Abstract
Diabetic foot ulcers account for 70-80% of all ulcer cases, with this proportion rising to 21–27% in developing countries. The associated mortality rate ranges from 3.75% to 58.8%. Initially, diabetic foot conditions are often life-threatening and require immediate resuscitation, along with various surgical treatments such as debridement or split-thickness skin grafting, depending on factors like the size, location, and depth of the wound. We explore the role of CAMPS in wound bed preparation of diabetic foot ulcers.
Keywords
CAMPs, Diabetic foot, Wound bed preparation
Introduction
Diabetic foot remains a significant global health issue, particularly among the elderly and immunocompromised individuals, who are at higher risk. Patients with poorly controlled blood sugar levels are more susceptible to developing diabetic foot ulcers. We explore the use of CAMPs (cellular, acellular, and matrix-like products) in wound bed preparation. Once critical care needs are addressed for diabetic foot patients, the focus shifts to wound management. The primary goals of ulcer management are to promote healing, restore function, and preserve appearance. The three main surgical approaches for treating diabetic foot ulcers are excision, grafting, and reconstruction. Early excision and skin grafting help remove necrotic tissue and provide an initial cover for the wound. Regenerative therapies like CAMPs play a vital role in improving healing of diabetic foot ulcers. CAMPs is an acellular dermal regeneration template made from a bilaminate sheet of cross-linked bovine tendon collagen and shark-derived glycosaminoglycans (chondroitin-6-sulfate), with a silicone cover [1]. CAMPs functions as a scaffold that promotes the growth of new dermal tissue. Blood vessels and other cells migrate into the matrix, gradually forming a new layer of skin. The silicone layer on top serves to seal the wound and prevent fluid loss [2].
Methodology
This study was conducted in a tertiary care centre in the Department of Plastic Surgery. The patient was a 69-year-old male with a non-healing ulcer on the heel of his left foot with exposed calcaneum, for a duration of 5 months. The condition initially began as a small blister before progressing into an open wound. Wound bed preparation was done and to further protect the exposed bone from damage, CAMPs was applied, containing an outer layer of semi-permeable thin silicone that acts as the epidermis. This helps to control water loss, provide a flexible adherent covering for wound surface and add increased strength. The inner layer is made of a complex matrix of ultra-pure bovine collagen and chondroitin-6-sulfate matrix that allows cell infiltration and proliferation which aids in the healing process [3-5]. This was followed by application of negative pressure wound therapy (NPWT).
Results
The raw area successfully integrated the CAMP, and the wound granulated effectively. After two weeks, the wound was grafted with autologous FTSG.
Discussion
The use of appropriate scaffold matrices is crucial for driving skin tissue regeneration. Scaffolds can come in various forms, including porous, fibrous, microsphere-shaped, hydrogel-based, composite, or acellular types. For ulcers that are difficult to heal or for larger wounds requiring coverage, skin grafting or flap procedures may be necessary, depending on the case. Skin is the most biologically suitable material for covering wounds. However, certain conditions, such as diabetic foot, can complicate the use of skin grafts, especially when there is insufficient available skin to cover the wound. In these cases, biologically effective and cost-efficient materials are needed to both cover the wound and protect against infection. CAMPs is considered a promising source of such scaffolding material.
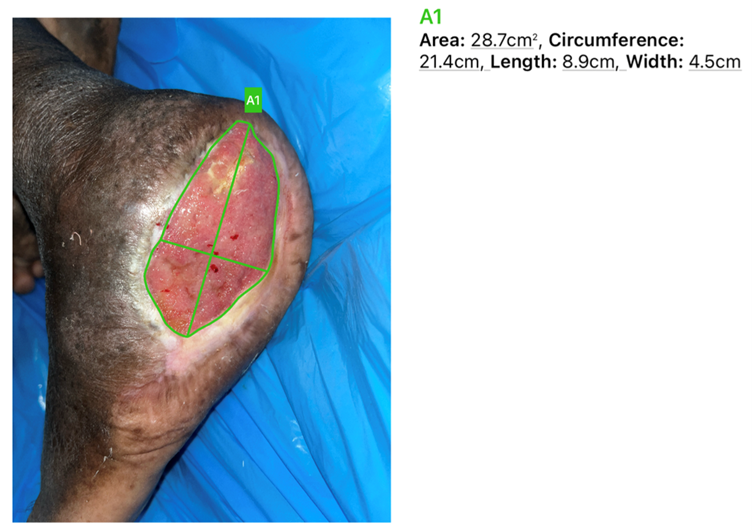
Figure 1. Diabetic foot ulcer with exposed calcaneum.

Figure 2. Application of CAMPs for wound bed preparation.

Figure 3. The wound was grafted after the application of CAMPs.
Dermal regeneration occurs in four distinct phases: imbibition, fibroblast migration, neovascularization, and remodelling/maturation. Imbibition begins within minutes, during which the matrix initially takes up fluid from the wound exudate, with fibrin playing a key role in enhancing this process. Swelling of the matrix is expected during this phase [6]. By around day seven, fibroblasts start migrating into the matrix. In the third week, myo-fibroblasts arrive and begin to deposit native collagen into the matrix. By week four, host-derived collagen becomes dominant, replacing the matrix collagen. During this time, the neodermis is initially thicker than the host dermis but gradually thins and gains flexibility through maturation [7,8]. By the end of week four, the neodermis is fully vascularized, which can be clinically observed as a color change from pink to pale yellow and then to peach. Some studies have shown that vascularization may occur within two weeks, particularly in diabetic foot patients, where accelerated vascularization could be linked to heightened metabolism and a systemic inflammatory response [9]. After vascularization, the neodermis is ready for graft placement.
Conclusion
CAMPs plays a significant role in wound bed preparation in diabetic foot ulcers. It supports and accelerates the healing process by promoting the regeneration of tissue and creates an optimal environment for further interventions, such as skin grafting.
Declarations
Authors’ contributions
All authors made equal contributions to the article.
Availability of data and materials
Not applicable.
Financial support and sponsorship
None.
Consent for publication
Not applicable.
References
2. Huang X, Ding Y, Pan W, Lu L, Jin R, Liang X, et al. A Comparative Study on Two Types of Porcine Acellular Dermal Matrix Sponges Prepared by Thermal Crosslinking and Thermal-Glutaraldehyde Crosslinking Matrix Microparticles. Front Bioeng Biotechnol. 2022 Aug 5;10:938798.
3. Thinda S, Wright HV, Mawn LA. Integra bilayer matrix wound dressing closure of large periorbital traumatic wound. Archives of Ophthalmology. 2012 Feb 1;130(2):217-9.
4. Wicks ED, Rezaie N, Gasner KA. One-stage use of integra in the management of a complex dorsal hand wound in a patient with acquired hemophilia A. Journal of Hand Surgery Global Online. 2019 Apr 1;1(2):115-8.
5. Mansour J, Nesbitt B, Khanjae S, Horowitz G, Amit M, Muhanna N, et al. The Feasibility and Outcome of Integra® Bilayer Matrix in the Reconstruction of Oral Cavity Defects. Otolaryngology–Head and Neck Surgery. 2024 Feb;170(2):373-9.
6. Sackett SD, Tremmel DM, Ma F, Feeney AK, Maguire RM, Brown ME, et al. Extracellular matrix scaffold and hydrogel derived from decellularized and delipidized human pancreas. Sci Rep. 2018 Jul 11;8(1):10452.
7. Lee YJ, Han HJ, Shim HS. Treatment of hard-to-heal wounds in ischaemic lower extremities with a novel fish skin-derived matrix. J Wound Care. 2024 May 2;33(5):348-56.
8. Simman R, Bakewell SJ, Bell D, Shuman S, Cheney M. A novel approach for the treatment of diabetic foot ulcers using a multimodal wound matrix: a clinical study. J Wound Care. 2024 Oct 2;33(10):772-7.
9. Ditmars FS, Kay KE, Broderick TC, Fagg WS. Use of amniotic membrane in hard-to-heal wounds: a multicentre retrospective study. J Wound Care. 2024 Mar 1;33(Sup3):S44-50.