Keywords
Complication, Ptosis, Facial palsy, Torticollis, Shunt
Commentary
Hydrocephalus is a life-threatening and chronic condition that can occur at any age, most often in the pediatric population. Cerebrospinal fluid diversion is necessary in dealing with most forms of hydrocephalus and ventriculoperitoneal shunt insertion is considered as one of the most commonly neurosurgical procedures for hydrocephalus management. Despite the effectiveness of shunt, it has been associated with a high rate of complications [1] including, infection, obstruction, disconnection, shunt fracture, migration of the catheters, and overdrainage. The most common reason for shunt malfunction is mechanical obstruction of the device, mostly proximal catheter blockage by choroid plexus, fibrous tissue, or tissue debris, blood or accumulation of high viscosity fluid within the catheter [2]. Distal catheter obstruction is commonly due to clogging, kinking, thrombosis, or venous occlusion [2,3].
The signs and symptoms of shunt dysfunction are related to high intracranial pressure most commonly including headache, nausea, vomiting, bulge fontanel, irritability, sunset eye. Increased ventricular diameter in comparison to prior studies, increased temporal horns width, sulcus effacement and rounding of 3rd ventricle are common findings in neuroimaging studies during shunt malfunction (Figure 1). However, stable ventricular dimensions on serial imaging studies (Figure 2) may wrongly be interpreted as normal shunt function [4].
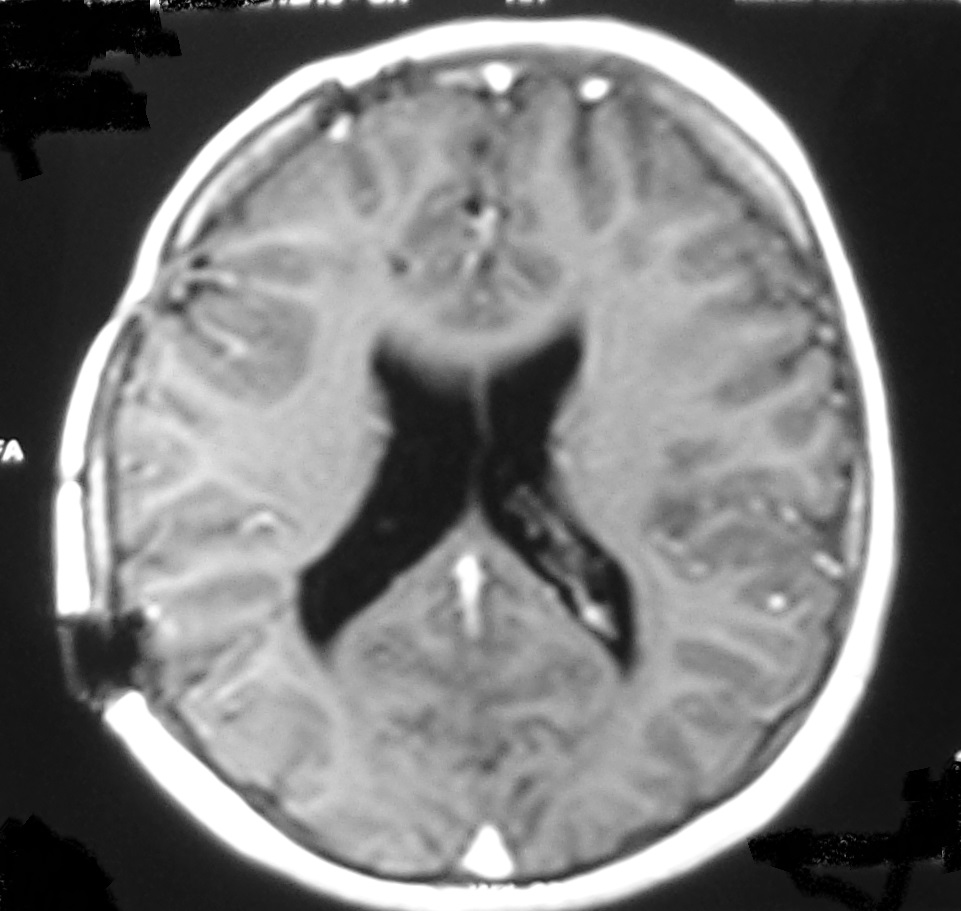

Figure 1: A. Surveillance brain MRI of a 12 year old boy with shunting due to brain tumor at age of 6. The lateral ventricles were nearly normal size and the child without any symptoms. B. The child admitted with headache vomiting and drowsiness. The brain CT scan confirms increased size of lateral ventricles with sulcus effacement.
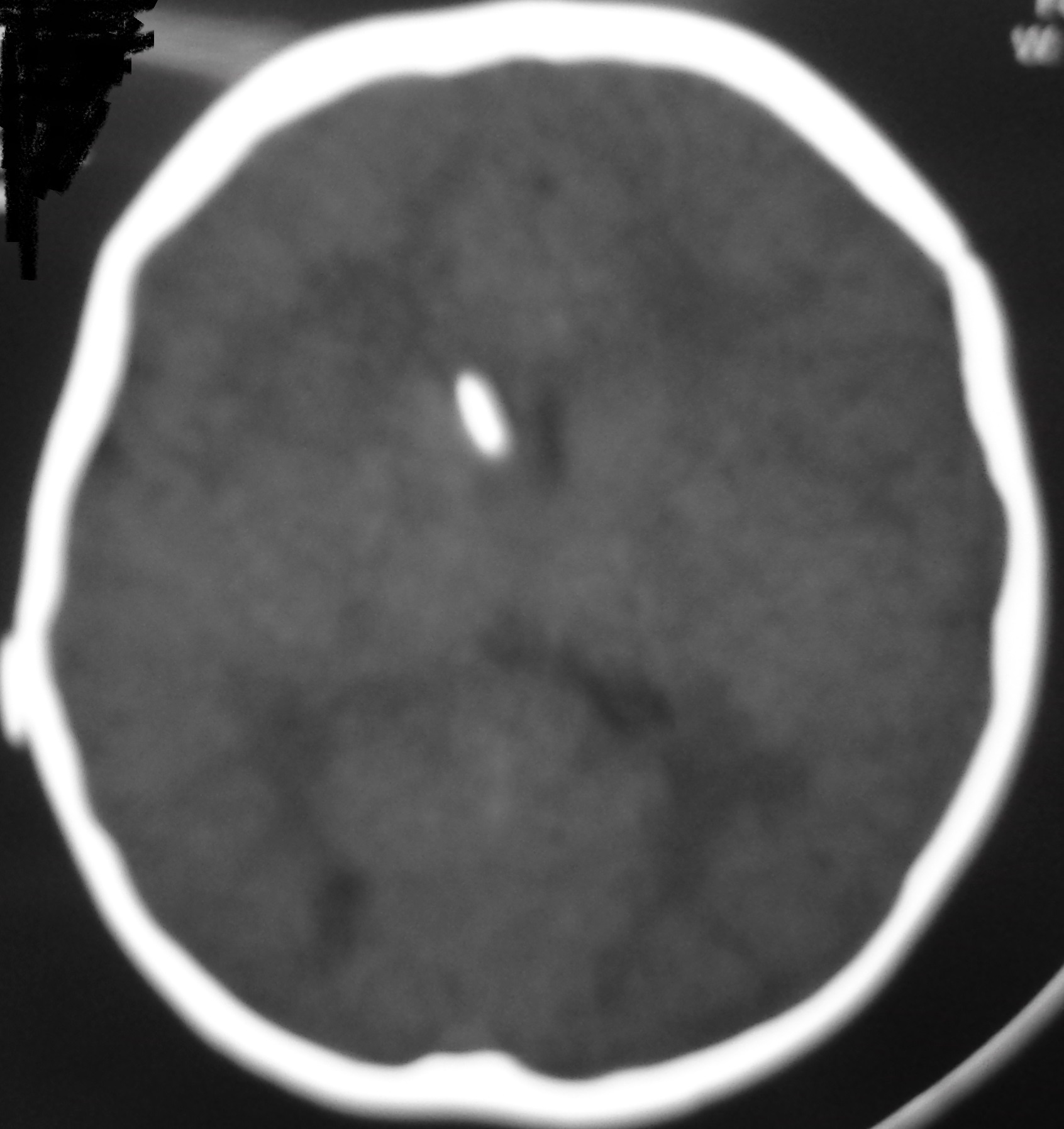

Figure 2: A. Slit like ventricle after 9 months of shunting in an infant with congenital hydrocephalus; the child was stable without any symptoms. B. One year later he was admitted with persistent vomiting and ptosis. The brain CT shows no obvious change in the size of ventricle. His symptoms were recovered after shunt revision due to proximal catheter obstruction.
Shunt malfunction is generally confirmed by a combination of shunt tap and brain CT scan. However, imaging may not demonstrate an increase in ventricular size despite dysfunctional shunt [3,4]. This condition is true particularly when shunt malfunction is intermittent.
The high intracranial pressure subsequent to shunt malfunction can be life threatening therefore the early diagnosis and emergent treatment are mandatory to decrease the risk of mortality and morbidity in patients with past history of shunt insertion.
There are rare instances in the literature with unusual or odd presentations of shunt malfunction that led to misdiagnosis or delayed diagnosis and treatment [5-7]. Knowing these rare manifestations of shunt malfunction while considering timely diagnosis and prompt surgical correction of these situations would save the patients’ lives.
We have reported several rare and unusual clinical manifestations of shunt dysfunction including facial nerve palsy, oculomotor palsy, torticollis, dystonia. The exact incidence of these odd and unusual presentations of shunt malfunction is not clear because of very rarity and most often being as case reports. Any usual symptoms of high intracranial pressure or even unusual neurological symptoms in patients with past history of shunt placement thorough investigations including brain imaging with CT scan and MRI, shunt tap, or shunt series are mandatory to rule out shunt dysfunction [3]. Shunt revision with reimplantation of prior shunt device or placement of a new shunt device or endoscopic third ventriculostomy are performed to manage the high intracranial pressure.
Clinical presentations of shunt malfunction in the pediatric population are widely varied from non-specific symptoms to severe disabling presentations and rarely very odd clinical manifestations that the exact pathophysiology is difficult to describe [8].
Notably, ventricular dilation following shunt malfunction and uncal herniation may compress the oculomotor nerve and result in oculomotor nerve palsy and ptosis [6]. Therefore, the presence of 3rd nerve dysfunction should trigger clinical suspicion of shunt malfunction in children with a history of prior shunt placement.
Although the exact pathophysiology of facial nerve palsy associated with shunt malfunction is not well known, ventricular dilation might produce a downward herniation of the brainstem and increased stretching forces applied to facial nerves, causing facial palsy [9]. In our series we noted more 7th nerve palsy in patients with Myelomeningocele and Chiari type II could be related to this mechanism. In addition, Maus et al. suggested mechanical irritation as the pathophysiology of facial nerve palsy in a patient with CSF overdrainage and intracranial hypotension [10].
On the other hand, dystonia and torticollis were odd symptoms in our patients that further assessment showed shunt malfunction as the culprit of their symptom. Shunt malfunction with increased intracranial pressure might induce lower cranial nerve dysfunction due to traction or stretching forces after hindbrain herniation [3].
Severe disabling clinical consequences of shunt failure are seizure, autonomic instability, and loss of consciousness [2]. It is suggested that increased intracranial pressure may disrupt cortical-subcortical interconnections, resulting in seizure disorder [4]. Bourgeois et al. [11] found that the average number of shunt revisions in children with seizures was significantly greater than in those who did not have seizures. There was a higher incidence of epilepsy among children who had shunt malfunction, infection, or combination of both associated with higher number of revisions.
In conclusion, shunt malfunction should be considered in any patient with a previous history of shunt placement and any new usual or unusual symptoms. Clinical examination, neuroimaging, shunt series radiography, intracranial pressure monitoring, shunt tap, close observation, are all steps that could help pediatric neurosurgeons make the most suitable decision at the right time. Because of diverse clinical presentations of shunt malfunction, this diagnosis could be delayed in the clinical setting or missed by some. As a result, a thorough examination of patients with shunt is required to ensure early and accurate diagnosis of shunt malfunction and decrease the morbidity and mortality.
The main limitation of this study is retrospective data collection related to odd and unusual presentations of shunt malfunction. A multicenter prospective study regarding the presentation, imaging study, intraoperative findings and outcome can be more informative in the future.
References
2. Bates P, Rajderkar D. Common and uncommon causes of ventriculoperitoneal shunt malfunction diagnosed on plain radiographs. Current Problems in Diagnostic Radiology. 2018 Sep 1;47(5):317-23.
3. Kankam SB, Karami S, Nejat A, Meybodi KT, Habibi Z, Nejat F. Odd presentation of shunt malfunction: a case series and review of literature. Child's Nervous System. 2023 Sep;39(9):2479-85.
4. Lucas S, Solomon G, Labar D, Chutorian A. Episodic brainstem compression masquerading as electrodecremental seizures. Journal of Child Neurology. 1994 Apr;9(2):167-9.
5. Spennato P, O’Brien DF, Fraher JP, Mallucci CL. Bilateral abducent and facial nerve palsies following fourth ventricle shunting: two case reports. Child's Nervous System. 2005 Apr;21:309-16.
6. Grossman R, Feldman Z. Bone growth causing ventriculoperitoneal shunt malfunction in a patient with osteopetrosis: case report. Journal of Neurosurgery: Pediatrics. 2004 May 1;100(5):530-1.
7. Samdani AF, Storm PB, Kuchner EB, Garonzik IM, Sciubba D, Carson B. Ventriculoperitoneal shunt malfunction presenting with pleuritic chest pain. Pediatric Emergency Care. 2005 Apr 1;21(4):261-3.
8. James HE, Nowak TP. Clinical course and diagnosis of migraine headaches in hydrocephalic children. Pediatric Neurosurgery. 1991 Mar 5;17(6):310-6.
9. Thines L, Vinchon M, Lahlou A, Pellerin P, Dhellemmes P. Facial diplegia revealing ventriculoperitoneal shunt failure in a patient with Crouzon syndrome: case report. Journal of Neurosurgery: Pediatrics. 2007 Jul 1;107(1):46-8.
10. Maus V, Petridis AK, Doukas A, Mehdorn HM. Isolated facial palsy as a hallmark of CSF overdrainage in shunted intracranial arachnoid cyst. Acta Neurochirurgica. 2011 May;153:1141-2.
11. Bourgeois M, Sainte-Rose C, Cinalli G, Maixner W, Malucci C, Zerah M, et al. Epilepsy in children with shunted hydrocephalus. Journal of Neurosurgery. 1999 Feb 1;90(2):274-81.