Abstract
Systemic sclerosis (SSc) is a heterogeneous, multisystem autoimmune disease characterized by fibrosis in genetically predisposed individuals. It can involve multiple organ systems, but hepatic involvement is rare.
In this study, we aim to find the correlation of liver disease, especially primary biliary cholangitis (PBC) and autoimmune hepatitis (AIH), in the population with SSc. Further, the correlation of anti-mitochondrial antibody (AMA) and other autoantibodies were done.
Databases were searched for liver disease in SSc, and studies were selected for analysis. Cochrane risk of bias tools and meta-analysis online were used. Controls were taken from the prevalence in the respective countries around the same time.
There was a significant association between PBC and AIH, AMA positivity, and SSc. There was no association with liver fibrosis.
Keywords
Primary biliary cholangitis, Autoimmune hepatitis, Systemic sclerosis, Anti-mitochondrial antibody
Introduction
Systemic sclerosis (SSc) is a heterogeneous, multisystem autoimmune disease characterized by fibrosis in genetically predisposed individuals. It has unclear pathogenesis but a strong predisposition in first-degree family members. It has a varying extent and often differs in clinical manifestations, skin involvement, complications, and mortality. It is more prevalent in middle-aged women, with incidence more common in North American countries. Poor prognostic factors include male gender and African American race [1].
In SSc, endothelial dysfunction and resultant microvascular damage promote tissue hypoxia and hence inflammation, including overproduction of transforming growth factor-β (TGF-β), resulting in fibrosis, which can affect the gastrointestinal tract from mouth to anus, with smooth muscle atrophy and fibrosis on biopsy. Liver involvement with this pathway is rare and seldom documented. Liver biopsy is similar to PBC, ranging from intrahepatic bile duct damage to portal inflammation, necrosis, and lymphocyte invasion [2,3].
Autoimmunity, such as through anti-mitochondrial antibodies (AMA) is a common driver of cholangiocyte activation and dysfunction as seen in primary biliary cholangitis (PBC) [2,4].
Primary biliary cholangitis, autoimmune hepatitis, and overlap syndrome are common hepatic associations with SSc [5]. A review of 35 patients with AIH identified only 2 patients with SSc. Patients with SSc have increased rates of PBC compared with the general population (2% versus 0.04%) [6,7].
In this systematic review and meta-analysis, we aim to look at studies that examine the incidence of liver disease in patients with SSc. Some of the studies also focus on the extent of liver injury, including steatosis, fibrosis, and cirrhosis.
Methods
The study aimed to observe the incidence of liver disease, associated antibodies, and degree of fibrosis in people diagnosed with scleroderma. PRISMA guidelines were followed (Figure 1).
Inclusion criteria for studies included:
- Patients aged more than 18 years
- Patients with a confirmed diagnosis of scleroderma
- Patients with pre-existing scleroderma with elevated transaminases
- Observational cohort studies, systematic reviews or meta-analyses
Exclusion criteria for the studies:
- Patients less than 18 years
- Studies focusing on multi-organ involvement
- Case reports, case series, or literature reviews were excluded
Databases explored included PubMed, PubMed Central, Scopus, Google Scholar, and Cochrane Library. MeSH terms included ("Scleroderma, Systemic"[MeSH] OR scleroderma) AND ("Liver Diseases"[MeSH] OR liver disease).
The literature search yielded 11 articles; 3 articles were duplicates and were excluded. Amongst 8 leftover articles, there were 2 literature reviews and one case report. These were excluded as well. Five articles, all observational cohort studies, were included in the study, as shown in Figure 1. The Cochrane risk of bias 2.0 tool was used, and the risk of bias calculated is shown in Figure 2.
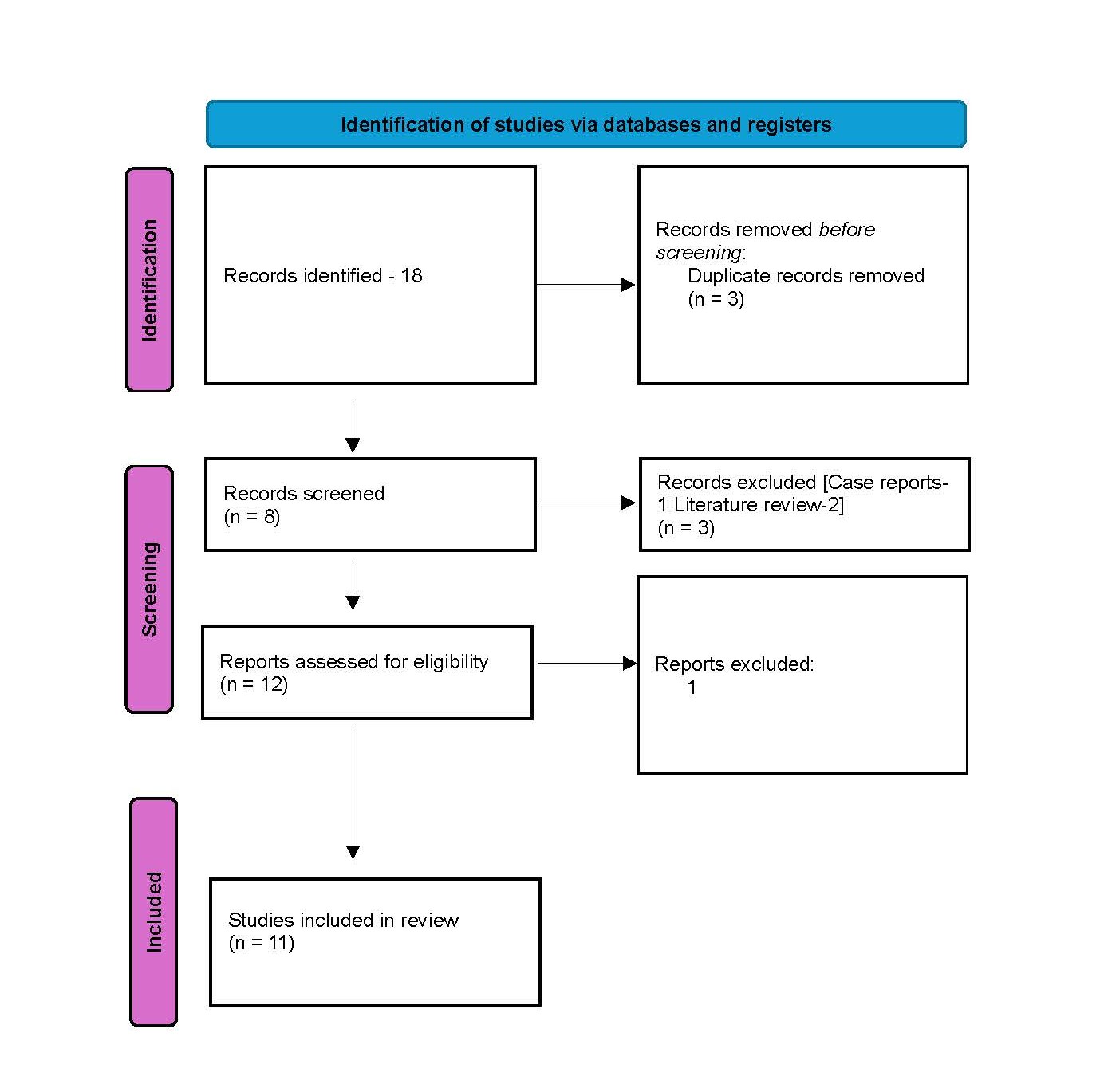
Figure. 1. PRISMA flowchart.
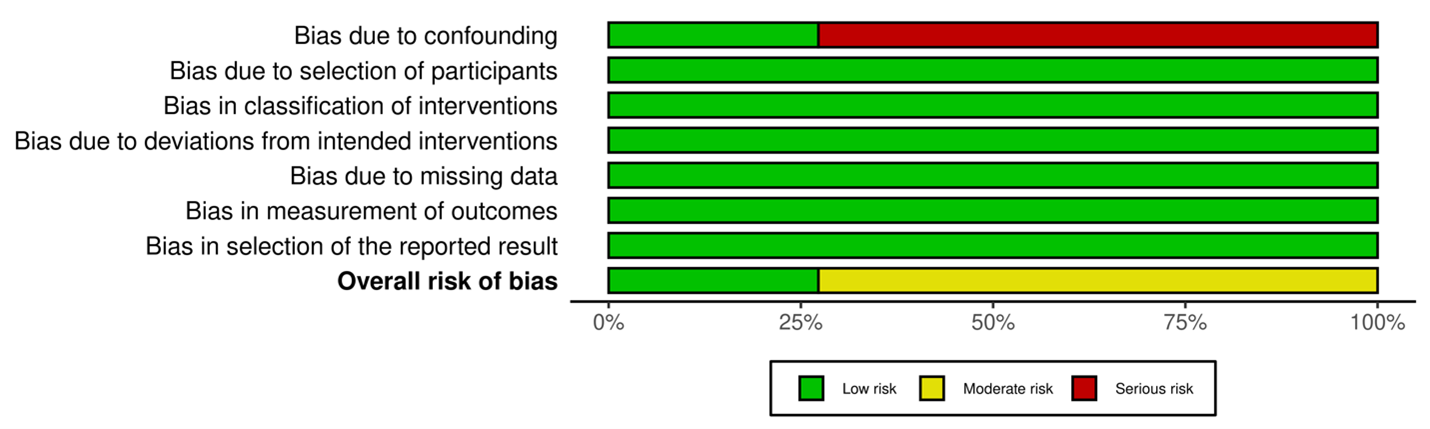
Figure 2. ROBVIS RoB
Three analyses were done. The incidence of patterns of liver injury, especially PBC, was examined. Secondly, the prevalence of different antibodies was determined. Lastly degree of fibrosis as a result of liver injury was checked. Meta-analysis online software was used to derive forest plots.
Results
Table 1 shows the name of the study, type, number of participants, year of study, and country.
|
STUDY |
AUTHOR |
TYPE |
NUMBER |
YEAR |
PLACE |
|
Clinical Relevance of Liver Involvement in the Clinical Course of Systemic Sclerosis
|
Lorena et al. [8] |
Retrospective observational cohort |
97 |
2018–2020 |
Italy |
|
Hepatobiliary involvement in systemic sclerosis and the cutaneous subsets characteristics and survival of patients from the Spanish registry
|
Alfonso et al. [9] |
Retrospective observational cohort |
1572 |
2015 |
Spain |
|
Liver Involvement in Patients with Systemic Sclerosis: Role of Transient Elastography in the Assessment of Hepatic Fibrosis and Steatosis
|
Cuomo et al. [10] |
Cross sectional |
59 |
2013 |
Italy |
|
Incidence and Predictors of an Abnormal Liver Function Test Among 674 Systemic Sclerosis Patients: A Cohort Study
|
Sawadpanich et al. [11] |
Retrospective observational cohort |
674 |
2012–2019 |
Thailand |
|
Evaluation of liver function tests in scleroderma patients |
Salem et al. [12] |
Retrospective observational cohort |
40 |
2012 |
Saudi Arabia |
|
Presence of organ specific antibodies in patients with systemic sclerosis |
Wielosz et al. [13] |
Retrospective observational cohort |
86 |
2006 |
Poland |
|
Primary biliary cirrhosis (PBC), PBC autoantibodies, and hepatic parameter abnormalities in a large population of systemic sclerosis patients |
Assassi et al. [5] |
Retrospective observational cohort |
817 |
2009 |
USA |
|
High prevalence of primary biliary cirrhosis and disease-associated autoantibodies in Japanese patients with systemic sclerosis |
Imura-Kumada et al. [14] |
Retrospective observational cohort |
225 |
2012 |
Japan |
|
Primary biliary cirrhosis-related autoantibodies in a large cohort of Italian patients with systemic sclerosis |
Cavazzana et al. [15] |
Retrospective observational cohort |
201 |
2011 |
Italy |
|
Is prevalence of PBC underestimated in patients with systemic sclerosis? |
Norman et al. [16] |
Retrospective observational cohort |
52 |
2009 |
Poland |
|
Liver autoantibodies in patients with scleroderma |
Skare et al. [17] |
Retrospective observational cohort |
63 |
2011 |
Brazil |
Table 2 shows patients who were diagnosed with liver disease. In 2 of the studies, a clear-cut diagnosis of PBC was not made, but transaminase elevation showed a cholestatic disease pattern in 37 and 14 patients, respectively. However, given the lack of formal diagnosis, it shall not be used in the calculation of prevalence in this study. Two thousand seven hundred ninety-seven patients with SSc were investigated, and 190 of them were diagnosed with liver disease. It, however, included 33 patients with alcoholic, metabolic, and viral liver disease, and the last 3 studies only studied PBC. Exclusively, 157 people had autoimmune-associated liver diseases, accounting for a 6.7% prevalence in SSc patients. PBC accounted for 5%, AIH for 1.20% (not studied in the last 3 studies, so calculated amongst studies 1 and 2). PSC was only seen in 1 patient across the studies. Figures 3 and 4 show forest plots for the prevalence of PBC and AIH, respectively in patients with SSc and general populations from the respective countries around the same time frame [18–20].
|
AUTHOR |
Number of patients with SSc |
Liver disease |
PBC |
AIH |
Others |
|
Lorena et al. [8] |
97 |
11 |
7 |
1 |
1 PSC 1 NRH 3 Viral Hepatitis 3 Alcoholic Hepatitis |
|
Alfonso et al. [9] |
1,572 |
118 |
67 AMA positive 6 AMA negative |
19 |
26 Secondary liver diseases (n = 11), SSc-related HBI (n = 7), nodular regenerative hyperplasia (n = 3), liver cirrhosis (n = 3), and HBI of unknown origin (n = 2, 0.1%) |
|
Sawadpanich et al. [11] |
674 |
430 |
Possibly 37 |
NA |
NA |
|
Salem et al. [12] |
40 |
14 |
Possibly 12 |
NA |
2 |
|
Wielosz et al. [13] |
86 |
10 |
10 |
NA |
NA |
|
Assassi et al. [5] |
817 |
16 |
16 |
NA |
NA |
|
Imura-Kumada et al. [14] |
225 |
35 |
35 |
NA |
NA |
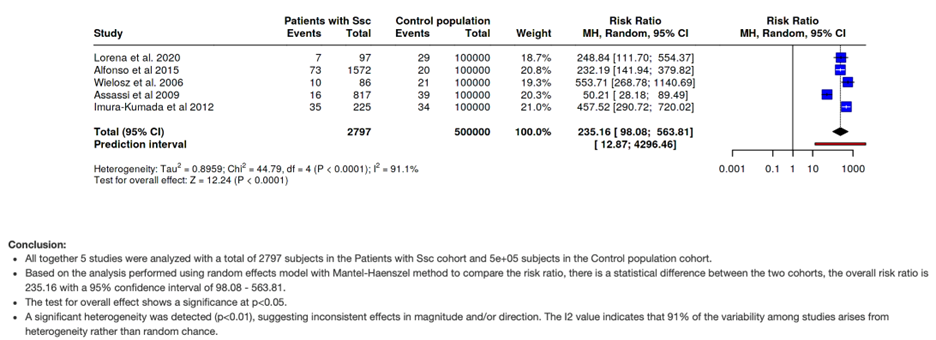
Figure 3. Prevalence of PBC in SSc compared to the general population.
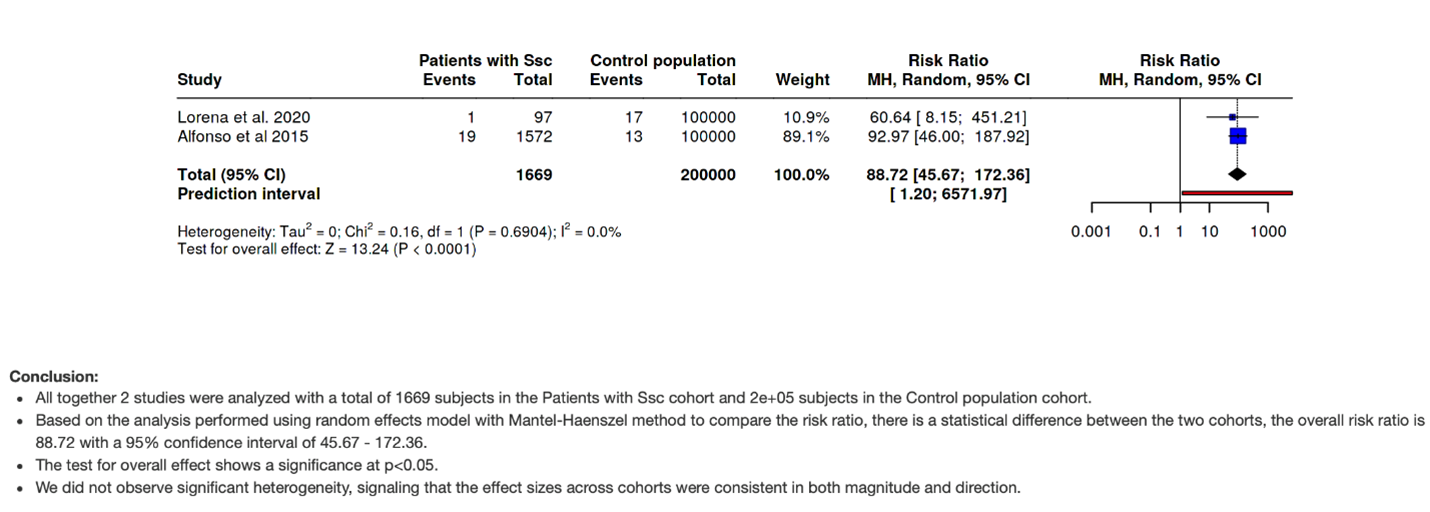
Figure 4. Prevalence of AIH in SSc compared to the general population.
The incidence of AMA positivity was 172 in 1581 patients, accounting for 10.87%, as shown in Table 3. The second most common antibody is Anti-sp100 with 3.1% positivity.
|
Author |
Number of patients with SSc |
AMA |
Others |
|
Lorena et al. [8] |
97 |
18 |
Anti SP-100- 4 Anti gp120- 1 |
|
Alfonso et al. [9] |
1572 |
NA |
NA |
|
Cuomo et al. [10] |
59 |
NA |
NA |
|
Sawadpanich et al. [11] |
674 |
NA |
NA |
|
Salem et al. [12] |
40 |
1 |
NA |
|
Wielosz et al. [13] |
817 |
56 |
sp100 -26 gp210 -3 |
|
Assassi et al. [5] |
225 |
37 |
sp100 -13 gp210 -3 |
|
Imura-Kumada et al. [14] |
86 |
11 |
|
|
Cavazzana et al. [15] |
201 |
36 |
sp100 -5 gp210 -1 |
|
Norman et al. [16] |
52 |
7 |
sp100-1 |
|
Skare et al. [17] |
63 |
6 |
|
Eighteen out of 156 patients had significant fibrosis, accounting for 12.5%. However, the distribution amongst the 2 studies was different as in Table 4. In study 1, the prevalence was 16.5%, and most associations were with autoimmune disease. On the other hand, Cuomo et al. had a low prevalence of 3.4%. A commonly associated risk factor was triglyceride levels. Figure 5 shows the forest plot indicating an insignificant relationship with the SSc despite it being a primarily fibrosing condition.
|
Author |
Number of patients with SSc |
Fibrosis |
Comments
|
|
Lorena et al. [8] |
97 |
16 patients |
AMA positivity and ALP were independently associated with liver fibrosis |
|
Cuomo et al. [10] |
59 |
2 |
TAG levels were associated |
Discussion
Systemic sclerosis (SSc) is a clinically and serologically heterogeneous disease rather than a single entity. The classic division is into limited cutaneous SSc (lcSSc) and Diffuse cutaneous SSc (dcSSc) based on the extent of skin fibrosis. Pulmonary fibrosis, renal crisis are more frequent in dcSSc. Pulmonary arterial hypertension and overlap autoimmunity are more common in lcSSc. Primary biliary cholangitis (PBC) is most strongly associated with the limited cutaneous subtype of systemic sclerosis (lcSSc). However, it has not been explored in this study. Patients with internal organ disease and SSc?specific autoantibodies but minimal/absent skin thickening are called Sine scleroderma (ssSSc) [21].
Recent cross-phenotype and genetic-correlation studies show a nontrivial shared genetic background between SSc and PBC. Shared loci include immune-regulatory and HLA-region signals. This genetic overlap plausibly explains why PBC is the most reported autoimmune liver disease co-occurring with SSc. AIH appears in some series as part of overlap syndromes (AIH–PBC overlap rather than isolated AIH). Overlapping features such as shared regulatory T cell abnormalities and common genetic variants (e.g., STAT4, IRF5, NF-κB, IRF8) justify a potential pathogenetic link. The prevalence of disease-specific autoantibodies is considerably higher, indicating a broader subclinical spectrum of hepatic involvement [21]. Hence investigation into associated autoimmune liver disease and antibody profile was also carried out.
This review of 11 retrospective observational studies highlights liver involvement in patients with systemic sclerosis (SSc), a primarily fibrosing autoimmune disease. Out of 2,797 patients with SSc across these studies, 190 were found to have liver disease, with 157 cases attributed to autoimmune etiologies, establishing a 6.7% prevalence of autoimmune liver diseases in this population.
Primary biliary cholangitis (PBC) emerged as the most common autoimmune liver disease associated with SSc, with a prevalence of approximately 5%. This is markedly higher than the general population prevalence of PBC, which ranges from 0.02% to 0.04% depending on the geographic region, underscoring a significant association between PBC and SSc. The association is further strengthened by the notable presence of antimitochondrial antibodies (AMA), detected in 10.87% of patients, which is considerably higher than in the general population and indicates subclinical or evolving PBC in many SSc patients.
Autoimmune hepatitis (AIH) was identified in 1.2% of SSc patients, a figure derived from studies 1 and 2 where a definitive diagnosis was made. This prevalence also exceeds general population estimates for AIH (approximately 0.02%-0.05%), further indicating that SSc patients may be predisposed to broader autoimmune liver involvement.
Serological profiles from studies focusing on PBC revealed the presence of disease-specific autoantibodies in a substantial proportion of SSc patients. Apart from AMA, anti-sp100 and anti-gp210 antibodies were frequently observed. Anti-sp100, found in 3.1%, and anti-gp210, although less frequent, serve as useful markers for PBC diagnosis and prognosis.
Two studies specifically addressed liver fibrosis using elastography. Notably, 16.5% of patients in the first study exhibited liver fibrosis, which was independently associated with AMA positivity and elevated alkaline phosphatase (ALP). In contrast, the rest of the studies found fibrosis in only 3.4%, with elevated triglyceride levels being a more prominent association than autoimmunity. The different incidence of actual fibrosis, possibly confounded by metabolic factors including triglyceride levels, needs further matching. Cholestatic fibrogenesis follows different cell-cell signaling and may be slower in many patients, especially if recognized and treated. SSc is primarily a vasculopathic disease. There’s no clear reason why SSc would accelerate hepatocellular fibrogenesis.
Although SSc is recognized as a fibrosing condition, the data do not strongly support a consistent or predominant hepatic fibrosing phenotype across all cohorts. Figure 5 underscores this variability, showing no significant pooled association between SSc and liver fibrosis, despite localized trends in select populations such as Italy.
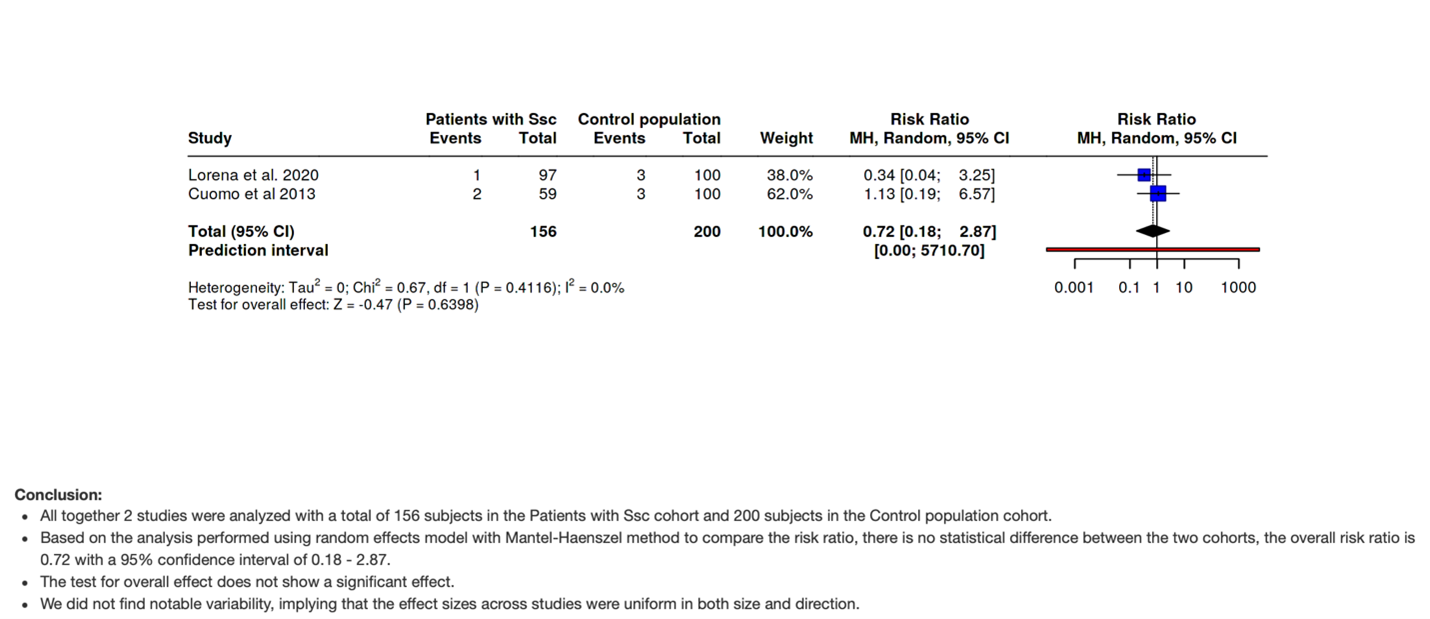
Figure 5. Forest plot indicating the relationship of liver fibrosis with the SSc in 2 Italian studies.
Geographic variability was notable, with a higher prevalence of autoimmune liver diseases observed in Italian and Japanese cohorts. This could reflect regional differences in diagnostic practices, genetic predisposition, or environmental triggers.
Conclusion
Hepatic involvement in SSc is under-investigated. Autoimmune conditions, including PBC and AIH, had a significant association as mentioned in the literature. The statistically significant elevation of anti-mitochondrial antibodies also consolidates it. As per fibrosis, despite the fibrosing nature of the disease, a significant association was not seen, and it was mostly associated with pre-existing conditions.
References
2. Emmanuel A. Current management of the gastrointestinal complications of systemic sclerosis. Nat Rev Gastroenterol Hepatol. 2016 Aug;13(8):461–72.
3. Lindor KD, Bowlus CL, Boyer J, Levy C, Mayo M. Primary Biliary Cholangitis: 2018 Practice Guidance from the American Association for the Study of Liver Diseases. Hepatology. 2019 Jan;69(1):394–419.
4. McFarlane IM, Bhamra MS, Kreps A, Iqbal S, Al-Ani F, Saladini-Aponte C, et al. Gastrointestinal Manifestations of Systemic Sclerosis. Rheumatology (Sunnyvale). 2018;8(1):235.
5. Assassi S, Fritzler MJ, Arnett FC, Norman GL, Shah KR, Gourh P, et al. Primary biliary cirrhosis (PBC), PBC autoantibodies, and hepatic parameter abnormalities in a large population of systemic sclerosis patients. J Rheumatol. 2009 Oct;36(10):2250–6.
6. Alastal Y, Hammad TA, Renno A, Khalil B, Pierre J, Kwaah B, et al. Gastrointestinal manifestations associated with systemic sclerosis: results from the nationwide inpatient sample. Ann Gastroenterol. 2017;30(5):498–503.
7. Chatterjee S, Dombi GW, Severson RK, Mayes MD. Risk of malignancy in scleroderma: a population-based cohort study. Arthritis Rheum. 2005 Aug;52(8):2415–24.
8. Lorena M, Bellan M, Lepore M, Sola D, Pedrazzoli R, Rigamonti C, et al. Clinical Relevance of Liver Involvement in the Clinical Course of Systemic Sclerosis. J Clin Med. 2022 Feb 12;11(4):966.
9. Marí-Alfonso B, Simeón-Aznar CP, Guillén-Del Castillo A, Rubio-Rivas M, Trapiella-Martínez L, Todolí-Parra JA, et al. Hepatobiliary involvement in systemic sclerosis and the cutaneous subsets: Characteristics and survival of patients from the Spanish RESCLE Registry. Semin Arthritis Rheum. 2018 Jun;47(6):849–57.
10. Cuomo G, Iandoli C, Galiero R, Caturano A, Di Vico C, Perretta D, et al. Liver Involvement in Patients with Systemic Sclerosis: Role of Transient Elastography in the Assessment of Hepatic Fibrosis and Steatosis. Diagnostics (Basel). 2023 May 17;13(10):1766.
11. Sawadpanich K, Promasen P, Mairiang P, Sukeepaisarnjareon W, Sangchan A, Suttichaimongkol T, et al. Incidence and Predictors of an Abnormal Liver Function Test Among 674 Systemic Sclerosis Patients: A Cohort Study. Open Access Rheumatol. 2023 May 16;15:81–92.
12. Salem GI, Abdulrahman AA. Evaluation of liver function tests in scleroderma patients. Rheumatol Int. 2012 Aug;32(8):2371–5.
13. Wielosz E, Majdan M, Koszarny A, Dryglewska M, Tabarkiewicz J. Presence of organ‑specific antibodies in patients with systemic sclerosis. Pol Arch Med Wewn. 2016 Oct 5;126(11):862–9.
14. Imura-Kumada S, Hasegawa M, Matsushita T, Hamaguchi Y, Encabo S, Shums Z, et al. High prevalence of primary biliary cirrhosis and disease-associated autoantibodies in Japanese patients with systemic sclerosis. Mod Rheumatol. 2012 Nov;22(6):892–8.
15. Cavazzana I, Ceribelli A, Taraborelli M, Fredi M, Norman G, Tincani A, et al. Primary biliary cirrhosis-related autoantibodies in a large cohort of italian patients with systemic sclerosis. J Rheumatol. 2011 Oct;38(10):2180–5.
16. Norman GL, Bialek A, Encabo S, Butkiewicz B, Wiechowska-Kozlowska A, Brzosko M, et al. Is prevalence of PBC underestimated in patients with systemic sclerosis? Dig Liver Dis. 2009 Oct;41(10):762–4.
17. Skare TL, Nisihara RM, Haider O, Azevedo PM, Utiyama SR. Liver autoantibodies in patients with scleroderma. Clin Rheumatol. 2011 Jan;30(1):129–32.
18. Muratori P, Granito A, Quarneti C, Ferri S, Menichella R, Cassani F, et al. Autoimmune hepatitis in Italy: the Bologna experience. J Hepatol. 2009 Jun;50(6):1210–8.
19. Hahn JW, Yang HR, Moon JS, Chang JY, Lee K, Kim GA, et al. Global incidence and prevalence of autoimmune hepatitis, 1970-2022: a systematic review and meta-analysis. EClinicalMedicine. 2023 Oct 17;65:102280.
20. Gazda J, Drazilova S, Janicko M, Jarcuska P. The Epidemiology of Primary Biliary Cholangitis in European Countries: A Systematic Review and Meta-Analysis. Can J Gastroenterol Hepatol. 2021 Jun 19;2021:9151525.
21. Lepri G, Bellando Randone S, Matucci Cerinic M, Allanore Y. Systemic sclerosis and primary biliary cholangitis: An overlapping entity? J Scleroderma Relat Disord. 2019 Jun;4(2):111–7.