Abstract
Targeting EGFR has a long history in the treatment of non-small cell lung cancer (NSCLC). It was around the 2000s that it was reported that EGFR protein expression increased with bronchial dysplasia in high-risk smokers and patients with lung cancer. However, EGFR inhibitors were not effective in unselected patients with advanced NSCLC. After the identification of sensitizing EGFR mutations, tyrosine kinase inhibitors became the cornerstone of treatment for patients with EGFR-mutated NSCLC. However, other drugs were developed to target EGFR in the EGFR-wild type population, such as monoclonal antibodies. Cetuximab is an anti-EGFR monoclonal antibody, and has been a focus over the past two decades. Though not approved in NSCLC due to marginal and inconsistent effects in phase 3 trials, research aimed to discover biomarkers to identify a subgroup of the population that might benefit. This includes a composite score that evaluates histology, immunohistochemistry, and gene copy amplification. This article reviews the history of the development and discontinuation of monoclonal antibodies in NSCLC and discusses the role of biomarkers in the treatment of advanced EGFR-wild type NSCLC.
Keywords
Non-small cell lung cancer, Squamous carcinoma, EGFR, Monoclonal antibody, Cetuximab
Abbreviations
ADC: Antibody-Drug Conjugate; EGFR: Epidermal Growth Factor; FISH: Fluorescence In Situ Hybridization; IHC: Immunohistochemitry; mAb: Monoclonal Antibody; NGS: Next-Generation Sequencing; NS: Non Statistically Significant; NSCLC: Non-Small Cell Lung Cancer; NR: Not Reported; ORR: Overall Response Rate; OS: Overall Survival; PFS: Progression-free Survival; TKI: Tyrosine Kinase Inhibitor
Background
Non-small cell lung cancer (NSCLC) is the leading cause of cancer-related deaths [1]. However, significant improvements in the past decades have been achieved with improved outcomes [2-4]. Several mutations have been described as promoters of oncogenesis, and specific treatments are available, including those for Epidermal Growth Factor (EGFR) mutations [4]. Testing for mutations is recommended for every patient with advanced NSCLC, with the exception of patients with squamous NSCLC with a history of tobacco consumption [2,4]. The EGFR gene, also known as ERBB1 or HER1 (Human Epidermal growth factor Receptor 1) encodes the EGFR protein, a trans-membrane growth factor receptor [5]. Binding of EGFR triggers the activation of its intracellular tyrosine kinase, leading to signaling cascades of several oncogenic pathways (e.g. PI3K/AKT, MAPK, Ras/Raf/Mek/Erk, PLC-y/PKCJAK/STAT) [5,6]. EGFR protein overexpression has been found in premalignant cells, underlining its role in carcinogenesis [7,8].
Methods for EGFR Evaluation
EGFR status can be described using immunohistochemistry (IHC) to examine surface protein expression, fluorescence in situ hybridization (FISH) to assess gene copy number, or DNA sequencing to detect mutations as well as copy number variations (Figure 1).
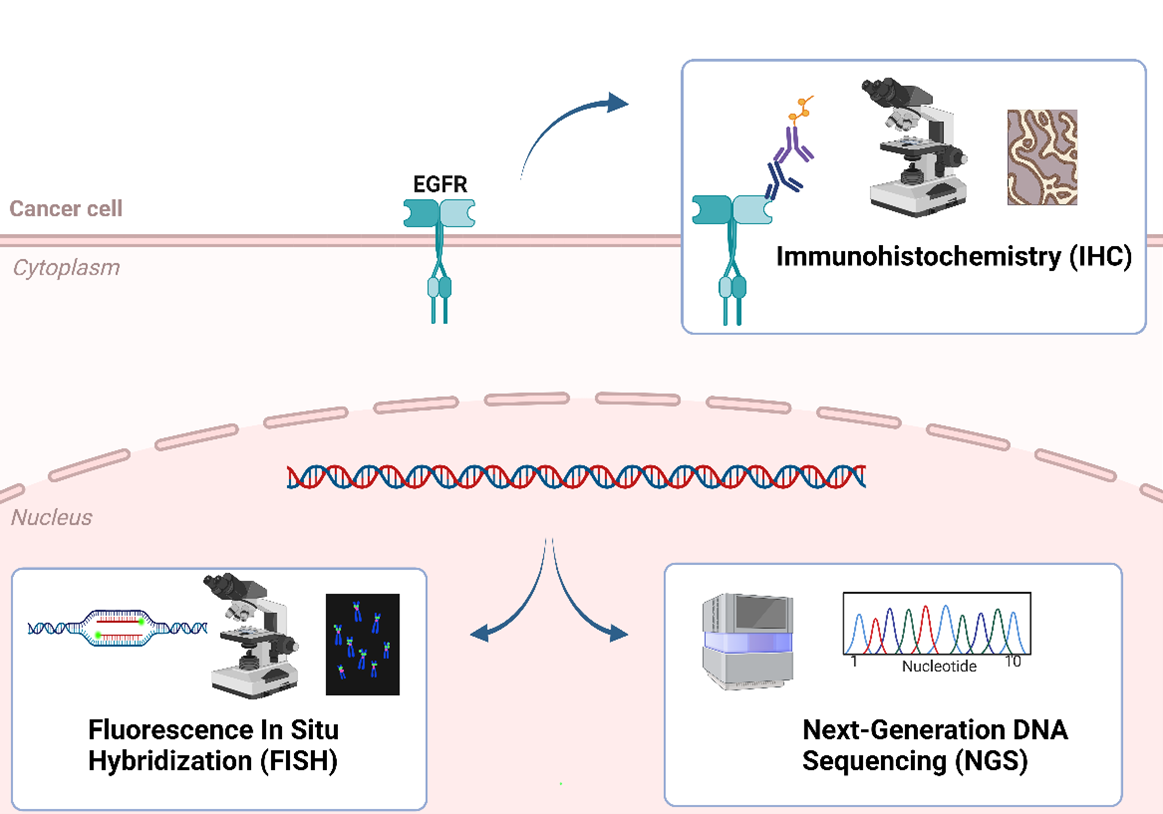
Figure 1. Techniques for EGFR evaluation.
EGFR protein expression studied with IHC is found in a majority of NSCLC, ranging from 50% to 90% of NSCLC, depending on the antibody and scoring technique used [9-11]. EGFR expression is reported to be higher in squamous NSCLC than in non-squamous histologies [11,12]. EGFR overexpression was not correlated with survival in a meta-analysis of 2185 patients with NSCLC [13]. However, due to variable staining methods and scoring systems, drawing definitive conclusions can be challenging [11].
Dysregulation of EGFR can also be detected using FISH, a technique that can determine whether the gene and the chromosome are amplified. The amplification can be either balanced (with the same number of gene copies as chromosomes) or unbalanced (with more gene copies than chromosomes); the latter condition is referred to as gene amplification or high gene copy number [14,15]. The Colorado Criteria were published to ensure homogeneous testing [15]. They define FISH positivity as EGFR FISH-positive in specimens that have (1) at least 40% of cells with at least 4 EGFR copies or (2) evidence of EGFR gene amplification, defined according to one of the following criteria: (a) an EGFR/CEP7 ratio of at least 2, (b) the presence of gene clusters in at least 10% of tumor cells, and (c) at least 15 copies of EGFR in at least 10% of tumor cells [15]. In phase 2-3 trials of cetuximab and necitumumab, monoclonal antibodies targeting EGFR, gene amplification according to these criteria was found in 20-60% of advanced NSCLC (Table 1) [16-20].
|
Trial, Phase |
Trial setting |
Trial population |
IHC + |
IHC H-score ≥200 |
Oucome IHC high with EGFR mAb |
FISH + (Colorado criteria) |
Outcome FISH+ with EGFR mAb |
|
FLEX, Phase 3 |
First line chemotherapy (cisplatin/vinorelbine) +/- cetuximab |
1125 patients with advanced NSCLC, 33% squamous |
100% (85% of screened patients) |
31% |
Improved OS |
37% |
No significant difference |
|
BMS 099, Phase 3 |
First- line chemotherapy (taxane/carboplatin) +/- cetuximab. |
676 patients with advanced NSCLC, 19% squamous |
89% |
NR |
Trend to improved ORR (NS) |
52% |
No significant difference |
|
BMS 100, Phase 2 |
First-line chemotherapy (gemcitabine/platinum) + cetuximab |
131 patients with advanced NSCLC, 33% squamous |
NR |
NR |
NR |
NR |
NR |
|
LUCAS, Phase 2 |
First-line chemotherapy (cisplatin/vinorelbine) +/- cetuximab |
86 patients with advanced NSCLC expressing EGFR, 42% squamous |
67% |
NR |
NR |
NR |
NR |
|
SWOG S0342, Phase 2 |
First-line chemotherapy (gemcitabine/ cisplatin or carboplatin) + cetuximab (concurrent or sequential) |
224 patients with advanced NSCLC, 17% squamous |
NR |
NR |
NR |
59% |
Improved PFS and OS |
|
SWOG S0536, Phase 2 |
First-line chemotherapy (carboplatin/paclitaxel) + cetuximab and bevacizumab +/- maintenance with cetuximab and bevacizumab |
102 patients with advanced non-squamous NSCLC |
73% |
36% |
Trend for better ORR, PFS, and OS (NS) |
26% |
No significant difference |
|
SWOG 0819, Phase 3 |
First-line chemotherapy (carboplatin/paclitaxel) +/- bevavacizumab +/- cetuximab |
1313 patients with advanced NSCLC, 24% squamous |
NR |
31% |
Trend for improved OS (NS) Improved OS in squamous NSCLC and when combined to FISH+ |
41% |
Trend for improved OS (NS) Improved OS in squamous NSCLC and when combined to IHC H-score ≥200 |
|
SQUIRE, Phase 3 |
First-line chemotherapy (cisplatin–gemcitabine) +/-necitumumab |
1093 patients with advanced squamous NSCLC |
95% |
38% |
Trend to improved OS (NS) |
37% |
Trend for improved OS (NS) |
|
INSPIRE, Phase 3 |
First-line chemotherapy (pemetrexed/cisplatin) +/- necitumumab |
633 patients with advanced non-squamous NSCLC |
77% |
41% |
No significant differences |
NR |
NR |
|
mAb: Monoclonal Antibody; NR: Not Reported; NS: Non Statistically Significant; OS: Overall Survival; PFS: Progression-Free Survival; ORR: Overall Response Rate |
|||||||
DNA sequencing techniques, notably next-generation sequencing (NGS), is considered the gold standard for detecting and classifying EGFR mutations in patients with NSCLC [4]. The identification of specific EGFR mutations has proven to be the best predictor of the response to EGFR tyrosine kinase inhibitor (TKI) therapy [4]. NGS has progressively replaced IHC and FISH in the assessment of oncogenic drivers in advanced NSCLC, thanks to its broad coverage, accuracy, and efficiency [3,4]. Furthermore, gene amplification can also be assessed with NGS [21,22].
Targeting EGFR in Mutated and Wild-type EGFR NSCLC: TKI and Monoclonal Antibodies
EGFR TKIs were initially developed and tested in all-comers with NSCLC. However, in 2004, two studies showed that responses to gefitinib, an EGFR TKI, were correlated with mutations in the kinase domain of EGFR. A phase 3 trial of gefitinib versus chemotherapy in patients with advanced NSCLC also reported a doubling of progression-free survival (PFS) in patients with EGFR mutations [23]. A phase 3 trial later confirmed these results in 2010, demonstrating improved PFS with gefitinib over chemotherapy for patients with EGFR-mutated advanced NSCLC [24].
Since these results, the treatment of patients with EGFR-mutated NSCLC now primarily relies on the third-generation EGFR TKI osimertinib [2,4]. For patients with wild-type EGFR NSCLC, after it became clear that they did not benefit from EGFR TKIs, the question remained whether they could benefit from other drugs targeting EGFR, such as monoclonal antibodies, bispecific antibodies or antibody drug conjugates (ADCs). This is indeed the case in other cancers [25-27].
Cetuximab is a chimeric IgG1 monoclonal antibody that binds to EGFR and inhibits its tumor signaling activation [28]. The interaction between cetuximab and the receptor causes the internalization of the antibody-receptor complex, resulting in a reduction in overall EGFR expression, ultimately inhibiting growth and survival signal [28]. Cetuximab is approved for the treatment of colon cancer, head and neck carcinoma, and non-melanoma skin cancer [25-27].
The association of cetuximab combined with chemotherapy in patients with advanced NSCLC was studied in several phase 2 and phase 3 trials [29-33]. Since these studies were conducted before EGFR mutations were identified as predictive factors for TKI treatment, patients were included regardless of their EGFR mutational status. Two meta-analyses of trials that added cetuximab to chemotherapy in the first-line treatment of patients with advanced NSCLC demonstrated a favorable benefit-to-risk ratio, with significantly improved overall survival [34,35]. However, due to limited benefits, cetuximab was not approved by regulatory authorities [36,37]. In the second-line setting, the combination of cetuximab and pemetrexed failed to improve outcomes compared to pemetrexed alone in advanced NSCLC [38].
Necitumumab is another monoclonal antibody that competitively inhibits EGFR [39]. The phase 3 INSPIRE trial evaluated the addition of necitumumab to chemotherapy in patients with advanced non-squamous NSCLC and did not find a survival improvement [40]. However, the SQUIRE trial, conducted in patients with advanced squamous NSCLC, demonstrated an improved overall survival (HR 0.84 [95% CI 0.74–0.96]; p=0.01), which led to necitumumab’s approval in this setting [12].
Other anti-EGFR monoclonal antibodies, such as panitumumab and matuxumab, failed to demonstrate significant improvements in outcomes for patients with advanced NSCLC [41,42]. Nimotuzumab, on the other hand, was found to be non-inferior to docetaxel in the second line but was not approved. Nimotuzumab was also studied with chemoradiotherapy for patients with locally advanced NSCLC in a phase 2 trial, with acceptable safety and better outcomes in patients with squamous NSCLC [43]. However, its phase 3 trial in patients with advanced squamous NSCLC was discontinued early due to safety concerns [44].
In 2021, amivantamab, a bispecific monoclonal antibody targeting EGFR and MET, was approved by the FDA for the treatment of advanced NSCLC with EGFR exon 20 insertion mutations in the second line [45]. It is expected to move to the first-line setting following the results of the PAPILLON trial, demonstrating improved PFS when combined to chemotherapy, compared to chemotherapy alone [46]. The combination of amivantamab and lazertinib compared to osimertinib also recently demonstrated PFS improvement in patients with advanced NSCLC and classical EGFR mutations (exon 19 deletion and L858R mutation) [47].
Role of Biomarker
While trials that included patients without biomarker selection did not show consistent improvements with anti-EGFR monoclonal antibodies, research aimed at identifying patients who could benefit from these treatments, exploring various criteria. These criteria primarily included EGFR expression using IHC, EGFR gene amplification through FISH, EGFR or KRAS mutations, and histology [37,48].
IHC expression was used as selection criterion in a phase 2 trial with cetuximab, demonstrating a good safety profile [33], and the phase 3 FLEX trial was conducted to validate these results. The FLEX trial enrolled chemotherapy-naive patients with advanced EGFR-expressing NSCLC and randomized them to chemotherapy plus cetuximab or chemotherapy alone. The trial demonstrated a survival improvement, with a median overall survival (OS) of 11.3 months with the addition of cetuximab versus 10.1 months; HR for OS 0.871 (95% CI 0.762–0.996; p=0.044) [30]. Retrospective analyses in patients with high EGFR expression, defined as an H-score ≥200, showed improved OS in the chemotherapy plus cetuximab group compared to the chemotherapy alone group, with a median OS of 12.0 months versus 9.6 months; HR 0.73 (95% CI 0.58–0.93; p=0.011) [49]. However, even though there was a trend in favor of cetuximab combination in other trials of cetuximab and chemotherapy, such as the BMS099 and SWOG S0536 trials [20,50], H-score ≥200 was not a consistent biomarker among other trials (Table 1) [16].
EGFR copy number via FISH was also studied. A retrospective analysis of the phase 2 SWOG S0342 trial, which evaluated concurrent or sequential cetuximab plus chemotherapy in advanced NSCLC, reported that patients with a high EGFR copy number had a better outcome with cetuximab treatment [18].
This finding led to the design of the phase 3 trial SWOG S0819, aiming to validate FISH amplification as a biomarker. While the FISH-positive subgroup did indeed show a better survival with cetuximab (HR for OS 0.81 [95% CI 0.66–1.0], p= 0.048), the primary endpoint of improved PFS was not statistically significant (HR 0.92, [05% CI 0.75–1.12], p = 0.40) [16]. A subgroup analysis of patients with squamous histology and high EGFR copy number by FISH demonstrated an even more improved survival (HR for OS 0.58 [95% CI 0.36–0.86]; p=0.0071) [51]. Nevertheless, FISH amplification was not predictive in retrospective analyses in other phase 3 trials [17,19]. Thus, this finding raises the question whether the predictive biomarker in the EGFR wild-type patient population might be histology dependent. Indeed, patients with squamous NSCLC also tended to benefit from cetuximab in the FLEX trial [30]. As mentioned earlier, it was also among the squamous NSCLC that necitumumab was more effective [12].
Regarding genomic analyses, EGFR mutational status was not predictive for cetuximab, as observed in several studies [17,19,20]. This was also the case for KRAS mutations, unlike what is observed in colon cancer [17,19,25,52,53].
As we see, results conflicted between IHC and FISH. A new retrospective analysis of the SWOG S0819 was published in 2022, exploring the role of combining IHC and FISH scores in patients with squamous NSCLC. This analysis identified a subgroup of patients, i.e., those with high gene copy number and high EGFR protein expression, who had a significant survival improvement with cetuximab, with a median OS of 12.6 versus 4.6 months (HR for OS 0.32 [95% CI 0.18-0.59], p=0.0002) [52].
Have We Found the Perfect Predictive Algorithm?
These results are encouraging and may have identified the subgroup of patients who benefit from cetuximab. The limitation of combining FISH, IHC, and histology relies on the retrospective nature of its analysis. Validation in other trials and prospective assessments would be required to implement it in clinical practice.
Due to its limited results and the revolution brought by immunotherapy, the development of cetuximab in NSCLC was discouraged [37]. The patent for cetuximab expired in Europe in 2014 and in the USA in 2016, and cetuximab and panitumumab are now developed by the same company [54]. Therefore, it is unlikely to see new large trials of cetuximab in advanced NSCLC [37]. Moreover, since panitumumab is approved for the treatment of squamous NSCLC, it's unlikely that cetuximab will have a future in NSCLC. Despite the consistent signal of effectiveness seen in all the trials involving cetuximab, it's disappointing to realize that the conclusions of biomarker research may have come too late [37].
Future Perspectives: Combination with Immunotherapy and Antibody-Drugs Conjugates
In the era of immunotherapy, a phase 2 trial combining avelumab and cetuximab with chemotherapy in patients with advanced squamous NSCLC demonstrated an acceptable safety profile, but overall response rate (ORR) was not improved [55]. A numerically higher ORR was observed in patients with EGFR FISH–positive tumors [55].
Necitumumab was also evaluated in combination with pembrolizumab in a phase 1b trial in advanced NSCLC, with acceptable safety and a modest benefit (ORR of 23%) [56]. There is an ongoing trial (NCT04285671) evaluating the combination of trastuzumab and necitumumab in patients with EGFR-mutated and TKI-resistant NSCLC. Currently, there is no ongoing trial involving necitumumab or cetuximab in the United States for patients with EGFR wild-type NSCLC, except for one trial with cetuximab in combination with PF-07284892, a SHP2 inhibitor (NCT04800822) [57].
Amivantamab, a bispecific antibody targeting EGFR and MET, was recently found to provide PFS benefit over osimertinib in the first-line setting for patients with sensitizing EGFR-mutated tumors [47]. It was also superior to chemotherapy in patients progressing after EGFR-TKI [58], and in patients with EGFR exon 20 mutations [46]. Whether this antibody might also benefit patients with wild-type EGFR NSCLC remains to be investigated. A study on xenograft models suggested activity of amivantamab in models with high EGFR expression (H-score ≥170) [59].
Antibody-drug conjugates (ADCs) are new treatments for NSCLC. They are engineered to connect a monoclonal antibody to a payload, typically a cytotoxic agent [60]. Several targets have been identified, with some of them being evaluated in all-comers patients, while others are "biomarker-dependent," requiring a previous analysis of the tumor, such as ADCs targeting HER2, c-MET, CEACAM5 and PK7 (Table 2) [61]. Trastuxumab deruxtecan, an ADC targeting HER2, has received FDA’s accelerated approval for the treatment of patients with HER2-mutated NSCLC [61]. In all-comers patients with advanced NSCLC, a phase 3 trial of datopotamab deruxtecan (Dato-DXd), an ADC targeting TROP2, recently demonstrated that Dato-DXd improved PFS compared to docetaxel [62]. However, patients with squamous histology did not seem to benefit from Dato-DXd, highlighting once again the role of histology [62]. Several trials are ongoing, and will probably redefine the treatment arsenal for NSCLC [60].
|
Target |
ADC |
Payload |
Population (biomarker) studied |
|
HER2 |
Ado-trastuzumab emtansine |
Emtansine (DM1) |
HER2 mutation |
|
Trastuzumab-deruxtecan (T-DXd) |
Deruxtacan (DXd) |
HER2 mutation or overexpression |
|
|
A166 |
Duostatin-5 |
HER2 + (IHC) or HER amplification (ISH or NGS) |
|
|
XMT-1522 |
Auristatin F-hydroxypropylamide |
HER2 + (IHC) |
|
|
HER3 |
Patritumab-deruxtecan |
Deruxtacan (DXd) |
EGFR mutation and no biomarker |
|
TROP2 |
Datopotamab-deruxtecan (Dato-DXd) |
Deruxtacan (DXd) |
No biomarker |
|
Sacituzumab-govitecan |
SN38 |
No biomarker |
|
|
Sacituzumab tirumotecan (SKB264) |
KL610023 |
No biomarker |
|
|
CEACAM5 |
Tusamitamab ravtansine |
DM4 |
CEACAM5 + of high level of circulating CEA |
|
c-MET |
Telisotuzumab vedotin |
MMAE |
c-MET1+ (IHC) of MET amplification (FISH) |
|
B7-H3 |
Vobramitamab duocarmazine (MGC018) |
DUBA |
No biomarker |
|
Ifinatamab Deruxtecan (DS-7300) |
Deruxtacan (DXd) |
No biomarker |
|
|
AXL |
Enapotamab vedotin |
MMAE |
No biomarker |
|
Mecbotamab vedotin (BA3011) |
MMAE |
No biomarker |
|
|
PK7 |
Cofetuzumab pelidotin |
Auristatin-0101 |
PK7+ (IHC) |
|
PVRL4 |
Enfortumab vedotin |
MMAE |
No biomarker |
|
TF |
Tisotumab-vedotin |
MMAE |
No biomarker |
|
ROR2 |
Ozuriftamab vedotin (BA3021) |
MMAE |
No biomarker |
|
GPNMB |
Glembatumumab Vedotin |
MMAE |
Squamous NSCLC |
|
NaPi2b |
Upifitamab rilsodotin |
AF-HPA |
No biomarker |
|
Lifastuzumab vedotin |
MMAE |
No biomarker |
ADCs targeting EGFR are being evaluated. Serclutamab talirine and depatuxizumab mafodotin were studied in glioblastoma, but did not demonstrate benefit [63,64]. MRG003 is another ADC targeting EGFR with a monomethyl auristatin E (MMAE) payload and is currently being studied in a phase 3 trial in patients with head and neck cancer (NCT05751512). In small-cell lung cancer, a phase 2 trial is underway in patients with EGFR positive tumors (NCT04838548). A phase 1 trial of M1231, a bispecific ADC targeting EGFR and Mucin 1 was recently completed, and results should be published soon (NCT04695847).
The use of biomarkers to select patient population varies depending on the drug. The benefit of trastuzumab deruxtecan was clearly observed in patients with HER2-mutated NSCLC but was not correlated with HER2 IHC expression [65]. However, other ADCs targeting HER2 are studied in IHC-positive tumors [61]. Tusamitamab ravtansine, an ADC targeting CEACAM5, focuses on a population of patient with positive CEACAM5 expression, or elevated CEA levels [61]. Telisotuzumab vedotin, an anti-c-MET ADC is studied in patients with c-MET positive NSCLC or with MET amplification, while cofetuzumab pelidotin is studied in patients with PK7 positive tumors [61]. This reflects the importance of IHC and gene amplification testing in the current landscape of clinical trials.
Conclusion
The role and mechanisms of EGFR overexpression and gene amplification in wild-type EGFR tumors are still unclear and deserve further research. Although NGS is now recommended for the identification of targetable mutations in advanced NSCLC, it is currently not recommended routinely for patients with squamous NSCLC and a history of tobacco consumption [2,3]. Neither IHC nor FISH EGFR status is currently explored in clinical practice in patients with squamous NSCLC. Although the story of cetuximab in NSCLC might have ended, we believe that it is always worthwhile to explore new biomarkers to maximize benefits and minimize side effects. This is how we approach personalized medicine, aiming to provide the right treatment to the right patient. In the era of ADCs, we believe that assessing protein expression, gene amplification and mutations will help us identify the right candidates. We also see how it is crucial to make efforts to harmonize techniques, such as with the Colorado Criteria, to ensure homogeneity in clinical research.
Future research is needed concerning biomarkers in NSCLC to enhance treatment and outcomes. Liquid biopsies are becoming widely implemented and might address the challenge of tissue limitation for comprehensive profiling, as well as playing a role in early detection and monitoring treatment response [66]. Currently, several axes are being investigated, including molecular, structural, and immune biomarkers. Innovative approaches, such as analyses integrating multi-omic profiling, might play an important role [67].
Acknowledgment
The figure was created with Biorender.
Author Contributions Statement
MLM and FH wrote, edited and approved the manuscript.
Conflicts of Interest
MLM declares no conflict of interest.
FRH: Scientific boards: AstraZeneca, Regeneron, Sanofi, Abbvie, G1 Therapeutics, Novartis, Merus Therapeutics, Merck, Novocure, NextCure, OncoHost. Patents: “EGFR protein expression and- copy number as predictive biomarkers for EGFR-directed therapies” (through University of Colorado)]. Sponsored research (through Icahn School of Medicine, Mount Sinai: Novartis. Through “Stand-Up-To Cancer”: Jazz Pharmaceuticals.
References
2. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) Non-Small Cell Lung Cancer [Internet]. 2022. Available from: https://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf
3. Hendriks LE, Kerr KM, Menis J, Mok TS, Nestle U, Passaro A, et al. Non-oncogene addicted metastatic non-small-cell lung cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up†. Annals of Oncology. 2023 Jan;S0923753422047858.
4. Hendriks LE, Kerr K, Menis J, Mok TS, Nestle U, Passaro A, et al. Oncogene-addicted metastatic non-small-cell lung cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Annals of Oncology. 2023 Jan;S0923753422047810.
5. Levantini E, Maroni G, Del Re M, Tenen DG. EGFR signaling pathway as therapeutic target in human cancers. Seminars in Cancer Biology. 2022 Oct;85:253-75.
6. Earp HS, Dawson TL, Li X, Yu H. Heterodimerization and functional interaction between EGF receptor family members: a new signaling paradigm with implications for breast cancer research. Breast Cancer Res Tr. 1995;35(1):115-32.
7. Kurie JM, Shin HJ, Lee JS, Morice RC, Ro JY, Lippman SM, et al. Increased epidermal growth factor receptor expression in metaplastic bronchial epithelium. Clin Cancer Res. 1996 Oct;2(10):1787-93.
8. Lonardo F, Dragnev KH, Freemantle SJ, Ma Y, Memoli N, Sekula D, et al. Evidence for the epidermal growth factor receptor as a target for lung cancer prevention. Clin Cancer Res. 2002 Jan;8(1):54-60.
9. Mukohara T. Expression of epidermal growth factor receptor (EGFR) and downstream-activated peptides in surgically excised non-small-cell lung cancer (NSCLC). Lung Cancer. 2003 Aug;41(2):123-30.
10. Gaber R, Watermann I, Kugler C, Reinmuth N, Huber RM, Schnabel PA, et al. Correlation of EGFR expression, gene copy number and clinicopathological status in NSCLC. Diagn Pathol. 2014 Dec;9(1):165.
11. Hirsch FR, Varella-Garcia M, Bunn PA, Di Maria MV, Veve R, Bremnes RM, et al. Epidermal Growth Factor Receptor in Non–Small-Cell Lung Carcinomas: Correlation Between Gene Copy Number and Protein Expression and Impact on Prognosis. JCO. 2003 Oct 15;21(20):3798-807.
12. Thatcher N, Hirsch FR, Luft AV, Szczesna A, Ciuleanu TE, Dediu M, et al. Necitumumab plus gemcitabine and cisplatin versus gemcitabine and cisplatin alone as first-line therapy in patients with stage IV squamous non-small-cell lung cancer (SQUIRE): an open-label, randomised, controlled phase 3 trial. The Lancet Oncology. 2015 Jul;16(7):763-74.
13. Meert AP, Martin B, Delmotte P, Berghmans T, Lafitte JJ, Mascaux C, et al. The role of EGF-R expression on patient survival in lung cancer: a systematic review with meta-analysis. European Respiratory Journal. 2002 Oct 1;20(4):975-81.
14. Cappuzzo F, Hirsch FR, Rossi E, Bartolini S, Ceresoli GL, Bemis L, et al. Epidermal Growth Factor Receptor Gene and Protein and Gefitinib Sensitivity in Non–Small-Cell Lung Cancer. JNCI: Journal of the National Cancer Institute. 2005 May 4;97(9):643-55.
15. Varella-Garcia M, Diebold J, Eberhard DA, Geenen K, Hirschmann A, Kockx M, et al. EGFR fluorescence in situ hybridisation assay: guidelines for application to non-small-cell lung cancer. J Clin Pathol. 2009 Nov;62(11):970-7.
16. Herbst RS, Redman MW, Kim ES, Semrad TJ, Bazhenova L, Masters G, et al. Cetuximab plus carboplatin and paclitaxel with or without bevacizumab versus carboplatin and paclitaxel with or without bevacizumab in advanced NSCLC (SWOG S0819): a randomised, phase 3 study. The Lancet Oncology. 2018 Jan;19(1):101-14.
17. O’Byrne KJ, Gatzemeier U, Bondarenko I, Barrios C, Eschbach C, Martens UM, et al. Molecular biomarkers in non-small-cell lung cancer: a retrospective analysis of data from the phase 3 FLEX study. The Lancet Oncology. 2011 Aug;12(8):795-805.
18. Hirsch FR, Herbst RS, Olsen C, Chansky K, Crowley J, Kelly K, et al. Increased EGFR Gene Copy Number Detected by Fluorescent In Situ Hybridization Predicts Outcome in Non–Small-Cell Lung Cancer Patients Treated With Cetuximab and Chemotherapy. JCO. 2008 Jul 10;26(20):3351-7.
19. Khambata-Ford S, Harbison CT, Hart LL, Awad M, Xu LA, Horak CE, et al. Analysis of Potential Predictive Markers of Cetuximab Benefit in BMS099, a Phase III Study of Cetuximab and First-Line Taxane/Carboplatin in Advanced Non–Small-Cell Lung Cancer. JCO. 2010 Feb 20;28(6):918-27.
20. Kim ES, Moon J, Herbst RS, Redman MW, Dakhil SR, Velasco MR, et al. Phase II Trial of Carboplatin, Paclitaxel, Cetuximab, and Bevacizumab Followed by Cetuximab and Bevacizumab in Advanced Nonsquamous Non–Small-Cell Lung Cancer: SWOG S0536. Journal of Thoracic Oncology. 2013 Dec;8(12):1519-28.
21. Singh RR, Patel KP, Routbort MJ, Aldape K, Lu X, Manekia J, et al. Clinical massively parallel next-generation sequencing analysis of 409 cancer-related genes for mutations and copy number variations in solid tumours. Br J Cancer. 2014 Nov;111(10):2014-23.
22. Xu Y, Yan J, Zhou C, Wu L, Wang H, Zhao J, et al. Genomic characterisation of de novo EGFR copy number gain and its impact on the efficacy of first-line EGFR-tyrosine kinase inhibitors for EGFR mutated non-small cell lung cancer. European Journal of Cancer. 2023 Jul;188:81-9.
23. Mok TS, Wu YL, Thongprasert S, Yang CH, Chu DT, Saijo N, et al. Gefitinib or Carboplatin–Paclitaxel in Pulmonary Adenocarcinoma. N Engl J Med. 2009 Sep 3;361(10):947-57.
24. Maemondo M, Inoue A, Kobayashi K, Sugawara S, Oizumi S, Isobe H, et al. Gefitinib or Chemotherapy for Non–Small-Cell Lung Cancer with Mutated EGFR. N Engl J Med. 2010 Jun 24;362(25):2380-8.
25. Cervantes A, Adam R, Roselló S, Arnold D, Normanno N, Taïeb J, et al. Metastatic colorectal cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Annals of Oncology. 2023 Jan;34(1):10-32.
26. Machiels JP, René Leemans C, Golusinski W, Grau C, Licitra L, Gregoire V. Squamous cell carcinoma of the oral cavity, larynx, oropharynx and hypopharynx: EHNS–ESMO–ESTRO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Annals of Oncology. 2020 Nov;31(11):1462-75.
27. Wollina U, Tchernev G, Lotti T. Chimeric Monoclonal Antibody Cetuximab Targeting Epidermal Growth Factor-Receptor in Advanced Non-Melanoma Skin Cancer. Open Access Maced J Med Sci. 2017 Dec 31;6(1):152-5.
28. Harding J, Burtness B. Cetuximab: An epidermal growth factor receptor chimerichuman-murine monoclonal antibody. Drugs of Today. 2005;41(2):107.
29. Ettinger DS. Emerging profile of cetuximab in non-small cell lung cancer. Lung Cancer. 2010 Jun;68(3):332-7.
30. Pirker R, Pereira JR, Szczesna A, Von Pawel J, Krzakowski M, Ramlau R, et al. Cetuximab plus chemotherapy in patients with advanced non-small-cell lung cancer (FLEX): an open-label randomised phase III trial. The Lancet. 2009 May;373(9674):1525-31.
31. Lynch TJ, Patel T, Dreisbach L, McCleod M, Heim WJ, Hermann RC, et al. Cetuximab and First-Line Taxane/Carboplatin Chemotherapy in Advanced Non–Small-Cell Lung Cancer: Results of the Randomized Multicenter Phase III Trial BMS099. JCO. 2010 Feb 20;28(6):911-7.
32. Butts CA, Bodkin D, Middleman EL, Englund CW, Ellison D, Alam Y, et al. Randomized Phase II Study of Gemcitabine Plus Cisplatin or Carboplatin, With or Without Cetuximab, As First-Line Therapy for Patients With Advanced or Metastatic Non–Small-Cell Lung Cancer. JCO. 2007 Dec 20;25(36):5777-84.
33. Rosell R, Robinet G, Szczesna A, Ramlau R, Constenla M, Mennecier BC, et al. Randomized phase II study of cetuximab plus cisplatin/vinorelbine compared with cisplatin/vinorelbine alone as first-line therapy in EGFR-expressing advanced non-small-cell lung cancer. Annals of Oncology. 2008 Feb;19(2):362-9.
34. Pujol JL, Pirker R, Lynch TJ, Butts CA, Rosell R, Shepherd FA, et al. Meta-analysis of individual patient data from randomized trials of chemotherapy plus cetuximab as first-line treatment for advanced non-small cell lung cancer. Lung Cancer. 2014 Feb;83(2):211-8.
35. Yang ZY, Liu L, Mao C, Wu XY, Huang YF, Hu XF, et al. Chemotherapy with cetuximab versus chemotherapy alone for chemotherapy-naive advanced non-small cell lung cancer. The Cochrane Database of Systematic Reviews. 2014 Nov 17;2014(11):CD009948.
36. Sgambato A, Casaluce F, Maione P, Rossi A, Ciardiello F, Gridelli C. Cetuximab in advanced non-small cell lung cancer (NSCLC): the showdown? J Thorac Dis. 2014 Jun;6(6):578-80.
37. Mazzarella L, Guida A, Curigliano G. Cetuximab for treating non-small cell lung cancer. Expert Opinion on Biological Therapy. 2018 Apr 3;18(4):483-93.
38. Kim ES, Neubauer M, Cohn A, Schwartzberg L, Garbo L, Caton J, et al. Docetaxel or pemetrexed with or without cetuximab in recurrent or progressive non-small-cell lung cancer after platinum-based therapy: a phase 3, open-label, randomised trial. The Lancet Oncology. 2013 Dec;14(13):1326-36.
39. Díaz-Serrano A, Sánchez-Torre A, Paz-Ares L. Necitumumab for the treatment of advanced non-small-cell lung cancer. Future Oncology. 2019 Mar;15(7):705-16.
40. Paz-Ares L, Mezger J, Ciuleanu TE, Fischer JR, Von Pawel J, Provencio M, et al. Necitumumab plus pemetrexed and cisplatin as first-line therapy in patients with stage IV non-squamous non-small-cell lung cancer (INSPIRE): an open-label, randomised, controlled phase 3 study. The Lancet Oncology. 2015 Mar;16(3):328-37.
41. Schneider-Merck T, Lammerts Van Bueren JJ, Berger S, Rossen K, Van Berkel PHC, Derer S, et al. Human IgG2 Antibodies against Epidermal Growth Factor Receptor Effectively Trigger Antibody-Dependent Cellular Cytotoxicity but, in Contrast to IgG1, Only by Cells of Myeloid Lineage. The Journal of Immunology. 2010 Jan 1;184(1):512-20.
42. Schiller JH, Von Pawel J, Schütt P, Ansari RH, Thomas M, Saleh M, et al. Pemetrexed with or without Matuzumab as Second-Line Treatment for Patients with Stage IIIB/IV Non-small Cell Lung Cancer. Journal of Thoracic Oncology. 2010 Dec;5(12):1977-85.
43. Yamamoto N, Harada H, Okamoto I, Masuda N, Hayakawa K, Satouchi M, et al. Phase 2 Study of Nimotuzumab in Combination With Concurrent Chemoradiotherapy in Patients With Locally Advanced Non–Small-Cell Lung Cancer. Clinical Lung Cancer. 2021 Mar;22(2):134-41.
44. Daiichi Sankyo. Daiichi Sankyo Announces Discontinuation of Phase 3 Clinical Trial in Japan of Nimotuzumab (DE-766) in Lung Cancer. 2014.
45. Cho BC, Simi A, Sabari J, Vijayaraghavan S, Moores S, Spira A. Amivantamab, an Epidermal Growth Factor Receptor (EGFR) and Mesenchymal-epithelial Transition Factor (MET) Bispecific Antibody, Designed to Enable Multiple Mechanisms of Action and Broad Clinical Applications. Clinical Lung Cancer. 2023 Mar;24(2):89-97.
46. Zhou C, Tang KJ, Cho BC, Liu B, Paz-Ares L, Cheng S, et al. Amivantamab plus Chemotherapy in NSCLC with EGFR Exon 20 Insertions. N Engl J Med. 2023 Oct 21;NEJMoa2306441.
47. Cho BC. LBA14: Amivantamab plus lazertinib vs osimertinib as first-line treatment in patients with EGFR-mutated, advanced non-small cell lung cancer (NSCLC): Primary results from MARIPOSA, a phase III, global, randomized, controlled trial. ESMO Congress 2023; 2023 Oct 23; Madrid, Spain.
48. Landi L, Rossi A. Cetuximab in the treatment of advanced non-small cell lung cancer: FISHing for a miraculous catch. J Thorac Dis. 2018 Jun;10(S16):S1940-4.
49. Pirker R, Pereira JR, Von Pawel J, Krzakowski M, Ramlau R, Park K, et al. EGFR expression as a predictor of survival for first-line chemotherapy plus cetuximab in patients with advanced non-small-cell lung cancer: analysis of data from the phase 3 FLEX study. The Lancet Oncology. 2012 Jan;13(1):33-42.
50. Lynch T, Bhagavatheeswaran P, Mukhopadhyay P, Khambata-Ford S, Harbison CT. 9001 ORAL A Retrospective Subgroup Analysis of EGFR Immunohistochemistry (IHC) Expression by Histo-Score Correlated to Outcomes From the BMS099 1st Line Phase III NSCLC Trial of Cetuximab (Cet) Plus Carboplatin/Taxane. European Journal of Cancer. 2011 Sep;47:S591-2.
51. Herbst RS, Redman MW, Kim ES, Semrad TJ, Bazhenova L, Masters G, et al. Cetuximab plus carboplatin and paclitaxel with or without bevacizumab versus carboplatin and paclitaxel with or without bevacizumab in advanced NSCLC (SWOG S0819): a randomised, phase 3 study. The Lancet Oncology. 2018 Jan;19(1):101-14.
52. Hirsch FR, Redman MW, Moon J, Agustoni F, Herbst RS, Semrad TJ, et al. EGFR High Copy Number Together With High EGFR Protein Expression Predicts Improved Outcome for Cetuximab-based Therapy in Squamous Cell Lung Cancer: Analysis From SWOG S0819, a Phase III Trial of Chemotherapy With or Without Cetuximab in Advanced NSCLC. Clinical Lung Cancer. 2022 Jan;23(1):60-71.
53. Herbst RS, Kelly K, Chansky K, Mack PC, Franklin WA, Hirsch FR, et al. Phase II Selection Design Trial of Concurrent Chemotherapy and Cetuximab Versus Chemotherapy Followed by Cetuximab in Advanced-Stage Non–Small-Cell Lung Cancer: Southwest Oncology Group Study S0342. JCO. 2010 Nov 1;28(31):4747-54.
54. BMS. Lilly, Bristol-Myers Squibb Restructure Erbitux® (cetuximab) Collaboration in North America. 2015.
55. Andric Z, Gálffy G, Cobo Dols M, Szima B, Stojanovic G, Petrovic M, et al. Avelumab in Combination With Cetuximab and Chemotherapy as First-Line Treatment for Patients With Advanced Squamous NSCLC. JTO Clinical and Research Reports. 2023 Feb;4(2):100461.
56. Besse B, Garrido P, Cortot AB, Johnson M, Murakami H, Gazzah A, et al. Efficacy and safety of necitumumab and pembrolizumab combination therapy in patients with Stage IV non-small cell lung cancer. Lung Cancer. 2020 Apr;142:63-9.
57. National Cancer Institute. Find NCI-Supported Clinical Trials [Internet]. [cited 2023 Oct 20]. Available from: https://www.cancer.gov/research/participate/clinical-trials-search/
58. Passaro A. Amivantamab plus chemotherapy (with or without lazertinib) vs chemotherapy in EGFR-mutated advanced NSCLC after progression on osimertinib: MARIPOSA-2, a phase III, global, randomized, controlled trial. ESMO Congress 2023; 2023 Oct 23; Madrid, Spain.
59. Henley B, Chevalier K, Smith M, Vijayaraghaven S, Bushey B, Chu G, et al. Abstract 953: Efficacy of amivantamab, a bispecific EGFR/MET antibody, correlates with EGFR expression and signaling in NSCLC models with wild-type EGFR. Cancer Research. 2021 Jul 1;81(13_Supplement):953.
60. Rosner S, Valdivia A, Hoe HJ, Murray JC, Levy B, Felip E, et al. Antibody-Drug Conjugates for Lung Cancer: Payloads and Progress. American Society of Clinical Oncology Educational Book. 2023 May;(43):e389968.
61. Passaro A, Jänne PA, Peters S. Antibody-Drug Conjugates in Lung Cancer: Recent Advances and Implementing Strategies. JCO. 2023 Jul 20;41(21):3747-61.
62. Lisberg A. Datopotamab deruxtecan (Dato-DXd) vs docetaxel in previously treated advanced/metastatic (adv/met) non-small cell lung cancer (NSCLC): Results of the randomized phase III study TROPION-Lung01. ESMO Congress 2023; 2023 Oct 23; Madrid, Spain.
63. Carneiro BA, Papadopoulos KP, Strickler JH, Lassman AB, Waqar SN, Chae YK, et al. Phase I study of anti-epidermal growth factor receptor antibody-drug conjugate serclutamab talirine: Safety, pharmacokinetics, and antitumor activity in advanced glioblastoma. Neuro-Oncology Advances. 2023 Jan 1;5(1):vdac183.
64. Lassman AB, Pugh SL, Wang TJC, Aldape K, Gan HK, Preusser M, et al. Depatuxizumab mafodotin in EGFR-amplified newly diagnosed glioblastoma: A phase III randomized clinical trial. Neuro-Oncology. 2023 Feb 14;25(2):339-50.
65. Rolfo C, Russo A. HER2 Mutations in Non–Small Cell Lung Cancer: A Herculean Effort to Hit the Target. Cancer Discovery. 2020 May 1;10(5):643-5.
66. Casagrande GMS, Silva MDO, Reis RM, Leal LF. Liquid Biopsy for Lung Cancer: Up-to-Date and Perspectives for Screening Programs. IJMS. 2023 Jan 28;24(3):2505.
67. Chen G, Zhang J, Fu Q, Taly V, Tan F. Integrative analysis of multi-omics data for liquid biopsy. Br J Cancer. 2023 Feb 16;128(4):505-18.
68. Genova C, Socinski MA, Hozak RR, Mi G, Kurek R, Shahidi J, et al. EGFR Gene Copy Number by FISH May Predict Outcome of Necitumumab in Squamous Lung Carcinomas: Analysis from the SQUIRE Study. Journal of Thoracic Oncology. 2018 Feb;13(2):228-36.
69. Hirsch FR, Redman MW, Herbst RS, Kim ES, Semrad TJ, Bazhenova L, et al. Biomarker-enriched efficacy of cetuximab-based therapy: Squamous subset analysis from S0819, a phase III trial of chemotherapy with or without cetuximab in advanced NSCLC. JCO. 2016 May 20;34(15_suppl):9090.
70. Abuhelwa Z, Alloghbi A, Nagasaka M. A comprehensive review on antibody-drug conjugates (ADCs) in the treatment landscape of non-small cell lung cancer (NSCLC). Cancer Treatment Reviews. 2022 May;106:102393.
71. Fang W, Cheng Y, Chen Z, Wang W, Yin Y, Li Y, et al. SKB264 (TROP2-ADC) for the treatment of patients with advanced NSCLC: Efficacy and safety data from a phase 2 study. JCO. 2023 Jun 1;41(16_suppl):9114.