Abstract
Objective: To evaluate patient-reported experiences with post-operative acute pain management, assess unmet needs, and describe impacts of inadequately managed acute pain in the United States.
Methods: This mixed-methods, exploratory sequential study included concept elicitation interviews and a survey of adults who underwent abdominal, orthopedic, plastic, or general surgery within the past 90 days. Interviews were conducted to identify themes, which were used to inform the design of a survey assessing post-operative pain levels; acute pain medication usage, experiences, and behaviors; and impacts of pain on activities of daily living (ADLs), recovery, and work/school productivity. A subgroup analysis examined inadequately managed post-operative acute pain. Healthcare resource utilization was assessed as an exploratory outcome.
Results: Interview participants (n=17) reported impacts of inadequately managed pain on physical functioning, ADLs, sleep, mood/emotions, and recovery. Survey participants (n=323) reported severe pain at Week 2 post-surgery (mean=7.6/10) and moderate pain by Week 4 (mean=3.7/10). Among those who took opioids (95.4%), over 70% reported breakthrough pain. Survey participants expressed hesitancy to take some classes of medications, including opioids, due to concerns about side effects (84.6%) and drug dependence/addiction (36.6%). Participants reporting inadequate pain management (37.8%) indicated severe pain at Week 4 (mean=6.3/10), ongoing limitations in ADLs, interference with physical therapy, and slowed recovery. Many participants also reported frequent, unplanned healthcare utilization.
Conclusions: This research highlights patient-reported challenges with post-operative acute pain management and describes downstream consequences of inadequately managed pain.
Keywords
Post-surgical pain, Pain control, Inadequate analgesia, Patient experience, Pain management, Healthcare resource utilization (HCRU)
Introduction
Approximately 64 million surgeries are performed in the United States (US) annually [1,2]. Literature shows 86% of surgical patients report pain during the immediate post-operative period, and among them, up to 75% reported moderate-to-extreme pain [3]. Opioids are the most commonly prescribed medication class for post-operative acute pain management despite serious risks, including respiratory depression, constipation, development of opioid use disorder, and overdose [4-6]. To mitigate such opioid-related risks and improve post-operative pain management, opioids are often combined with non-opioid analgesics as part of a multimodal analgesia protocol [7]. This strategy often includes prescribing opioids along with gabapentinoids (e.g., gabapentin, pregabalin), acetaminophen, and/or nonsteroidal anti-inflammatory drugs (NSAIDs) with a goal of reducing the necessary dose of each drug to maximize pain relief and reduce side effects/risks associated with individual medications [7].
Despite advancements in multimodal strategies, acute post-operative pain continues to be inadequately managed in many patients, often resulting in downstream consequences including increased morbidity, impaired physical function, slowed recovery, and higher healthcare resource utilization (HCRU) and costs [8]. Inadequately managed post-operative pain may also lead to persistent pain and prolonged opioid use [8].
International registries such as PAIN OUT highlight global challenges in post-operative pain management, including variability in pain intensity, patient satisfaction, and provider/patient communication across surgical settings [9–11]. However, differences in healthcare systems and treatment philosophies limit the applicability of these findings to the US, and evidence on US patient-reported experiences with inadequately managed post-operative pain remains limited [12–16]. This study addresses this gap by examining US patients’ experiences with post-operative pain, oral medication use, and its impact on recovery and daily functioning through a mixed-methods approach.
Methods
Participant selection
Participants for the qualitative phase were recruited using purposive sampling, a nonprobability sampling method commonly used in qualitative studies [17,18]. Adults aged 18 years and older were eligible if they underwent abdominal or orthopedic surgery within 90 days prior to the interview and reported no prescription opioid use within 6 months prior to surgery (i.e., were opioid-naive). Potential participants were asked to consider their post-operative pain within 14 days following surgery; individuals who indicated their post-operative pain was inadequately managed and moderate to severe (defined as ≥4 on an 11-point numeric pain rating scale [NPRS], where 0 represented "No pain" and 10 represented "Worst pain imaginable") were eligible to participate. Individuals were excluded if they reported chronic pain (defined as lasting >3 months) unrelated to their surgery, had non-elective orthopedic surgery, or experienced a complication related to their surgery.
In the quantitative phase, individuals were eligible to participate if they underwent a general (colectomy, hemorrhoidectomy, cholecystectomy, or proctocolectomy), orthopedic (total knee arthroplasty [TKA], lumbar spinal fusion of 1–2 levels, total shoulder arthroplasty, or shoulder arthroscopy), or plastic surgery procedure (breast reconstruction or any plastic surgery procedure with skin autograft or musculocutaneous flap). These procedures were selected because they are known to result in moderate-to-severe post-operative acute pain [19]. Additional eligibility criteria for the quantitative phase required participants to be 30- to 90-days post-surgery at screening and able and willing to provide documentation confirming their surgical procedure and surgery date. To support data integrity and strengthen confidence in self-reported information, we sought to obtain surgical confirmation for up to 20% of participants. A randomly selected subset was asked to electronically submit de-identified documentation (e.g., surgical notes or insurance documents) which was then reviewed by the study team for verification. Exclusion criteria included more than one surgery in the 3 months prior to screening, clinical trial participation at the time of surgery and/or screening, or report of any of the following regarding a qualifying surgery: robot-assisted surgery; surgical complication(s) or infection requiring hospital admission; or surgery costs covered as part of an injury claim settlement. Surgery-specific exclusion criteria included emergent surgeries, same-day bilaterial TKA, and multilevel lumbar spinal fusion (>2 levels).
All participants were English-speaking, US-based adults recruited through preexisting patient panels, postings on social media, and patient advocacy organizations. The study was descriptive and non-comparative. Therefore, the target sample sizes were determined based on feasibility and expected precision of descriptive estimates rather than on hypothesis-driven inferential testing, and a priori power calculations were not conducted. For the qualitative phase, the sample size was determined using established criteria for thematic saturation in qualitative research rather than statistical power calculations [20,21]. The quantitative phase was designed to generate descriptive insights and did not include inferential hypothesis testing or subgroup comparisons. Because the objective was to describe overall post-operative pain experiences rather than compare outcomes across surgery types, no subgroup or inferential analyses were conducted. Descriptive statistics were reported in aggregate to reflect overall patient experience.
Study procedures
Qualitative phase
A targeted literature search was conducted to evaluate concepts relevant to this study population. Concepts identified included concern about opioid addiction and negative impacts of inadequately managed post-operative pain on physical functioning and activities of daily living (ADLs), sleep, emotional well-being, and work productivity. Based on these findings, a study-specific semi-structured interview guide was developed to explore the following key concepts: 1. Experiences with post-operative pain and recovery, 2. Use of pain medications and non-pharmacologic strategies, 3. Communication with healthcare providers, and 4. The perceived adequacy and impact of pain management. Interviewers were encouraged to probe as needed to elicit rich, detailed accounts of participants’ experiences. Interviews were conducted from May to July 2023 and lasted approximately 60 minutes. Sampling continued until conceptual saturation was achieved, meaning no new themes or subthemes emerged in successive interviews, indicating that the final sample size (n=17) was adequate for the study’s exploratory purpose. Although pain trajectories may vary by surgical type, thematic analysis revealed consistent experiences across participants. The inclusion of diverse surgical types was intentional, enabling identification of overarching themes relevant to real-world multimodal pain management rather than limiting interpretation to a single surgical context.
Quantitative phase
Results from the qualitative phase informed survey development to quantify patient-level impacts of post-operative acute pain management. The survey included a maximum of 70 items (total items varied by participant due to skip logic) designed to capture participant self-reported demographic and clinical characteristics; post-operative acute pain levels and pain management subsequent to hospital discharge; oral medications prescribed; behaviors and attitudes towards these medications, including opioids; impacts of pain on work/school, ADLs, mood, and health-related quality of life; and HCRU during the first month following surgery. Survey questions were tailored to address study objectives, administered online, and data were collected from April to November 2024. Items on the impacts of post-operative acute pain on ADLs and mood were answered using 11-point, categorical numeric rating scales (NRS), where 0 represented “Did not limit” or “Not at all” and 10 represented “Completely limited” or “Extremely,” respectively. NRS scores were further categorized as “no” (rating 0), “mild” (ratings >0–3), “moderate” (ratings >3–6), and “severe” (ratings >6–10).
Participants were asked to self-report whether they would describe their post-operative pain management within the first month as adequate (“I felt my pain was well managed”) or inadequate (“I felt my pain was not managed well”). A subgroup of participants self-reporting inadequately managed pain was described.
All study procedures were conducted in accordance with the ethical standards of WCG Institutional Review Board (IRB) and the Helsinki Declaration of the World Medical Association. Both studies were reviewed by the WCG IRB, a centralized IRB. The qualitative study was deemed IRB exempt; however, participants were still provided with an informed consent and study-specific information sheet, and they provided verbal consent prior to each interview for use of their audio and quotes in analyses and publications. The quantitative phase was approved by the IRB (approval #1367607), and all participants provided written informed consent prior to completing the survey. All data collected across both studies were fully anonymized to ensure participant confidentiality.
Analyses
Audio recordings were professionally transcribed verbatim, and each transcript was fully reviewed for accuracy and missing data, against the audio recording as necessary, and de-identified before coding and thematic analysis. Interview transcripts were coded and analyzed using both inductive and deductive thematic analysis [22] using NVivo12 (Lumivero, LLC) software. Survey responses were analyzed using univariate statistics and summarized descriptively. Statistical analyses were conducted using SAS® (Version 9.4; SAS Institute Inc., Cary, NC, USA).
Results
Qualitative phase
Participant characteristics
Seventeen adults participated in the qualitative phase (Table 1). Most participants were female (n=14, 82.4%) and White (n=10, 58.8%), with an average age of 49.7 years (median=51 years; minimum [min], maximum [max]=36, 67 years). Seven participants had recently undergone abdominal surgery, including gastric bypass, diagnostic laparoscopy, appendectomy, cholecystectomy, and Cesarean section procedures. Ten participants had recently undergone orthopedic surgery, including ankle reconstruction, hip replacement, knee replacement, and shoulder repair (e.g., rotator cuff surgery) procedures. Most procedures were inpatient (n=12, 70.6%), with hospital stays ranging from overnight to 6 days. On average, interviews were conducted 52.8 days post-surgery (median=52 days; min, max=24, 80 days).
|
|
Qualitative Sample |
|
|
|
Mean (SD) |
Min, Max |
|
Age in years |
49.8 (10.29) |
36, 67 |
|
Pain at its worst within 14 days of surgery (0-10 scale)a |
8.9 (1.03) |
7, 10 |
|
Sex Female Male |
n 14 3 |
% 82.4 17.6 |
|
Surgical category Elective orthopedic Abdominal |
10 7 |
58.8 41.2 |
|
Race/Ethnicity White Black or African American Asian Hispanic or Latino |
10 3 2 2 |
58.8 17.6 11.8 11.8 |
|
Abbreviations: Max: Maximum; Min: Minimum. a0 = “No pain” to 10 = “Worst pain imaginable.” |
||
|
Descriptions of post-operative acute pain |
|
I would say it was like a 9…I mean people have explained to me that, like, the pain score—it’s like a 10 when you’re like, crying and like, on the ground in a fetal position, and I never got to that point. I’d say a 9 is kind of like…I was really kind of overwhelmed with the pain, but I wasn’t crying. (Participant 01, abdominal, appendectomy) |
|
It was a 10. I…regretted the surgery. Asked my husband like, “Just take me out, cut my arm off, I don’t care. Like, this is awful.” (Participant 08, orthopedic, shoulder repair) |
|
Pain management |
|
Opioids |
|
The side effects it [oxycodone] did cause around—you know, vomiting and, and h-heavily—you know, nausea—that, that made me feel worse. That really, [made me] bedridden quite a bit. However, I will say it did numb the pain in a way that—at, at a deeper level, stronger level than the Advil or Tylenol. But it caused other problems. And so, I had to—choose: do I want to take the oxycodone and, and throw up? And be, you know, dizzy? Or just take the Tylenol and Advil and be somewhat functionable? And so, that was kind of the trade-off of it. (Participant 05, abdominal, cholecystectomy) |
|
[The doctor’s office] recommended, you know, I take Percocet, which I did, and that helped the pain but it upset my stomach…I didn’t feel good after taking it. (Participant 10, orthopedic, hip replacement) |
|
Opioids with OTC analgesics |
|
[Interviewer: Were you taking anything over the counter?] Not until later. I didn’t wanna mix them and I kept having questions about that. Like, if I take Tylenol in between, am I allowed to do that? Or is that a bad thing? And it took [my HCP] days to figure that out…They got back to me, but it was like, 3 days later. (Participant 04, abdominal, cholecystectomy) |
|
[The doctor] said “I want you to take [oxycodone] every—you know, 3 hours and I want you to combine it so when you’re taking the [oxycodone], you’re also taking Tylenol and in 3 hours, you’re taking the [oxycodone], you’re also taking Advil.” So, I was alternating every 3 hours, a high dosage of [oxycodone], with a dosage of Tylenol or Advil. (Participant 07, orthopedic, shoulder repair) |
|
Heat and cold therapy |
|
Other than the pain medicine, [I] was just constant[ly] icing, to the point where my physical therapist was like “You’re icing too much, [laughs] you need to back off the icing. I know you’re using as, like, pain control.” (Participant 06, orthopedic, knee replacement) |
|
Drivers of inadequate pain management |
|
Lack of effectiveness |
|
The medication just wasn't effective for me. I don't know if I was on the correct dosage or whatever but I didn't—I just tried to bear with it. I didn't even let my doctor know honestly cause I was just disappointed in how everything panned out. (Participant 09, abdominal, caesarean section) |
|
[T]he problem with this was…when I would take the oxycodone with the Advil and extra-strength Tylenol, it caused me to vomit. And so, it actually made me feel worse. I was dizzy. Experienced a lot of nausea from that and…it didn’t help me sleep…The pain management wasn’t handled well because it was—I wasn’t getting the rest, I wasn’t sleeping well and the mix of the medications—eventually…I’d stopped taking the oxycodone and just was taking the extra-strength Tylenol and Advil, and that helped but it wasn’t, certainly it wasn’t strong enough. It wasn’t helpful enough to numb some of that pain. (Participant 05, abdominal, cholecystectomy) |
|
Difficulty accessing HCPs |
|
If I had to call [the doctor] to ask a question, it took like, you know, an hour or 2 just to receive the answer, which happened a lot because I wasn’t, you know, told a whole lot of stuff to—afterwards. So, it was kind of frustrating. (Participant 04, abdominal, cholecystectomy) |
|
I called the [doctor’s] office and let them know that [that I was in pain]. I mean they didn't even, [sighs], they didn't call in—I had my surgery on a Thursday—and they didn’t call in the tramadol until Saturday. Or I didn’t get it ’til Saturday, and that wasn't a pharmacy issue. So, I don't know if he [the doctor] or the staff kind of dropped the ball. (Participant 02, orthopedic, ankle repair) |
|
Abbreviations: HCPs: Healthcare Providers; OTC: Over-the-Counter. |
Three themes emerged from interviews: descriptions of the ways participants experienced pain, how it was managed (i.e., oral medications and/or other treatments employed), and what they felt were the drivers and impacts of their inadequately managed acute pain (Box; Supplemental Table 1).
Post-operative acute pain: descriptors
Two-thirds of participants (n=11, 64.7%) indicated their post-operative pain started shortly after the nerve block or other local anesthetic subsided. For the remaining third (n=6, 35.3%), pain started after emergence or leaving the operating room. When describing their pain, participants used descriptors such as “throbbing” or “aching”; “sharp,” “spikes,” or “pinching”; “intense”; “hot” or “burning”; and “dull.”
Post-operative acute pain: pain management
Participants managed post-operative pain with prescription oral medications (n=16, 94.1%); over-the-counter (OTC) medications (n=12, 70.6%); and other, nonpharmaceutical options (n=17, 100.0%), including heat/cold therapy and rest. Nearly all participants (n=15, 88.2%) were prescribed and took opioids for post-operative pain. Most participants described post-discharge multimodal regimens that included supplementing opioids with OTC medications (n=12, 80.0%), such as acetaminophen (n=11, 91.6%), ibuprofen (n=7, 58.3%), and naproxen (n=2, 16.7%). Overall, participants experienced fewer side effects from non-opioid medications but also experienced less pain relief.
All participants reported difficulty managing their post-operative pain at home. More than half (n=9, 52.9%) changed their approach to pain management during the first 2 weeks following surgery, including starting a different prescription medication, adjusting the dose of their initial prescription medication (due to ineffectiveness or challenging side effects), or adding nonpharmaceutical agents and/or OTC medications to their pain management regimen. Just over half of participants (n=9, 52.9%) found opioids to be effective, but experienced unpleasant side effects, including vomiting, nausea, and dizziness. Others (n=7, 41.2%) felt opioids were only somewhat effective, describing the medications as dulling but not eliminating the pain. Participants typically adhered to prescribed opioid regimens; however, a few (n=3, 17.6%) expressed frustration due to breakthrough pain between doses.
Inadequately managed post-operative acute pain: drivers and impacts
Participants described several drivers of inadequate pain management, such as challenges with pain medications (n=12, 70.6%), difficulty accessing timely and/or attentive care from healthcare providers (HCPs; n=11, 64.7%), and minimal presurgical education resulting in unrealistic expectations for post-operative pain (n=6, 35.3%). All 17 participants described negative impacts of inadequately managed acute pain on their physical functioning, including challenges with walking and/or climbing stairs (n=12, 70.6%) and standing up from a seated position/lying down (n=4, 23.5%). Twelve participants (70.6%) reported challenges with completing ADLs, such as eating, bathing, dressing, and using the toilet; 12 (70.6%) also described difficulty with instrumental ADLs, such as cooking/preparing meals, cleaning, driving, and shopping. Because of these challenges, more than half the sample described needing help from others (n=12, 70.6%). Other impacts included negative effects on mood/emotions (n=11, 64.7%), sleep (difficulty falling asleep: n=10, 58.8%; difficulty staying asleep: n=8, 47.1%), work and productivity (n=9, 52.9%), and recovery from surgery (n=6, 35.3%).
Quantitative phase
Participant characteristics
Overall sample: A total of 651 individuals were screened during the quantitative phase; 323 were eligible and included in the final analytic sample. All eligible participants indicated willingness to provide confirmation of surgery; this documentation was requested and verified for a subset of participants (n=45, 13.9%). Demographic and clinical characteristics for the overall sample and an inadequately managed pain subgroup are provided in Table 2. Almost half of participants underwent orthopedic surgery (n=142, 44.0%), and similar proportions underwent general surgery (n=89, 27.6%) and plastic surgery (n=92, 28.5%). The average age was 53.5 (standard deviation [SD]=11.20) years, approximately one-fifth were over 65 years of age (n=58, 18.0%), and over half were female (n=176, 54.5%). Most of the sample had commercial insurance at the time of surgery (n=235, 72.8%), while 62 participants (19.2%) were enrolled in Medicare or Medicare Advantage, and 28 (8.7%) were enrolled in Medicaid.
|
|
Quantitative Sample (N=323) |
Inadequately Managed Pain Subgroup (n=122) |
|||
|
|
Mean (SD) |
Min, Max |
Mean (SD) |
Min, Max |
|
|
Age in years |
53.5 (11.20) |
18, 78 |
54.6 (10.96) |
27, 35 |
|
|
Sex Female Male Prefer not to answer |
n 176 137 10 |
% 54.5 42.4 3.1 |
n 65 51 6 |
% 53.3 41.8 4.9 |
|
|
Surgical category Orthopedic surgery Plastic surgery General surgery |
n 142 92 89 |
% 44.0 28.5 27.6 |
n 70 29 23 |
% 57.4 23.8 18.9 |
|
|
Racea White Black or African American Asian Native Hawaiian/Pacific Islander I prefer not to answerb |
n 135 54 34 30 55 |
% 41.8 16.7 10.5 9.3 17.0 |
n 58 23 11 7 6 |
% 47.5 18.9 9.0 5.7 4.9 |
|
|
Ethnicity Not Hispanic or Latino Hispanic or Latino I prefer not to answer |
n 226 40 57 |
% 70.0 12.4 17.6 |
n 85 15 22 |
% 69.7 12.3 18.0 |
|
|
Insurance type(s) at time of surgerya Commercial health insurancec Medicare insurance Medicaid (MediCal for California residents) Veterans Affairs/TRICARE No insurance coverageb |
n 235 62 28 9 1 |
% 72.8 19.2 8.7 2.8 0.3 |
n 67 31 20 6 0 |
% 54.9 25.4 16.4 4.9 0.0 |
|
|
Abbreviations: Max: Maximum; Min: Minimum. |
|||||
Inadequately managed pain subgroup: Over a third of participants reported inadequately managed post-operative acute pain (n=122, 37.8%). The most frequently reported reasons included pain experienced after surgery was greater than expected (n=85, 69.7%), pain medications did not relieve the pain (n=84, 68.9%), pain resulted in longer-than-expected recovery time (n=70, 57.4%), pain medications resulted in unwanted side effects (n=52, 42.6%), and difficulty in contacting surgeon to discuss pain management (n=37, 30.3%). Participant demographic and characteristic distributions were similar to the overall sample (Table 2). However, compared to the overall sample, larger proportions of participants in this subgroup were enrolled in Medicare (n=31, 25.4%) and/or Medicaid (n=20, 16.4%) at time of surgery.
Post-operative acute pain levels
All participants experienced moderate-to-severe pain in the days and weeks after surgery (Table 3). On average, participants experienced severe levels of acute pain during Week 2 following surgery (mean ± SD, 7.6 ± 1.8). While pain levels improved over time, average pain scores indicated moderate pain during Week 4 after surgery (3.7 ± 2.9). The inadequately managed pain subgroup experienced severe pain, on average, during Week 4 post-surgery (6.3 ± 2.3).
|
|
Overall Sample |
Inadequately Managed Pain Subgroup |
||||||
|
|
n |
% |
n |
% |
||||
|
Day(s) of worst pain, first 7 days post-surgerya |
|
|
||||||
|
The day of surgery |
171 |
52.9 |
52 |
42.6 |
||||
|
One day after surgery |
157 |
48.6 |
75 |
61.5 |
||||
|
Two days after surgery |
138 |
42.7 |
74 |
60.7 |
||||
|
Three days after surgery |
111 |
34.4 |
67 |
54.9 |
||||
|
Four days after surgery |
73 |
22.6 |
54 |
44.3 |
||||
|
Five days after surgery |
63 |
19.5 |
53 |
43.4 |
||||
|
Six days after surgery |
58 |
18.0 |
52 |
42.6 |
||||
|
Seven days after surgery |
57 |
17.7 |
51 |
41.8 |
||||
|
|
Mean |
SD |
Median |
Min, Max |
Mean |
SD |
Median |
Min, Max |
|
Rating of worst pain experienced, Weeks 2-4 post-surgeryb |
|
|
|
|
||||
|
Week 2 |
7.6 |
1.80 |
8.0 |
3, 10 |
8.9 |
1.34 |
9.5 |
3, 10 |
|
Week 3 |
5.8 |
2.39 |
6.0 |
0, 10 |
7.9 |
1.77 |
8.0 |
2, 10 |
|
Week 4 |
3.7 |
2.86 |
3.0 |
0, 10 |
6.3 |
2.33 |
6.0 |
0, 10 |
|
Abbreviations: Max: Maximum; Min: Minimum. aGroups are not mutually exclusive and may not add up to 100%. b0 = “No pain” to 10 = “Worst pain imaginable”; pain rating categories: 0 = “no,” >0–3 = “mild,” >3–6 = “moderate,” >6–10 = “severe.” |
||||||||
Post-operative acute pain medication: medication utilization, experiences, and behaviors
Overall sample: All participants were prescribed at least one oral medication, including opioids, NSAIDs, and/or gabapentinoids, to manage acute pain in the first month following surgery (Table 4). Every participant who filled one or more prescriptions reported taking at least one dose of pain medication. Most participants were prescribed at least one opioid (n=311, 96.3%); however, a few participants did not take the opioid (n=3, 1.0%). Of the remaining 308 participants, 130 (42.2%) took an opioid(s) as monotherapy and 178 (57.8%) did so as part of multimodal analgesia that also included gabapentinoids, NSAIDs, and/or acetaminophen. Most participants reported at least one side effect associated with their pain medication(s) (n=281, 87.0%), with constipation (n=170, 52.6%), drowsiness (n=128, 39.6%), dizziness (n=88, 27.2%), and nausea (n=86, 26.6%) most commonly reported (Supplemental Table 2).
|
|
Overall Sample |
Inadequately Managed Pain Subgroup |
||
|
|
n |
% |
n |
% |
|
Medications prescribed in the first month after surgerya |
(N=323) |
(n=122) |
||
|
Opioids Strong opioids (e.g., oxycodone, oxycodone with acetaminophen) Moderate opioids (e.g., hydrocodone, hydrocodone with acetaminophen) Other opioids (e.g., tramadol, acetaminophen with codeine) |
311 149 180 67 |
96.3 46.1 55.7 20.7 |
117 66 64 45 |
95.9 54.1 52.5 36.9 |
|
Gabapentinoids (e.g., gabapentin, pregabalin) |
54 |
16.7 |
35 |
28.7 |
|
Nonsteroidal anti-inflammatory drugs (e.g., ibuprofen, naproxen, aspirin) |
164 |
50.8 |
64 |
52.5 |
|
Other non-opioid pain relief medications (e.g., acetaminophen) |
30 |
9.3 |
13 |
10.7 |
|
Other, not listed above |
12 |
3.7 |
6 |
4.9 |
|
None |
0 |
0.0 |
0 |
0.0 |
|
Opioid analgesia strategy in the first month after surgeryb |
(n=308) |
(n=106) |
||
|
Monotherapy/Only took opioids (i.e., strong, moderate, or other) |
130 |
42.2 |
40 |
37.7 |
|
Multimodal/Took both opioids and non-opioids |
178 |
57.8 |
76 |
71.7 |
|
aAll patients were prescribed medications for acute pain; groups are not mutually exclusive and may not add up to 100%. bThese rows represent participants who were prescribed and took at least one opioid in the first month after surgery. |
||||
Among participants who took opioids, either as monotherapy or as part of multimodal analgesia, over 70% (n=216) reported breakthrough pain between opioid doses. To address this, participants took OTC medication (n=114, 52.8%), used non-medication therapy (e.g., heat/cold therapy; n=98, 45.4%), or took their next opioid dose earlier than prescribed (n=81, 37.5%).
Some participants indicated hesitancy or refusal to take certain pain medications (n=123, 38.1%). While nearly half of participants asked their doctors to prescribe a strong opioid (e.g., oxycodone or oxycodone with acetaminophen; n=148, 45.8%), nearly a quarter of participants expressed a degree of reluctance to taking this class of opioid (n=79, 24.5%). This latter proportion includes participants who told their physicians they did not want a strong opioid prescription (n=42, 13.0%) or that they were hesitant to take them (n=37, 11.5%). Approximately 1 in 7 participants expressed a reluctance to take gabapentinoids, such as gabapentin or pregabalin, for post-operative pain (n=45, 13.9%). The top reasons for hesitancy or refusal to take prescription acute pain medications, including opioids, were concern about potential side effects (n=104, 84.6% of this subgroup) or developing drug dependence or addiction (n=45, 36.6% of this subgroup).
Inadequately managed pain subgroup: Among the 122 participants with inadequately managed pain, 62.3% (n=76) used a multimodal analgesia approach, taking both prescription opioids and non-opioids. An additional 32.8% (n=40) relied solely on prescription opioids, while 4.9% (n=6) did not use opioids. Notably, almost all participants in this subgroup reported breakthrough pain between opioid doses (n=115, 99.1%). Many participants experienced at least one side effect associated with pain medication(s) (n=105, 86.1%). The most frequently reported side effects included constipation (n=67, 54.9%), drowsiness (n=52, 42.6%), nausea (n=45, 36.9%), and dizziness (n=40, 32.8%) (Supplemental Table 2).
Participant ratings of post-operative acute pain medication: All participants were asked to rate their pain medications as “Poor,” “Fair,” “Good,” or “Excellent.” Almost 60% rated their medications as “Poor” (n=92, 28.5%) or “Fair” (n=93, 28.8%), nearly a third reported their medications as “Good” (n=97, 30.0%), and the remaining 12.7% (n=41) rated their medications as “Excellent.” In contrast to the overall sample, 97.5% (n=119) of participants in the inadequately managed pain subgroup that rated their pain medications as “Poor” (n=89, 73.0%) or “Fair” (n=30, 24.6%).
Impacts of post-operative acute pain on adls, recovery, and work/school productivity
Overall sample: Nearly 40% (n=123) of participants reported their pain was not well managed while recovering at home. Participants indicated post-operative acute pain negatively impacted their ADLs, sleep, recovery, physical therapy (PT), and ability to return to or be productive at work/school. Figure 1 displays descriptive statistics for each assessed ADL. Mean (±SD) scores for the overall sample showed moderate impacts across all ADLs and ranged from 5.8 (± 2.9) for “Tasks such as cleaning and cooking/preparing meals” (highest) to 4.4 (± 2.7) for “Activities out of bed (sitting in a chair or standing at the sink)” (lowest). ADLs related to physical functioning, such as walking, climbing stairs, housework, and additional daily activities, were impacted at a moderate level, with mean scores falling between 4.4 and 5.8. In addition to impacts on ADLs, participants also reported that pain delayed their return to regular activities (n=153, 47.4%) and negatively impacted participation in PT (n=80 of 164 participants reporting PT as part of recovery, 48.8%). Among the 68 participants who had returned to work/school at time of survey completion, 25.0% (n=17) indicated post-operative pain interfered with work/school productivity. On average, participants missed 13.2 (± 11.1) days (range: 0-45 days) of work/school.
Inadequately managed pain subgroup: Participants with inadequately managed pain reported severe limitations across all ADLs, with the greatest limitations reported for “normal tasks at work, school, and around the house” (mean ± SD, 7.2 ± 2.3), “tasks such as cleaning and cooking/preparing meals” (7.1 ± 2.5), and “basic daily tasks, such as bathing, dressing, or using the toilet” (7.0 ± 2.4; Figure 1). Inadequately managed pain also impacted participants’ ability to “Fall asleep,” “Stay asleep,” and “Get the sleep [they] needed”.
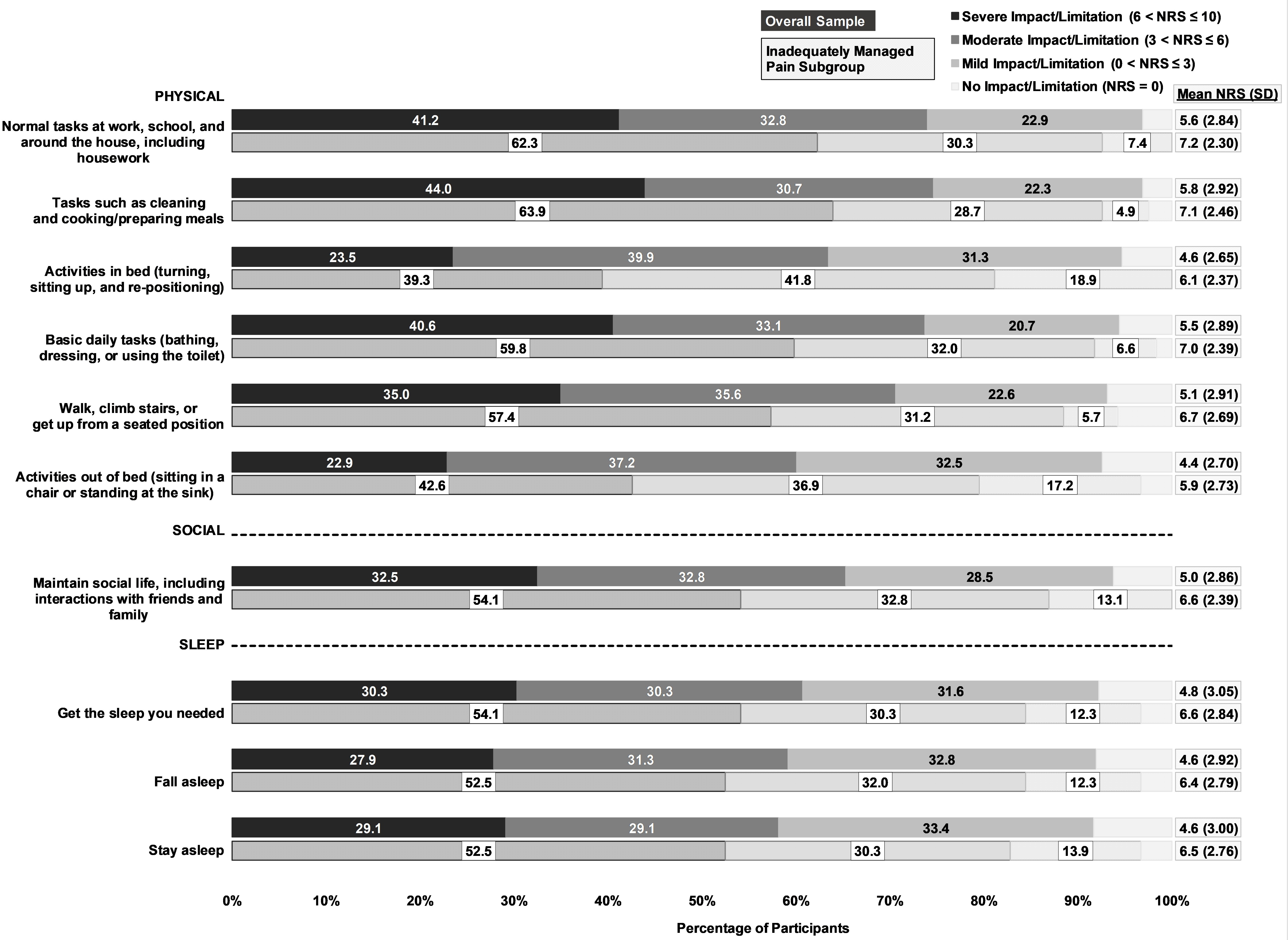
Figure 1. Impact of post-operative pain on ADLs in the first 2 weeks after surgery among survey participants.
Inadequately managed pain also delayed participants’ return to regular activities, and their participation in PT. Almost all participants indicated pain delayed return to regular activities (n=114, 93.4%). Among the 59.8% (n=73) that received PT, 84.9% (n=62) reported pain negatively affected their ability to perform PT.
Return to work and productivity were also negatively impacted in this subgroup. At the time of survey completion, 13 participants (46.4%) had returned to work/school and reported an average of 21.7 ± 12.8 work/school days lost after surgery (range: 4–45 days). Among those who had returned to work/school, 84.6% (n=11) indicated pain interfered with work/school activities.
Unplanned HCRU associated with post-operative acute pain
Frequency and types of unplanned, pain-related healthcare visits during the first month following surgery were evaluated. Examples included visits to physicians (tele-health or office), urgent care, and the emergency room. Participants most frequently reported tele-health/virtual visits with physicians (n=108, 33.4%), followed by visits to their surgeon’s office (n=78, 24.1%), their primary care physician’s office (n=33, 10.2%), the emergency room (n=33, 10.2%), and urgent care (n=16, 5.0%), within the first month following surgery due to acute pain. These proportions were nearly double for participants with inadequately managed pain, who also most frequently reported tele-health/virtual visits with physicians (n=78, 63.9%), followed by visits to their surgeon’s office (n=60, 49.2%), the emergency room (n=31, 25.4%), their primary care physician’s office (n=22, 18.0%), and urgent care (n=14, 11.5%).
Discussion
This mixed-methods study provides contemporary, US patient-centered evidence that inadequately managed post-operative acute pain remains common and clinically consequential, even among patients receiving prescription opioids as part of multimodal analgesic regimens. Importantly, the results from this study extend beyond documenting the presence of post-operative pain to illustrate how insufficient pain control directly affects functional recovery, including the ability to perform activities of daily living, and healthcare utilization, highlighting persistent gaps between current pain management strategies and patient needs.
For example, a key finding is that commonly used analgesic approaches, including prescription opioids and multimodal regimens, did not consistently achieve adequate pain control from the patient perspective. Breakthrough pain was frequently reported despite adherence to prescribed regimens, suggesting that current treatment paradigms may not reliably provide sustained analgesia during the early post-operative recovery period. This observation has important clinical implications, as uncontrolled pain during this phase may impair participation in rehabilitation, delay mobilization, and prolong functional recovery. Moreover, the frequent occurrence of medication-related side effects underscores the clinical trade-offs inherent in existing pharmacologic options, where tolerability and effectiveness may be difficult to optimize simultaneously. These findings reinforce the need for analgesic strategies that provide effective and sustained pain relief while minimizing adverse effects.
Patient attitudes toward pain medications also emerged as an important factor influencing post-operative pain management. Many participants expressed reluctance to use opioids or other prescribed analgesics due to concerns about side effects or addiction, even when experiencing substantial pain. This highlights a critical tension between the clinical need for effective analgesia and patient concerns about medication-related risks. In the current opioid stewardship environment, patient hesitancy may contribute to undertreatment of acute pain or inconsistent medication use, potentially compromising recovery. These results underscore the importance of incorporating patient-centered communication and shared decision-making into post-operative care, including clear discussion of analgesic benefits, risks, and appropriate use expectations.
This study also demonstrates that inadequately managed post-operative pain has meaningful downstream consequences for recovery and healthcare utilization. Patients reporting inadequate pain management described ongoing functional limitations, disrupted sleep, and delayed return to normal activities, which are clinically relevant markers of recovery. These impacts extended to participation in physical therapy and work productivity, suggesting that insufficient pain control may contribute to prolonged recovery trajectories and functional impairment. Furthermore, the high frequency of unplanned healthcare encounters among patients with inadequately managed pain suggests that insufficient post-operative pain control may increase healthcare utilization. From a health system perspective, these findings highlight inadequately managed post-operative pain as not only a clinical concern but also a potential driver of avoidable healthcare use.
Importantly, this study also identifies modifiable aspects of perioperative care that may improve patient outcomes. Participants frequently described unmet needs related to expectation-setting and access to timely clinical guidance. Many reported the intensity of their acute pain surpassed expectations or that they lacked adequate information about how else to manage pain after discharge. These findings echo guidelines from the American Pain Society, reinforcing the importance of clear, realistic communication and provider accessibility for effectively managing acute pain [23] and suggest that improving perioperative education and post-discharge communication may represent actionable opportunities to enhance post-operative pain management.
Results from this study are consistent with prior research demonstrating that inadequately controlled post-operative pain remains common despite routine use of prescription opioids and multimodal analgesic regimens. Large US patient surveys have shown that most surgical patients experience moderate-to-severe pain following surgery, with many reporting dissatisfaction with pain control [3]. Similarly, international registry studies, including the PAIN OUT registry and related analyses, have documented substantial proportions of patients reporting inadequate pain relief and unmet pain management needs [9–11]. These results suggest that challenges in achieving effective post-operative pain control persist across diverse healthcare settings and geographies. Variability in opioid prescribing patterns and patient response further highlights limitations of current analgesic strategies in consistently achieving adequate pain relief [24]. Additionally, inadequate post-operative pain control has been associated with delayed recovery, functional impairment, and increased healthcare utilization [8,25,26]. Together, these findings reinforce the need for improved analgesic strategies that better address patient needs during post-operative recovery.
These data hold significant implications for clinical practice. First, they highlight the need for continued optimization of post-operative analgesic strategies that improve effectiveness while minimizing adverse effects. Second, they underscore the importance of patient-centered post-operative care, including improved education, expectation-setting, and communication. Finally, they suggest that improving post-operative acute pain control may have broader implications for recovery, functional outcomes, and healthcare utilization. Future research using procedure-specific cohorts or larger stratified samples may help further characterize differences in pain trajectories and management needs across surgical populations.
Several limitations should be considered when interpreting these findings. As a patient-reported study, results may be influenced by recall or social desirability bias. Participants may not have accurately remembered details of their post-operative pain or medication use or may have provided responses they perceived as more socially acceptable. However, patient-reported experience is itself a critical component of pain assessment and recovery, as pain is inherently subjective. To address social desirability bias in the qualitative phase, interviewers were trained in using active listening and neutral language and the interview guide was designed to build rapport and trust with participants to support truthful responses. Additionally, perioperative clinical details, such as intraoperative analgesic techniques (e.g., nerve blocks or intraoperative analgesia) were not collected, limiting the ability to assess their influence on post-discharge pain experiences. These data were not collected because patients often have limited awareness of medications administered during surgery, and such data would be subject to substantial recall bias. Additionally, the findings may have limited generalizability due to potential self-selection bias from the recruitment methods and the high proportion of commercially insured participants. Nonetheless, the mixed-methods design strengthens confidence in the results by integrating qualitative and quantitative data, and the inclusion of multiple surgical types was intentional to capture broad patient experiences and common challenges in post-operative pain management across real-world surgical settings.
Conclusions
This study offers important insights into post-operative acute pain management, highlighting current strategies, whether relying solely on opioids or as part of multimodal analgesia, may be insufficient and can lead to unwanted side effects. The mixed-methods study design combined the strengths of both qualitative and quantitative methods, resulting in a comprehensive exploration of patient experiences with post-operative pain management as well as challenges with oral pain medications available during the study period. The results of this study highlight challenges with acute pain management therapies, including opioids, and the consequences of inadequately managed acute pain, such as impacts on ADLs and strains on recovery, and underscore the need for improved treatment options and patient-centered approaches for managing post-operative acute pain.
Conflict of Interest Statement
Vinod Dasa: Consulting fees from Vertex Pharmaceuticals Incorporated. Lauren A. Crowder, Meaghan O’Connor, Nana Y. Asiedu, and Alexandra J. Feld: Employees of IQVIA, which received funding from Vertex Pharmaceuticals Incorporated for this research. Ann M. Menzie: Employees and stockholders of Vertex Pharmaceuticals Incorporated. Moeen Panni: Former employee of Vertex Pharmaceuticals Incorporated and may own stock or stock options in the company.
Funding Sources
Funding was provided by Vertex Pharmaceuticals Incorporated. In addition, Vertex Pharmaceuticals Incorporated contributed to the design, interpretation, and activities surrounding publication of this manuscript.
Acknowledgements
The authors would like to thank the interview and survey participants who contributed their experiences to this study. Additionally, the authors thank Drs. Elizabeth Brennan (qualitative data collection, analysis, and interpretation), Kristen McCausland (quantitative oversight and interpretation), Laura Tesler Waldman (qualitative oversight and interpretation), and Cary Thurm (quantitative data analysis), as well as Kristen Bouzaid (project management) and Emily Chicklis (editorial and research assistance) from IQVIA for their expertise and contributions to this work.
References
2. Weiser TG, Regenbogen SE, Thompson KD, Haynes AB, Lipsitz SR, Berry WR, et al. An estimation of the global volume of surgery: a modelling strategy based on available data. Lancet. 2008 Jul 12;372(9633):139–44.
3. Gan TJ, Habib AS, Miller TE, White W, Apfelbaum JL. Incidence, patient satisfaction, and perceptions of post-surgical pain: results from a US national survey. Curr Med Res Opin. 2014 Jan;30(1):149–60.
4. Dowell D, Ragan KR, Jones CM, Baldwin GT, Chou R. CDC Clinical Practice Guideline for Prescribing Opioids for Pain - United States, 2022. MMWR Recomm Rep. 2022 Nov 4;71(3):1–95.
5. Horn R, Hendrix JM, Kramer J. Postoperative Pain Control. [Updated 2024 Jan 30]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan. Available from: https://www.ncbi.nlm.nih.gov/books/NBK544298/.
6. National Academies of Sciences E, and Medicine; Health and Medicine Division; Board on Health Sciences Policy; Committee on Pain Management and Regulatory Strategies to Address Prescription Opioid Abuse. Pain Management and the Intersection of Pain and Opioid Use Disorder. In: Phillips JK, Ford MA, Bonnie RJ, eds. Pain Management and the Opioid Epidemic: Balancing Societal and Individual Benefits and Risks of Prescription Opioid Use: Washington (DC): National Academies Press (US); 2017 Jul 13. 2. Available from: https://www.ncbi.nlm.nih.gov/books/NBK458655/.
7. O'Neill A, Lirk P. Multimodal Analgesia. Anesthesiol Clin. 2022 Sep;40(3):455–68.
8. Gan TJ. Poorly controlled postoperative pain: prevalence, consequences, and prevention. J Pain Res. 2017 Sep 25;10:2287–98.
9. Zaslansky R, Rothaug J, Chapman CR, Bäckström R, Brill S, Fletcher D, et al. PAIN OUT: the making of an international acute pain registry. Eur J Pain. 2015 Apr;19(4):490–502.
10. Schnabel A, Yahiaoui-Doktor M, Meissner W, Zahn PK, Pogatzki-Zahn EM. Predicting poor postoperative acute pain outcome in adults: an international, multicentre database analysis of risk factors in 50,005 patients. Pain Rep. 2020 Jul 27;5(4):e831.
11. Komann M, Baumbach P, Stamer UM, Weinmann C, Arnold C, Pogatzki-Zahn E, et al. Desire to Receive More Pain Treatment - A Relevant Patient-Reported Outcome Measure to Assess Quality of Post-Operative Pain Management? Results From 79,996 Patients Enrolled in the Pain Registry QUIPS from 2016 to 2019. J Pain. 2021 Jun;22(6):730–8.
12. Paladini A, Rawal N, Coca Martinez M, Trifa M, Montero A, Pergolizzi J Jr, et al. Advances in the Management of Acute Postsurgical Pain: A Review. Cureus. 2023 Aug 4;15(8):e42974.
13. Carr DB, Goudas LC. Acute pain. Lancet. 1999 Jun 12;353(9169):2051–8.
14. Joshi GP, Ogunnaike BO. Consequences of inadequate postoperative pain relief and chronic persistent postoperative pain. Anesthesiol Clin North Am. 2005 Mar;23(1):21–36.
15. Kehlet H. Multimodal approach to control postoperative pathophysiology and rehabilitation. Br J Anaesth. 1997 May;78(5):606–17.
16. Breivik H. Postoperative pain management: why is it difficult to show that it improves outcome? Eur J Anaesthesiol. 1998 Nov;15(6):748–51.
17. Creswell JW. Qualitative Inquiry & Research Design: Choosing Among Five Approaches. 2nd ed. Thousand Oaks: Sage Publications, Inc; 2007.
18. Patton M. Qualitative Research and Evaluation Methods: 4th Edition. Thousand Oaks: Sage Publications, Inc; 2015.
19. Gerbershagen HJ, Aduckathil S, van Wijck AJ, Peelen LM, Kalkman CJ, Meissner W. Pain intensity on the first day after surgery: a prospective cohort study comparing 179 surgical procedures. Anesthesiology. 2013 Apr;118(4):934–44.
20. Patrick DL, Burke LB, Gwaltney CJ, Leidy NK, Martin ML, Molsen E, et al. Content validity--establishing and reporting the evidence in newly developed patient-reported outcomes (PRO) instruments for medical product evaluation: ISPOR PRO Good Research Practices Task Force report: part 2--assessing respondent understanding. Value Health. 2011 Dec;14(8):978–88.
21. Turner-Bowker DM, Lamoureux RE, Stokes J, Litcher-Kelly L, Galipeau N, Yaworsky A, et al. Informing a priori Sample Size Estimation in Qualitative Concept Elicitation Interview Studies for Clinical Outcome Assessment Instrument Development. Value Health. 2018 Jul;21(7):839–42.
22. Assarroudi A, Heshmati Nabavi F, Armat MR, Ebadi A, Vaismoradi M. Directed qualitative content analysis: the description and elaboration of its underpinning methods and data analysis process. J Res Nurs. 2018 Feb;23(1):42–55.
23. Chou R, Gordon DB, de Leon-Casasola OA, Rosenberg JM, Bickler S, Brennan T, et al. Management of Postoperative Pain: A Clinical Practice Guideline From the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists' Committee on Regional Anesthesia, Executive Committee, and Administrative Council. J Pain. 2016 Feb;17(2):131–57.
24. Apfelbaum JL, Chen C, Mehta SS, Gan TJ. Postoperative pain experience: results from a national survey suggest postoperative pain continues to be undermanaged. Anesth Analg. 2003 Aug;97(2):534–40.
25. Ladha KS, Neuman MD, Broms G, Bethell J, Bateman BT, Wijeysundera DN, et al. Opioid Prescribing After Surgery in the United States, Canada, and Sweden. JAMA Netw Open. 2019 Sep 4;2(9):e1910734.
26. Buvanendran A, Fiala J, Patel KA, Golden AD, Moric M, Kroin JS. The Incidence and Severity of Postoperative Pain following Inpatient Surgery. Pain Med. 2015 Dec;16(12):2277–83.