Abstract
Rheumatoid arthritis is a chronic autoimmune inflammatory disease causing joint pain, swelling, destruction and premature death. This minireview summarizes the clinically relevant information on classification, assessment of disease activity and functional status and gives a synopsis of the current ACR and EULAR recommendations for the management and treatment of RA.
Introduction
This minireview focuses on clinically relevant information on how to assess and treat patients with rheumatoid arthritis based on a synopsis of the current ACR and EULAR management recommendations. Comprehensive summary of all relevant new developments is beyond the scope of this minireview.
Definition and Epidemiology
Rheumatoid arthritis (RA) is a chronic disease of yet unknown etiology causing joint tenderness, swelling, destruction and premature death. Extraarticular manifestations such as cervical spine involvement, bursitis, tendovaginitis, rheumatoid nodules, rheumatoid vasculitis, pulmonary fibrosis, and accelerated atherosclerosis - to name a few – may occur [1]. Autoantibodies such as rheumatoid factor and anti-citrullinated protein antibody (ACPA) as well as elevated inflammation parameters such as erythrocyte-sedimentation rate and C-reactive protein characterize RA as an autoimmune-mediated systemic inflammatory process. About 0.5-1% of the adult population is afflicted with RA with female predominance and rising incidence among the elderly [2].
Classification Criteria
The goal of developing classification criteria to enable stratification of patients with and without RA even at an early stage was pursued by the 2010 Rheumatoid Arthritis classification criteria as a collaborative initiative of the American College of Rheumatology (ACR) and European League Against Rheumatism (EULAR). Applying these criteria helps to recruit standardized patient populations for clinical studies. These criteria are not intended for use as diagnostic criteria. With considerable variability of clinical manifestations, diagnosis is a clinical decision established by the experienced physician. Thus, the entry criterion of the 2010 RA classification criteria in a patient is at least one joint with definite clinical synovitis and with this synovitis not better explained by another disease. Especially the latter point needs to be emphasized since the specificity of the score itself is only about 0.74 [3]. Other diseases such as SLE, peripheral spondyloarthritis or virus-associated arthritis may be mistaken for RA if the aforementioned criterion of exclusion is being ignored.
Prerequisites:
1. At least one joint with definite clinical synovitis
2. Synovitis not better explained by other disease
|
Joint involvement |
|
|
1 large joint* |
0 |
|
2-10 large joints |
1 |
|
1-3 small joints** |
2 |
|
4-10 small joints |
3 |
|
>10 joints |
5 |
|
Serology |
|
|
Negative RF and negative ACPA |
0 |
|
Low-positive RF or low-positive ACPA |
2 |
|
High-positive RF or high-positive ACPA |
3 |
|
Acute-phase reactants |
|
|
Normal CRP and normal ESR |
0 |
|
Abnormal CRP or Abnormal ESR |
1 |
|
Duration of symptoms |
|
|
<6 weeks |
0 |
|
≥6 weeks |
1 |
|
RF: Rheumatoid Factor; ACPA: Anti-citrullinated Protein Antibodies; CRP: C-reactive Protein; ESR: Erythrocyte Sedimentation Rate RA is considered likely for patients reaching an overall score of ≥6 points. *large joints: ankle, knee, hip, shoulder, elbow **small joints: MCP II-V, PIP I-V joints of hands, wrists, MTP II-V PIP I-V of the feet |
|
Disease activity and outcome measurement
With growing numbers of disease modifying anti-rheumatic drugs (DMARDs), remission is nowadays the primary goal with low-disease activity being the best possible alternative target [3,4]. For standardized and reproducible monitoring of disease activity at a certain point and over time composite scores such as DAS28, simple disease activity index (SDAI) and Crohn's disease activity index are recommended by the ACR and EULAR with Boolean-based or SDAI based definition of remission. By Boolean based definition, patients are considered in remission if the tender joint count TJC28, the swollen joint count SJC28, CRP (in mg/dl) and patient global assessment (0–10 scale) are all ≤1. By index based definition, patients in remission present an SDAI score <3.3.
DAS28 < 2,6 should not be considered remission any longer since the DAS28 based-definition does not exclude progressive, destructive disease [5].
Patient outcome
To monitor the patient’s functional status over time, the ACR recommends the use of the PROMIS (patient-reported outcomes measurement information system) PF10a-score, the Multidimensional health assessment questionnaire (MDHAQ)or the HAQII [6]. The PF-10a is a 10-item questionnaire. Raw scores range from 10 to 50 and are translated into T-scores. A higher PROMIS-PF10a T-score represents better physical function [7]. The HAQ is a questionnaire containing 34 items in five main dimensions. Scores range from 0 to 3, with higher scores reflecting greater functional limitations [8]. The HAQII was validated to simplify the HAQ using 10 items only [9].
Treatment Principles
Remission, as mentioned and defined above, is the main therapeutic target in every patient with RA both in current European and American guidelines. If remission is not achievable, low-disease activity is the alternative. Therefore, the principle of “Treat to Target” (T2T) is the basis of both the 2015 ACR guideline as well as the 2019 EULAR recommendations [10,11]. This presupposes repeated and continued evaluation of the individual patient’s response and disease activity using Boolean criteria or SDAI and modifying or escalating therapy if remission or at least low disease activity is not achieved. Both guidelines highlight that - despite providing algorithms to simplify therapy decisions in clinical practice - individual patient circumstances and comorbidities have to be considered.
2015 ACR Guideline
The current ACR guidelines were published in 2015 (Figure 1); an updated version is scheduled for publication in 2020.

T2T Checkpoint: Evaluation of treat-to-target success. If the disease activity is remission or low, continue current treatment and consider tapering later on. If not, proceed as depicted.
csDMARD: MTX, sulfasalazine, leflunomide, hydroxychloroquine.
bDMARD: TNF-inhibitors such as adalimumab, infliximab, etanercept and non-TNF-inhibitors such as abatacept, rituximab, tocilizumab.
Figure 1: ACR flow chart (cf.[11]), simplified by the authors.
The ACR guideline differentiates between early RA in patients presenting symptoms for less than 6 months and established RA >6 months, respectively. T2T is strongly recommended even though no specific time frame to achieve the target is defined. Key provisions and principles are the focus on common clinical scenarios, cost is considered but cost-effectiveness considerations were not conducted. Disease activity and functional status assessments, respectively, should repeatedly be performed. Treatment switch in low-disease activity or remission is at the discretion of the physician in consultation with the patient but not based on an insurance policy. Medication strategies are organized in more or less favorite strategies.
Regardless of the current disease activity, the guideline recommends starting with a conventional synthetic DMARD (csDMARD) monotherapy, preferably Methotrexate (MTX). If disease activity continues to be moderate to high, a combination of two csDMARDs, a biologic DMARD (bDMARD) or the JAK-inhibitor tofacitinib are suggested. Co-administration of MTX - although being optional - is recommended over biologic monotherapy. In case of persisting moderate to high disease activity an elaborated system of possible options of different bDMARDs and tofacitinib, respectively, is recommended.
EULAR guideline with 2019 update
The current EULAR RA management recommendations are represented (simplified by the authors) in (Figure 2).
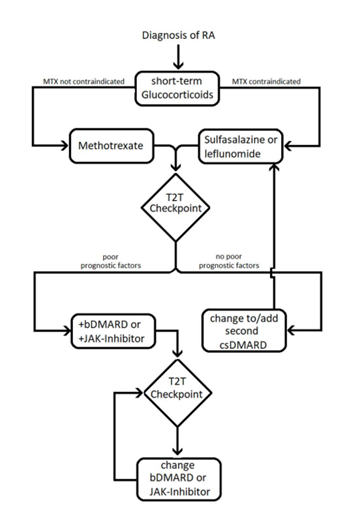
T2T Checkpoint: Evaluation of treat-to-target success. Improvements are expected after 3 months, remission after 6 months. If the targets are met, continue current treatment and consider tapering later on. If not, proceed as depicted.
Figure 2: Simplified EULAR flow chart [10].
Several overarching principles such as the aim for best care, shared decision making by the patient and the rheumatologist, being the specialist who primary cares for RA patients, consideration of disease activity, safety, patient factors such as comorbidities and structural damage are defined. Patients require access to multiple drugs with multiple successive therapies throughout their life. Cost aspects need to be considered by the rheumatologist.
An emphasis of the European guideline is on early diagnosis and treatment as the early course has proven to be decisive for the further prognosis of the disease. Core principles are the target of remission or low disease activity with tight control of the patient’s clinical response every 4-12 weeks. Unlike the ACR recommendations, there is no differentiation between early and established RA.
MTX should, if not contraindicated, be the first choice after clinical diagnosis, continuously escalating dosage to a weekly dose of about 0.3 mg/kg within 4-6 weeks. This would typically result in weekly doses of 20-25 mg in the Western hemisphere (while in Asia the maximum dose will be considerably lower). Folic acid supplementation is part of the MTX-therapy [10]. At 3 months of treatment, an improvement of at least 50% in disease activity should be achieved. Remission or, if remission is unlikely, low activity should be obtained after 6 months. Otherwise, changes to the current medication are necessary, considering individual prognostic factors:
Without poor prognostic factors, changing to or adding of another csDMARD such as leflunomide or sulfasalazine is recommended. If poor prognostic factors (high levels of RF/ACPA, high disease activity, early joint damage or failure of > 2 csDMARDs) are present, biological DMARDs (bDMARD) or tsDMARDs (JAK-inhibitors) should be added while continuing the csDMARD. If csDMARDs cannot be co-administered, monotherapy with IL6- or JAK-inhibitors may have advantages over other biologicals. If the target will still not be achieved, changing the bDMARD/JAK-inhibitor to another substance has to be considered.
2015 ACR Guideline versus 2019 EULAR Guideline – Similarities and Differences
Whereas the title “guideline” (ACR) and “recommendations” (EULAR) imply a differing strength and necessity to comply with these recommendations both provide consensus and orientation on the management of RA and “do not dictate the care of a particular patient”[4].
A comparison of these two sets of recommendations is hampered by different factors: The ACR guideline is four years older, thus misses new drugs and developments such as the increasing number of JAK-inhibitors available and the availability of biosimilars. The ACR guideline additionally addresses use of vaccines, screening for tuberculosis, laboratory monitoring and treatment in high-risk populations (i.e. patients with hepatitis, heart failure, malignancy and serious infections) and provides weighted recommendations for individual patient constellations.
However, the similarities in general are abundant: Shared decision, treat to target, repeated evaluation of the patient’s status (disease activity, functional status, comorbidities etc.), adjustment of therapy according to the individual patient’s situation, short-term use of glucocorticoids (GC), escalation as well as de-escalation strategies.
In our view, there are some differences we think are worthwhile noting:
- In contrast to the ACR, EULAR defines prognostic factors, whose absence or presence trigger different therapy algorithms (Figure 2).
- The EULAR stresses that MTX has to be given in adequate doses, whereas the ACR does not define a target dose of MTX.
- While both recommend the use of bDMARDs in combination with csDMARD the EULAR states that IL6-inhibitors and tsDMARDs “may have some advantage compared with other bDMARDs” (Recommendation 9), while the ACR prefers TNFi monotherapy over tofacitinib monotherapy (albeit with low level of evidence and due to shorter experience with tofacitinib in 2015, Recommendation 5 early RA).
In 2020, the new ACR guideline will be published which will certainly again enrich our clinical decision-making.
Implications of the Covid-19 Pandemic
The current COVID-19 pandemic has raised concerns in both patients and physicians about the management of RA with RA patients being at an increased risk of serious infections. First data from the German Covid-19 inflammatory rheumatic diseases (IRD) registry show that older age (>65 years), cardiovascular comorbidity and prior or current treatment with GC are risk factors for COVID-19 related hospitalizations and that male gender is probably a risk factor for a more severe course of COVID-19 [12]. Very recent data from Spain seem to support the continuation of bDMARDs and tsDMARDs during the Covid-19 pandemic [13].
Currently, the continuous use of DMARDs in RA is recommended, whereas the preemptive stop of immunosuppressive therapy is not advised due to higher risks of infections in patients with high disease activity [14-16]. GC should be used at the lowest dose possible [15]. In case of SARS-Cov-2 infection, immunosuppressants should be stopped or withheld. The role of Hydroxychloroquine and IL-6 inhibition in COVID-19 is being examined [16].
Future Directions
Important questions from the clinician’s point of view are:
- How can we avoid the development of rheumatoid arthritis, e.g. in ACPA-positive patients with arthralgia?
- How can we predict which treatment is best suited and most efficient for the individual patient with RA?
- Which treatment sequence and strategy - given the numerous options of treatment – are the most efficient with lowest side effects, risk and cost?
- When an in whom de-escalation and complete treatment withdrawal is possible without the risk of relapse?
Conclusion
Shared decision between the patient and the physician with treatment algorithms based on T2T and tight control of disease activity together with numerous new treatment options help to deliver best possible care to our patients with RA.
References
2. Scott DL, Wolfe F, Huizinga TWJ. Rheumatoid arthritis. Lancet (London, England). 2010 Sep 25;376(9746):1094-108.
3. Sakellariou G, Scirè CA, Zambon A, Caporali R, Montecucco C. Performance of the 2010 Classification Criteria for Rheumatoid Arthritis: A Systematic Literature Review and a Meta-Analysis. PLoS ONE. 2013 Feb 20;8(2).
4. Aletaha D, Neogi T, Silman AJ, Funovits J, Felson DT, Bingham CO, et al. 2010 Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis & Rheumatology. 2010 Sep;62(9):2569-81.
5. Felson DT, Smolen JS, Wells G, Zhang B, van Tuyl LHD, Funovits J, et al. American College of Rheumatology/European League Against Rheumatism provisional definition of remission in rheumatoid arthritis for clinical trials. Arthritis & Rheumatology. 2011 Mar;63(3):573-86.
6. Barber CEH, Zell J, Yazdany J, Davis AM, Cappelli L, Ehrlich-Jones L, et al. 2019 American College of Rheumatology Recommended Patient-Reported Functional Status Assessment Measures in Rheumatoid Arthritis. Arthritis Care & Research. 2019;71(12):1531-9.
7. Wahl E, Gross A, Chernitskiy V, Trupin L, Gensler L, Chaganti K, et al. Validity and Responsiveness of a 10-Item Patient-Reported Measure of Physical Function in a Rheumatoid Arthritis Clinic Population. Arthritis Care & Research. 2017;69(3):338-46.
8. Fries JF, Spitz P, Kraines RG, Holman HR. Measurement of patient outcome in arthritis. Arthritis & Rheumatology. 1980 Feb;23(2):137-45.
9. Wolfe F, Michaud K, Pincus T. Development and validation of the health assessment questionnaire II: a revised version of the health assessment questionnaire. Arthritis & Rheumatology. 2004 Oct;50(10):3296-305.
10. Smolen J, Landewé R, Bijlsma J, Burmester G, Dougados D, Kerschbaumer A, et al. EULAR Recommendations for the Management of Rheumatoid Arthritis With Synthetic and Biological Disease-Modifying Antirheumatic Drugs: 2019 Update. Annals of the Rheumatic Diseases. 2020 Jan 22.
11. Singh JA, Saag KG, Bridges SL, Akl EA, Bannuru RR, Sullivan MC, et al. 2015 American College of Rheumatology Guideline for the Treatment of Rheumatoid Arthritis. Arthritis & Rheumatology. 2016;68(1):1-26.
12. Regierer A, Hasseli R, Hoyer B, Krause A, Lorenz HM, Pfeil A, et al. Co0004 Older Age, Cardiovascular Comorbidity and Glucocorticosteroids Are Risk Factors for Covid-19 Hospitalisation in Patients with Inflammatory Rheumatic Diseases: First Results of the German Covid-19-Ird Registry. Annals of the Rheumatic Diseases. 2020 Jun 1;79(Suppl 1):215-6.
13. Gonzalez C, Viso LAM, Rodríguez OB, Alonso AH, Rodríguez CL, Nieto JC, et al. Co0003 Treatment with Biological Therapies and Risk of Being Admitted to the Hospital for Covid19 Infection. Annals of the Rheumatic Diseases. 2020 Jun 1;79(Suppl 1):214-5.
14. Favalli E, Ingegnoli F, De Lucia O, Cincinelli G, Cimaz R, Caporali R. COVID-19 Infection and Rheumatoid Arthritis: Faraway, So Close! Vol. 19, Autoimmunity reviews. Autoimmune Reviews; 2020.
15. Mikuls TR, Johnson SR, Fraenkel L, Arasaratnam RJ, Baden LR, Bermas BL, et al. American College of Rheumatology Guidance for the Management of Rheumatic Disease in Adult Patients During the COVID-19 Pandemic: Version 1. Arthritis & Rheumatology. 2020 Apr 29;online version ahead of print.
16. Deutsche Gesellschaft für Rheumatologie e.V. [Internet]. DGRh e.V. [cited 2020 Jun 21]. Available from: https://dgrh.de/Start/Publikationen/Empfehlungen/Therapie-bei-besonderen-Situationen/Empfehlungen-w%C3%A4hrend-der-SARS-CoV-2-Covid-19-Pandemie.html.