Keywords
Primary central nervous system lymphoma, Neurotoxicity, WBRT, HDR-WBRT
Abbreviations
DBCL: Diffuse B-Cell Lymphoma; FFNT: Freedom from Neurotoxicity; HDR-WBRT: Hippocampal Dose Reduce Whole Brain Radiation Therapy; HD-MTX: High-Dose Methotrexate; hdWBRT: Higher-dose WBRT; IMRT: Intensity Modulated Radiotherapy; MTX: Methotrexate; PCNSL: Primary Central Nervous System Lymphoma; RT: Radiotherapy; VMAT: Volumetric Arc Therapy; WBRT: Whole Brain Radiotherapy
Case Report
Primary central nervous system lymphoma (PCNSL) is a rare and aggressive extranodal Non Hodgkin Lymphoma. Combined modality treatment with high-dose methotrexate (HD-MTX) followed by whole brain radiotherapy (WBRT) has been a commonly used treatment approach. While this combined modality treatment has shown to offer favourable treatment responses, it has a risk of increased treatment-related neural toxicity particularly for older patients; with a rate of around 26% in patients younger less than sixty years old and 75% in patients over 60 years [1].
Various strategies have been used to decrease neurotoxicity while maintaining high treatment response. These include using chemotherapy as induction as well as consolidation without the use of WBRT [2], using high dose chemotherapy followed by autologous stem cell transplant, reducing the dose WBRT following induction chemotherapy and avoiding radiation injury to the neural progenitor cells in the hippocampal region [3,4,6].
The clinical efficacy and toxicity profile between patients treated with higher-dose WBRT (hdWBRT) of >23.4Gy and reduced-dose WBRT (rdWBRT) of <23.4Gy has shown a favourable 3-year freedom from neurotoxicity (FFNT) for patients who received rdWBRT [5]. Patients aged more than 60 years treated with rdWBRT had a 3-year FFNT rate of 87.5% as compared to 39.1% in patients treated with hdWBRT. No neurotoxicity was observed in patients younger than 60 years treated with rdWBRT. Similarly, Shah et. al showed that patients with PCNSL who achieved a complete response (CR) with induction chemotherapy (rituximab, MTX, procarbazine, and vincristine [R-MPV]) treated consolidative rdWBRT of 23.4Gy was associated with high response rates, long-term disease control, and no reported treatment-related neurotoxicity, lending support for this approach [6]. Patients with an incomplete response to chemotherapy are currently treated with higher doses of radiotherapy, which is associated with increased neurotoxicity, with either 45 Gy WBRT or 36 Gy with additional 9 Gy to residual disease [3].
Another strategy to reduce WBRT related neurotoxicity includes avoiding radiation dose delivery to the hippocampal region where neural progenitor cells are located. Neural progenitor cells including neural stem cells which are located in the sub-granular zone of the hippocampal dentate gyrus are particularly sensitive to radiation damage. Injury to the neural stem cell compartment is thought to be responsible for the pathogenesis of radiation-induced early cognitive decline [8]. Using advanced conformal radiation techniques such as intensity modulated radiotherapy (IMRT), helical tomotherapy or volumetric arc therapy (VMAT), neural progenitor cells in the hippocampi can be spared higher doses of radiation thus preserving cognitive function and quality of life [9]. A recent phase III study comparing patients with brain metastasis treated with WBRT avoiding the hippocampal region compared with patient treated with WBRT without hippocampal sparing demonstrated that patients receiving the former treatment showed better cognitive function preservation [10].
Taking the above into consideration, it is feasible, using current clinical protocols and present-day technology to alter turmoricidal doses of radiotherapy to residual disease and at the same time reduce neurotoxicity by reducing radiotherapy doses to unaffected parts of the brain, in particular the hippocampi. Illustrating the above, two immunocompetent patients with biopsy proven PCNSL and who did not achieve complete response after completing HD-MTX chemotherapy were treated with consolidation radiotherapy with hippocampal dose reduce whole brain radiation therapy (HDR-WBRT). Patient A is a 62 year-old female presented with right sided weakness. An MRI brain scan showed a 2.6 x 2.0 cm left parietal lobe lesion. Patient B is a 59 year-old female who presented with left lower limb weakness, poor memory, behavioural changes and impaired executive function. A 3.3 x 4.1 cm mass lesion involving bilateral frontal lobes was found on MRI scanning. Stereotactic biopsy of the lesions for both the patients showed diffuse B-cell lymphoma (DBCL), ABC subtype histology.
Both patients had residual disease after completing 9 weeks of induction chemotherapy using R-MPV (Rituximab, methotrexate, procarbazine and vincristine) in April 2015 and January of 2018 respectively. Both patients subsequently received radiotherapy using a 3-phase Volumetric Arc Therapy (VMAT) plan, delivering 23.4Gy to the hippocampi, 36Gy to the rest of the brain, and 45Gy to the residual disease at 1.8Gy per fraction. Bilateral hippocampal contours were manually outlined on the fused MRI-CT image set and expanded 5mm to generate the hippocampal avoidance regions. Axial MRI scans of the brain with axial slices thickness ≤1.5mm were fused to a radiotherapy-planning head CT scan with axial slice thickness ≤ 2.5mm (Figure 1, Table 1) [7].

Figure 1: Treatment plan of Patient B who received HDR-WBRT technique. Dose colour wash transverse and sagittal images showing different radiation dose distribution with tumour-bed region (within red line), dose reduced region around the hippocampi region (yellow line) and the rest of the brain.
|
Target |
Dose Metric |
Patient A , Gy |
Patient B, Gy |
|
PTV 45 Gy |
D95 % |
45.0 Gy |
45.0 Gy |
|
|
D2 cc |
46.7 Gy |
47.4 Gy |
|
PTV 36 Gy |
D95 % |
35.2 Gy |
33.1 Gy |
|
|
D90 % |
37.5 Gy |
34.9 Gy |
|
PTV 23.4 Gy |
D95 % |
33.7 Gy |
34.5 Gy |
|
OARs |
|
|
|
|
Hippocampus L |
D100% |
20.9 Gy |
21.9 Gy |
|
|
D0.03 cc |
26.5 Gy |
25.9 Gy |
|
|
Dmean |
22.44 Gy |
24.0 Gy |
|
Hippocampus R |
D100% |
20.6 Gy |
22.0 Gy |
|
|
D0.03 cc |
24.0 Gy |
25.9 Gy |
|
|
Dmean |
21.9 Gy |
23.6 Gy |
|
Chiasm |
D0.03 cc |
36.3 Gy |
40.3 Gy |
|
Optic Nerve L |
D0.03 cc |
37.8 Gy |
38.5 Gy |
|
Optic Nerve R |
D0.03 cc |
37.9 Gy |
38.2 Gy |
|
Eye L |
Dmean |
23.1 Gy |
24.5 Gy |
|
Eye R |
Dmean |
23.7 Gy |
25.8 Gy |
|
Lens L |
D0.03 cc |
11.9 Gy |
11.7 Gy |
|
Lens R |
D0.03 cc |
11.7 Gy |
11.5 Gy |
|
Brainstem |
D0.03 cc |
38.1 Gy |
37.9 Gy |
|
Cochlear L |
Dmean |
37.1 Gy |
36.2 Gy |
|
Cochlear R |
Dmean |
36.9 Gy |
35 Gy |
|
Abbreviations: PTV: Planning Target Volume; OARs: Organs at Risk; D x Gy: Dose received by the specified x volume (%/cc); Dmean: Mean Dose |
|||
Both patients tolerated radiotherapy well with minimal side effects and no complaints. Specifically, there was no fatigue or neurological toxicity reported. They were last followed up at the clinic at 51 months and 19 months respectively with the latest MRI scan of the brain. MRI brain scans of both patients showed no tumour recurrence. Both patients were in clinical remission and have achieved good recovery in their performance status. There was no change of their cognitive function based on pre and post WBRT mini-mental state testing using Chinese Mini Mental Examination Questionnaire used in our department [10] (Figure 2).
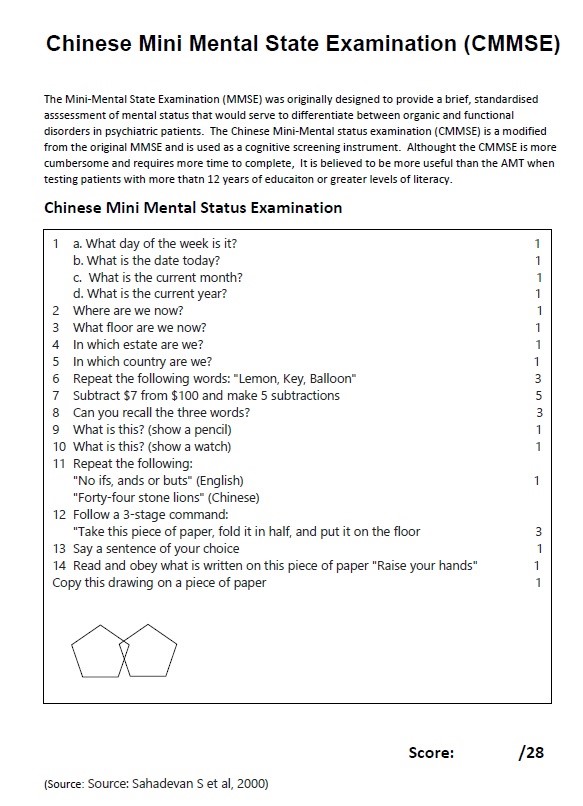
Figure 2:
This novel method of HDR-WBRT has demonstrated that adequate doses for the treatment of residual and microscopic disease can be achieved whilst minimising the risk of neurotoxicity by delivering lower doses to the hippocampi. These findings therefore warrant larger prospective clinical trials to investigate the utility of this approach to complement systemic treatment in the evolving treatment landscape for this condition.
Competing Interests
The authors declare that they have no competing interests.
Author Contributions
KW Yeoh, FY Yong, and KH Wong drafted the paper. KW Yeoh, CLM Chua, KP Chan, M Ghani, LK Ong, T Swaminathan carried out the radiotherapy planning, dosimetric study and interpretation. KW Yeoh conceived of the study and drafted the manuscript with CLM Chua, FY Yong, KH Wong. KW Yeoh, CLM Chua participated in the management of the patient and KW Yeoh and CLM Chua participated in the design of the study. All authors read and approved the final manuscript.
References
2. Rubenstein JL, Hsi ED, Johnson JL, Jung SH, Nakashima MO, Grant B, et al. Intensive chemotherapy and immunotherapy in patients with newly diagnosed primary CNS lymphoma: CALGB 50202 (Alliance 50202). J Clin Oncol. 2013;31:3061-3068.
3. Ferreri AJ, Cwynarski K, Pulczynski E, Ponzoni M, Deckert M, Politi LS, et al. Chemoimmunotherapy with methotrexate, cytarabine, thiotepa, and rituximab (MATRix regimen) in patients with primary CNS lymphoma: results of the first randomisation of the International Extranodal Lymphoma Study Group-32 (IELSG32) phase 2 trial. Lancet Haematol. 2016 May;3(5):e217-27.
4. Omuro A, Correa DD, DeAngelis LM, Moskowitz CH, Matasar MJ, Kaley TJ, et al. R-MPV followed by high-dose chemotherapy with TBC and autologous stem-cell transplant for newly diagnosed primary CNS lymphoma. Blood. 2015;125:1403-1410.
5. Lee TH, Lee JH, Chang JH, Ye SJ, Kim TM, Park CK, et al. Reduced-dose whole-brain radiotherapy with tumor bed boost after upfront high-dose methotrexate for primary central nervous system lymphoma. Radiat Oncol J. 2020;38(1):35-43.
6. Shah GD, Yahalom J, Correa DD, Lai RK, Raizer JJ, Schiff D, et al. Combined immunochemotherapy with reduced whole-brain radiotherapy for newly diagnosed primary CNS lymphoma. J Clin Oncol. 2007;25(30):4730-4735. Erratum in: J Clin Oncol. 2008 Jan 10;26(2):340.
7. Gondi V, Pugh SL, Tome WA, Caine C, Corn B, Kanner A, et al. Preservation of memory with conformal avoidance of the hippocampal neural stem-cell compartment during whole-brain radiotherapy for brain metastases (RTOG 0933): a phase II multi-institutional trial. J Clin Oncol. 2014;32:3810-6.
8. Kazda T, Jancalek R, Pospisil P, Sevela O, Prochazka T, Vrzal M, et al. Why and how to spare the hippocampus during brain radiotherapy: the developing role of hippocampal avoidance in cranial radiotherapy. Radiat Oncol. 2014 Jun 16;9:139.
9. Brown PD, Gondi V, Pugh S, Tome WA, Wefel JS, Armstrong TS, et al. Hippocampal avoidance during whole-brain radiotherapy plus memantine for patients with brain metastases: phase III trial NRG oncology CC001. J Clin Oncol. 2020 Apr 1;38(10):1019-1029.
10. Sahadevan S, Lim PP, Tan NJ, Chan SP. Diagnostic performance of two mental status tests in the older Chinese: influence of education and age on cut-off values. Int J Geriatr Psychiatry. 2000;15:234-41.