately results in a workforce which is not representative of the demographics [3,24,25]. The census conducted states that EMGs are expected to continue to increase where certain cities across the UK will be EMGs’ majority in comparison to natives [10]. This reiterates the fact that language barriers are going to continue to increase and be an issue if the profession does not create suitable methods in being able to tackle this and train the future workforce in being competent in dealing with EMPs who struggle to communicate and understand what is being done [28-31].
The issue pertaining to gender preference and modesty was echoed in both studies. This was stated from the Pakistani women [24] as well as the Physiotherapists from health authority A and B in treating Bangladeshi patients [25]. Not being culturally aware of the preferences and attitudes of the EMPs results in further complications with treatment resulting in person/patient centred care not being achieved [3,15,16]. In the study done by Yeowell (2010), the Pakistani women voiced concerns regarding not attending exercise classes due to men being present. If service improvements such as single sex exercise classes within Physiotherapy could be arranged or more abundance of with varied times and days, the participation of EMPs from this study may have increased. Also, due to this many EMPs may fail to attend Physiotherapy appointments as they know they will be asked to do exercise in mixed wards. The issue pertaining to modesty and gender preference seems to be apparent in EMPs who female are. However, the voices of the male EMPs have somewhat been ignored and understudied as there is no literature to be found on this. This unquestionably creates a bridge between the profession and EMPs and results in complications in trust and relationship as explained above. These findings are in harmony with Mujallad and Taylor (2016), who looked at ‘Modesty Among Muslim Women: Implications for Nursing Care’ [32]. This study states that, modesty is ‘central’ to the individuals who follow the Islamic way of life and are more than likely to withhold strong religious and cultural beliefs regarding covering of the body, guarding Interactions with persons of the opposite sex. This is of paramount importance for the Physiotherapists within the UK in being able to understand the reasons, beliefs, and attitudes towards gender preferences, as most of the migration into the UK has taken place from countries in which Islam is the main religion, hence will encounter EMPs during their careers [32].
Strengths and limitations of study
The strengths of this study include its focus on an under researched topic area within the profession of Physiotherapy which is a major gap identified. By conducting a systematic review, allows for critically analyzing the available literature providing an overview of the topic. The rigorous methodology applied following the PRISMA guidelines, which were adhered to thoroughly, ensuring transparency, reliability and creditability of the findings, allowing for solid foundation for research to be conducted in this field in the coming future.
The limitations of the study include the knowing of scarce data to be found was expected due to it being a niche topic area, which inherently limits available data and extent of findings. Additionally, only three databases were used which limits the amount of data to be found. If more databases were used it may have given more data to assess to give deeper insight allowing for more themes to be identified.
Conclusion
The relationship between Physiotherapists and EMPs is understudied in literature. There is a great emphasis placed upon this exact relationship through the Charted Society of Physiotherapy (CSP) and Health and Care Professional Council (HCPC) codes of conduct. Factors influencing this relationship include language barriers, gender preferences and cultural awareness. Appropriate interventions are vital for mutual understanding, as their absence may lead to distrust, complicate the professional identity, and hinder person-centred care ultimately reducing adherence and satisfaction to treatment.
The findings of this study can guide future qualitative and quantitative research on EMPs in the UK. These can ultimately be used to inform employers in the Physiotherapy sector about the importance of diverse workforces allowing for better representation of the community being treated. Effective communication and understanding of EMP’s beliefs, attitudes, and preferences can be achieved if Physiotherapists receive appropriate training and resources through the university institutions as well as employers. Such measures would create a harmonious relationship, fundamentally enhancing patient care and treatment outcomes.
It is evident that there is a lack of Physiotherapists working in the UK from an EMG. It is crucial for efforts to be made in the profession of Physiotherapy to further educate and expose the profession through initiatives such as delivering presentations in schools and places of worship. Additionally, promoting single sex exercise groups can encourage activity participation for patients in places of worship or the community centers rather than hospitals or clinics. Also, to further support the goal of incorporating this message it is crucial for a module to be added into the Physiotherapy degree programs addressing EMGs.
Future research needs to be conducted on primary qualitative research directly eliciting minority ethnic patient perceptions on physiotherapy should be concocted in the UK. Furthermore, there needs to be a significant focus placed on understanding religions and the barriers on Physiotherapy practice. For those in practice, surveys should be conducted locally looking at understanding the EMG’s within their locality and their beliefs, preferences and attitudes to Physiotherapy. Ultimately this would then lead the way in enhancing the Physiotherapy practice in ensuring it is person/patient centred to the specific area of practice. The CSP and HCPC need to tailor modules focusing on religious beliefs, attitudes and understanding within the UK which would equip future Physiotherapists and allowing for better adherence to treatment.
References
2. Downie F, McRitchie C, Monteith W, Turner H. Physiotherapist as an alternative to a GP for musculoskeletal conditions: a 2-year service evaluation of UK primary care data. Br J Gen Pract. 2019 May;69(682):e314-e320.
3. Killingback C, Tomlinson A, Stern J, Whitfield C. Teaching person-centred practice in physiotherapy curricula: a literature review. Physical Therapy Reviews. 2022 Jan 2;27(1):40-50.
4. Webb G, Skinner M, Jones S, Vicenzino B, Nall C, Baxter D. Physiotherapy in the 21st century. Contexts of Physiotherapy Practice. 2009:3-19.
5. Wikberg A, Eriksson K, Bondas T. Intercultural caring from the perspectives of immigrant new mothers. J Obstet Gynecol Neonatal Nurs. 2012 Sep-Oct;41(5):638-49.
6. Owen K, Hopkins T, Shortland T, Dale J. GP retention in the UK: a worsening crisis. Findings from a cross-sectional survey. BMJ Open. 2019 Feb 27;9(2):e026048.
7. Astrup J. Doctor google. Community Practitioner. 2018 Feb 1;91(1):28-9.
8. British medical association, 2022. NHS backlog data analysis [cited 2023 1 January]. Available from: https://www.bma.org.UK/advice-and-support/nhs-delivery-and-workforce/pressures/nhs-backlog-data-analysis#:~:text=The%20latest%20figures%20for%20October,slight%20increase%20from%20last%20month.
9. Safarani S, Ravaghi H, Raeissi P, Maleki M. Financial challenges of teaching hospitals and providing solutions. J Educ Health Promot. 2018 Dec 28;7:155.
10. Garlick S. Ethnic group, England and Wales: Census 2021. 2021. [cited 2023 on 10 January]. Available from https://www.ons.gov.UK/peoplepopulationandcommunity/culturalidentity/ethnicity/bulletins/ethnicgroupenglandandwales/census2021.
11. Johnson SK. Hmong health beliefs and experiences in the western health care system. Journal of Transcultural Nursing. 2002 Apr;13(2):126-32.
12. Basri R, Naseen M, Naz A. Factors affecting compliances with physiotherapy among stroke patients: physiotherapist's perspective: a study from Peshawar Pakistan. Pakistan Journal of Neurological Sciences (PJNS). 2017;12(3):26-31.
13. Patel N, Ferrer HB, Tyrer F, Wray P, Farooqi A, Davies MJ, et al. Barriers and Facilitators to Healthy Lifestyle Changes in Minority Ethnic Populations in the UK: a Narrative Review. J Racial Ethn Health Disparities. 2017 Dec;4(6):1107-1119.
14. Rath L, Faletra A, Downing N, Rushton A. Cross-sectional UK survey of advanced practice physiotherapy: characteristics and perceptions of existing roles. International Journal of Therapy And Rehabilitation. 2021 Jul 2;28(7):1-4.
15. Redmond R, Parrish M. Variables influencing physiotherapy adherence among young adults with cerebral palsy. Qual Health Res. 2008 Nov;18(11):1501-10.
16. Higginbottom GM, Safipour J, Yohani S, O'Brien B, Mumtaz Z, Paton P. An ethnographic study of communication challenges in maternity care for immigrant women in rural Alberta. Midwifery. 2015 Feb;31(2):297-304.
17. Dustmann C, Frattini T, Theodoropoulos N. Ethnicity and second generation immigrants. The Labour Market in Winter: the state of working Britain. 2011 Jan 27:220-39.
18. Molina-Mula J, Gallo-Estrada J. Impact of Nurse-Patient Relationship on Quality of Care and Patient Autonomy in Decision-Making. Int J Environ Res Public Health. 2020 Jan 29;17(3):835.
19. Moyle W. Nurse-patient relationship: a dichotomy of expectations. Int J Ment Health Nurs. 2003 Jun;12(2):103-9.
20. Yeowell G. 'Isn't it all Whites?' Ethnic diversity and the physiotherapy profession. Physiotherapy. 2013 Dec;99(4):341-6.
21. Higginbottom GM, Safipour J, Mumtaz Z, Chiu Y, Paton P, Pillay J. “I have to do what I believe”: Sudanese women’s beliefs and resistance to hegemonic practices at home and during experiences of maternity care in Canada. BMC Pregnancy and Childbirth. 2013 Dec;13:1-10.
22. Critical Appraisal Skills Programme. CASP Qualitative Checklist. 2018. [cited 2023 5 March]. Available from: URL https://casp-UK.net/.
23. Downes MJ, Brennan ML, Williams HC, Dean RS. Development of a critical appraisal tool to assess the quality of cross-sectional studies (AXIS). BMJ Open. 2016 Dec 8;6(12):e011458.
24. Yeowell G. What are the perceived needs of Pakistani women in the North west of England in relation to physiotherapy, and to what extent do they feel their needs are being met? Physiotherapy. 2010 Sep;96(3):257-63.
25. Jaggi A, Bithell C. Relationships between physiotherapists' level of contact, cultural awareness and communication with Bangladeshi patients in two health authorities. Physiotherapy. 1995 Jun 1;81(6):330-7.
26. World Health Organisation. Rehabilitation. Total number of people who would benefit from rehabilitation. 2024. [cited 2024 18 July]. Available from https://www.who.int/news-room/fact-sheets/detail/rehabilitation
27. Teng CI, Hsiao FJ, Chou TA. Nurse-perceived time pressure and patient-perceived care quality. J Nurs Manag. 2010 Apr;18(3):275-84.
28. Al Shamsi H, Almutairi AG, Al Mashrafi S, Al Kalbani T. Implications of Language Barriers for Healthcare: A Systematic Review. Oman Med J. 2020 Apr 30;35(2):e122.
29. Meuter RF, Gallois C, Segalowitz NS, Ryder AG, Hocking J. Overcoming language barriers in healthcare: A protocol for investigating safe and effective communication when patients or clinicians use a second language. BMC Health Serv Res. 2015 Sep 10;15:371.
30. Schwei RJ, Del Pozo S, Agger-Gupta N, Alvarado-Little W, Bagchi A, Chen AH, et al. Changes in research on language barriers in health care since 2003: A cross-sectional review study. Int J Nurs Stud. 2016 Feb;54:36-44.
31. Steinberg EM, Valenzuela-Araujo D, Zickafoose JS, Kieffer E, DeCamp LR. The "Battle" of Managing Language Barriers in Health Care. Clin Pediatr (Phila). 2016 Dec;55(14):1318-1327.
32. Mujallad A, Taylor EJ. Modesty Among Muslim Women: Implications for Nursing Care. Medsurg Nurs. 2016 May-Jun;25(3):169-72.