Abstract
Background: Enterovirus infection poses a significant and recurrent public health challenge in Taiwanese preschool and childcare settings. While numerous studies address knowledge gaps, there is a lack of synthesized evidence identifying common practice errors and the multi-level factors influencing childcare personnel's infection control behaviors from a systemic perspective.
Objective: This narrative review aims to synthesize empirical and policy literature to systematically map the principal categories of infection control errors, identify their multilevel influencing factors, and provide actionable implications for enterovirus prevention in early childhood settings.
Methods: A systematic literature search was conducted across multiple databases, including PubMed, Scopus, ERIC, and Taiwan’s National Digital Library of Theses, spanning January 2010 to December 2024. A total of 21 studies and official reports were included in the final synthesis.
Results: Three principal categories of infection control errors were identified among childcare personnel: insufficient hand hygiene and environmental cleaning, delayed symptom recognition and reporting, and inconsistent adherence to institutional procedures. These errors are shaped by interacting factors across three levels: individual (e.g., knowledge and self-efficacy), organizational (e.g., staffing and resource constraints), and sociocultural (e.g., parental cooperation and cultural norms).
Conclusion: These findings underscore that effective enterovirus control requires interventions targeting not only individual knowledge but also addressing structural and relational barriers. The review recommends standardized, sustained training, the implementation of clear and simple protocols, and policy adjustments to optimize staffing and support parental involvement.
Keywords
Enterovirus infections Infection control, Childcare personnel, Practice gaps
Introduction
Epidemiological context of enterovirus in Taiwanese preschool settings
Enterovirus infections represent one of the most significant public health concerns among preschool-aged children in Taiwan. Due to immature immunity, limited hygiene habits, and the close-contact nature of preschool environments, transmission risk is substantially elevated. National surveillance data from the Taiwan Centers for Disease Control (CDC) consistently show seasonal peaks during the spring and summer months, with most reported cases occurring in preschool settings [1]. Over the past decade, nationwide epidemiological surveys have further indicated that transmission rates of enteroviruses in childcare and early childhood education settings are markedly higher than in community environments, with cyclic fluctuations in the prevalence of Enterovirus A71 (EV-A71), various coxsackievirus serotypes (CVA), and other enteric viruses [2].
International studies similarly classify childcare centers as high-risk settings for enteric and respiratory infections. For example, a study conducted in Spanish childcare centers found that inadequate hand hygiene and intense interpersonal contact were strongly associated with clusters of acute respiratory and gastrointestinal infections [3]. Research from the Netherlands also demonstrated that preschool children attending day-care centers had several-fold higher infection risks than those cared for at home [4]. Common clinical presentations such as hand-foot-mouth disease and herpangina may lead to neurological complications in severe cases [5]. These findings underscore the critical role of preschools in national infection control systems.
Policy framework and practice gaps in preschool infection control
Taiwan’s government has established detailed guidelines for infection control in preschool settings, including case reporting criteria, class suspension standards, and environmental cleaning protocols [6]. Local education authorities have supplemented these guidelines with operational specifications; for instance, Taipei City mandates immediate class suspension and intensified disinfection when two confirmed cases occur within the same class [7]. However, analyses of cluster events conducted by the CDC continue to identify common failures such as symptom misinterpretation, delayed reporting, and inadequate disinfection [8]. These discrepancies highlight persistent gaps between policy expectations and real-world implementation in preschool environments.
Roles and challenges of childcare personnel in infection control
Childcare personnel serve as the primary agents of health management in preschool settings. Their responsibilities include daily monitoring of children’s health, teaching hygiene routines, conducting environmental cleaning, and communicating with parents. Existing studies show that infection risk increases when preschools experience inadequate ventilation, insufficient cleaning frequency, or high staffing burdens [9]. According to the Health Belief Model, if childcare personnel underestimate the severity of enterovirus illness or perceive infection control tasks as overly time-consuming, their motivation to implement recommended practices decreases [10]. Social Cognitive Theory further suggests that limited self-efficacy and insufficient external support can undermine the sustainability of infection control behaviors [11].
Purpose of the study
Most existing research centers on knowledge levels or the effectiveness of specific educational interventions, while fewer studies examine the actual practice gaps, error types, and the multilevel factors shaping childcare personnel’s infection control performance. Therefore, this narrative review synthesizes Taiwanese and international evidence to identify common types of infection control errors among childcare personnel, analyze influencing factors across individual, organizational, and familial contexts, and propose directions for policy development, professional training, and preschool management.
Methods
Study design
This narrative review synthesized empirical and policy literature on enterovirus infection control in Taiwanese preschool and childcare settings. A narrative approach was chosen to integrate heterogeneous study designs and to map common practice gaps, multilevel influencing factors, and implications for infection-control practice.
Data sources and search strategy
The literature search covered publications between January 2010 and December 2024 to capture contemporary infection-control practices in preschool and childcare environments. Databases included PubMed, Scopus, ERIC, ScienceDirect, Airiti Library, and the National Digital Library of Theses and Dissertations in Taiwan, supplemented by official documents from the Taiwan Centers for Disease Control (Taiwan CDC) and local education authorities. Bilingual keywords in Chinese and English were combined using Boolean operators, including terms such as “enterovirus”, “hand, foot and mouth disease”, “kindergarten”, “childcare center”, “childcare personnel”, “teacher”, “infection control”, and “Taiwan”.
Inclusion and exclusion criteria
Studies were eligible if they: (1) focused on preschool, kindergarten, or childcare settings; (2) examined enterovirus or related enteric or respiratory infections; (3) reported data on infection-control practices, errors, or influencing factors among childcare personnel, teachers, or caregivers; and (4) used a clearly described research method. Exclusion criteria were: (1) basic virology or clinical treatment studies; (2) studies without empirical or policy data; and (3) publications without accessible full texts.
Screening process and study selection
The selection process followed PRISMA principles, as detailed in Figure 1. The initial search identified 428 records. After removing duplicates, 316 unique records remained for title and abstract screening. Of these, 254 records were excluded as clearly irrelevant to infection control or early childhood settings. Sixty-two full-text articles and official reports were assessed for eligibility. Forty-one were excluded due to lack of relevant outcomes, inadequate methodological description, or non-preschool settings. A total of 21 studies met the inclusion criteria and were included in the final synthesis (Figure 1).
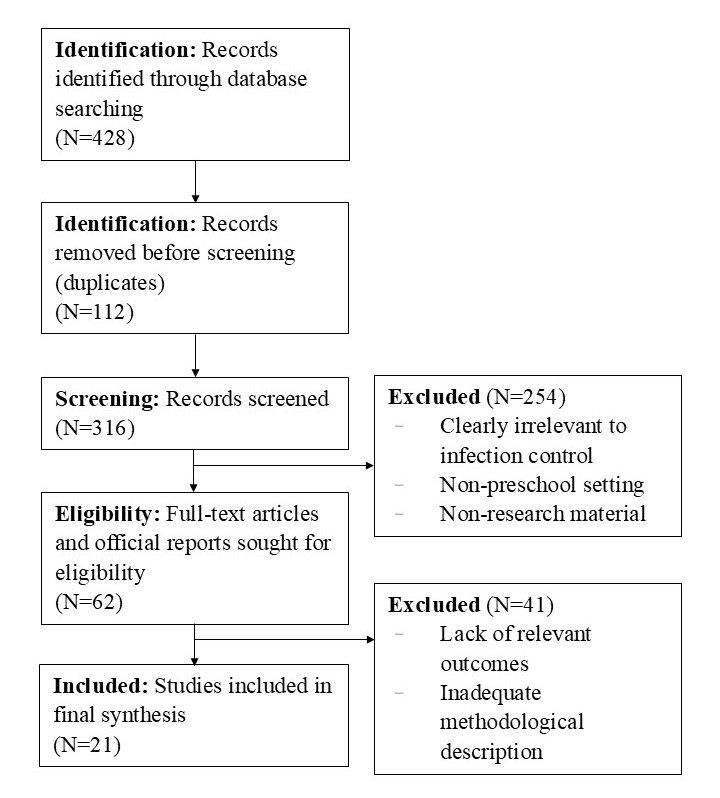
Figure 1. PRISMA flow diagram of study selection. This diagram illustrates the comprehensive process of identifying, screening, assessing eligibility, and including the studies and reports for the final narrative synthesis, conducted according to the PRISMA 2020 guidelines. (N=428 initial records; N=21 included studies).
Data extraction and thematic analysis
Data from the included studies were extracted into structured evidence tables summarizing study design, setting, participants, infection type, key findings on practice gaps, and reported influencing factors. A thematic analysis approach was then used to synthesize the evidence. Findings were grouped into three overarching domains: (1) common error types in infection-control practice; (2) individual-, organizational-, and policy-level determinants; and (3) suggested or evaluated strategies for improvement.
Results
This review synthesized evidence from 21 empirical studies and official reports (8 from Taiwan and 13 from international settings) on enterovirus and related infection control in preschool and childcare environments. For clarity, the findings are organized into two parts: Section 3.1 describes the common types of infection control errors among childcare personnel, and Section 3.2 summarizes the main factors that contribute to these errors at the individual, organizational, and policy/sociocultural levels, which are further outlined in Tables 1 and 2.
Common types of errors in enterovirus infection control among childcare personnel
Across the included studies and reports, three recurrent categories of infection control errors among childcare personnel were identified: (1) hygiene practices (hand hygiene and environmental cleaning); (2) symptom recognition and reporting; and (3) implementation of institutional procedures and communication. These categories are summarized in Table 1.
|
Error category |
Typical errors in preschool/childcare settings |
Representative references |
|
Hygiene practices (hand hygiene and environmental cleaning) |
Incomplete handwashing at key moments (before meals, after toileting, after contact with secretions); use of water only or incorrect technique; irregular or insufficient disinfection of toys, tabletops, and shared equipment; improper disinfectant dilution or inadequate ventilation. |
[3,4,8,12,13] |
|
Symptom recognition and reporting |
Difficulty recognizing early enterovirus symptoms; reliance on obvious rashes or high fever; uncertainty about oral ulcers and vesicular lesions; delayed exclusion or reporting of suspected cases. |
[5,8,9] |
|
Implementation of institutional procedures and communication |
Incomplete daily health checks and cleaning records; variable adherence to reporting and class-suspension criteria; unclear division of responsibilities for cleaning and health monitoring; fragmented communication with parents and local authorities. |
[6–8,13] |
Errors in hygiene practices
Childcare personnel frequently demonstrate gaps in basic hygiene practices, including incomplete handwashing at key moments and inconsistent environmental cleaning. Wu et al. [12] found that even after education, some staff could not consistently perform the seven-step handwashing technique, while Taiwan CDC outbreak investigations linked clusters to inadequate disinfection of toys, tabletops, and shared equipment or incorrect disinfectant dilution [8]. International trials in childcare and kindergarten settings have likewise shown that low baseline hand hygiene adherence among staff and children is associated with higher rates of enterovirus, HFMD, and other infections, and that structured hand hygiene interventions can significantly reduce infection incidence and illness-related absence [3,4,13].
Errors in symptom recognition and reporting
The literature indicates that childcare personnel often misinterpret early enterovirus symptoms and feel uncertain about clinical judgment. Hu et al. [5] reported that low-grade fever and oral discomfort were sometimes treated as common colds, resulting in delayed reporting and missed isolation opportunities, while Chen et al. [9] noted that many staff relied on parents to report symptoms and lacked confidence in recognizing oral ulcers and rashes. Such diagnostic uncertainty contributes directly to delayed action and the amplification of cluster risk.
Gaps in institutional implementation and communication
Even where comprehensive policies and guidelines exist, implementation at preschool level remains uneven. Taiwan CDC manuals and Taipei City regulations specify clear standards for daily health checks, environmental cleaning, reporting, and class suspension [6,7], but audit reports and outbreak investigations have revealed variability in compliance and delayed reporting due to concerns about parental dissatisfaction or enrollment [7,8]. These findings suggest that, without routine audits, designated responsible personnel, and supportive communication channels with families and local authorities, institutional procedures may remain superficial rather than embedded in daily practice. International systematic reviews of HFMD control in childcare facilities similarly emphasize that timely reporting, class or center closure, and stringent environmental cleaning are critical components of outbreak control yet are often implemented inconsistently in practice [14].
Key factors contributing to errors in infection control among childcare personnel
Across the included studies and official reports, the factors contributing to infection control errors among childcare personnel clustered into three interrelated levels: (1) individual factors related to knowledge, risk perception, and self-efficacy; (2) organizational factors such as staffing, workload, space, and material resources; and (3) policy and sociocultural factors, including parental cooperation, attendance pressures, and the feasibility of implementing guidelines. These multilevel determinants are summarized in Table 2.
|
Level |
Key factors |
Representative references |
|
Individual (knowledge, attitudes, self-efficacy) |
Enterovirus knowledge; perceived severity and susceptibility; perceived benefits and barriers; self-efficacy in performing hand hygiene, symptom assessment, and environmental cleaning. |
[10–12,15–17] |
|
Organizational (resources, workload, management systems) |
Child-to-staff ratios and workload; availability of sinks, soap, hand rubs, disinfectants, and adequate ventilation; presence of dedicated cleaning or health staff; clarity of roles and division of labor; monitoring, feedback, and auditing systems. |
[6–9,18] |
|
Policy, family, and sociocultural context |
Parental cooperation with exclusion and reporting; work-related and attendance pressures; cultural norms regarding “mild illness” and school attendance; alignment between home hygiene practices and school policies; cross-sectoral support from health and education authorities. |
[1,5–8,15,19–21] |
Individual level: Insufficient knowledge, attitudes, and self-efficacy
Training programs can improve childcare personnel’s knowledge and self-reported infection control behaviors, but the effects are often short-lived without continuous reinforcement. Wu et al. [12] showed that gains in hand hygiene behavior diminished over time, and international reviews have similarly found that hand hygiene interventions lose effectiveness without repeated practice and feedback [15,16,17]. From the perspective of the Health Belief Model and Social Cognitive Theory, low perceived severity, high perceived barriers, and limited self-efficacy make it difficult for staff to sustain recommended preventive behaviors in busy preschool environments [10,11].
Organizational level: Workforce and resource constraints
Organizational conditions strongly shape the feasibility of consistent infection control. Chen et al. [9] observed that high child-to-staff ratios and the absence of dedicated cleaning or health personnel forced childcare workers to prioritize direct care and teaching over thorough cleaning. The Danish Hi Five study further demonstrated that structured school systems—with standardized supplies, clear procedures, and monitoring mechanisms—significantly reduced infection rates [18], suggesting that institutionalized support is more effective than relying on individual motivation alone.
Policy and sociocultural level: Family cooperation and external pressures
At the policy and sociocultural level, parental cooperation and broader work and attendance pressures critically influence how infection control is implemented. Taiwan CDC reports indicate that some parents resist school-initiated exclusion or reporting because of work disruptions, thereby limiting timely preventive action [1,8]. Studies of parent-focused interventions have shown that when parents receive targeted hygiene education and structured support from schools, infection risks decrease and adherence to health policies improves [19–21]. These findings underscore that effective preschool infection control requires not only clear guidelines but also institutionalized parent-school collaboration and cross-sectoral support.
Discussion
This narrative review synthesizes evidence from 8 Taiwanese and 13 international studies to elucidate the common errors in enterovirus infection control and the systemic, multilevel factors contributing to these lapses. The findings move beyond describing individual deficits to offering a critical evaluation of organizational and sociocultural barriers.
Systemic nature of errors: Moving beyond individual deficiencies
Our synthesis confirms that the three categories of infection control errors (hygiene, symptom reporting, and procedural adherence) are recurrent patterns in preschool settings. Crucially, this review demonstrates that these errors do not stem from isolated individual deficiencies but emerge under conditions of high workload, time constraints, and competing responsibilities [5,8,12,17]. This dynamic interaction of factors highlights a complex behavioral system consistent with ecological and behavioral science frameworks emphasizing multilevel determinants of health behavior [10,11].
Organizational and cultural constraints hinder policy translation into practice
Although national guidelines specify requirements for school closure, cleaning procedures, and enterovirus reporting systems [6,7], the most critical finding is the substantial variability and failure in translating these well-established policies into routine practice. Limited staffing and administrative capacity directly impede this translation, with some preschools delaying reporting suspected cases to avoid enrollment and parental pressures [8]. Critically, institutional climate is closely tied to procedural adherence; without regular audits, designated health personnel, or systematic oversight, infection control becomes highly context-dependent. International evidence, such as the Danish Hi Five study [18] and a systematic review of best practices for HFMD control in childcare facilities [14], underscores that structured institutional systems—standardized procedures, environmental cleaning protocols, and clear criteria for exclusion and closure—are more effective than relying solely on individual motivation.
Sustainability challenge: Training requires contextual reinforcement and technological integration
Previous studies clearly indicate that initial hand hygiene training and infection control education can enhance compliance among childcare personnel [12]; however, the core challenge lies in sustainability, as these improvements diminish rapidly without continued supervision or practical reinforcement. International findings consistently demonstrate that interventions lose effectiveness without mechanisms for follow-up monitoring, replenishment of supplies, or behavioral practice [13,15,16]. This need for sustained reinforcement can be partially addressed by incorporating technological advancements: Graichen et al. [22] demonstrated that digital, multimodal hygiene interventions improved children’s handwashing accuracy. Therefore, future training must progress beyond one-time knowledge delivery toward contextualized and sustained professional development to meaningfully improve behavioral consistency.
The critical gap of family engagement and the need for institutionalized collaboration
Family engagement emerges as a core determinant of effective infection control. International literature consistently emphasizes the central role of parental involvement: studies show that parent-focused hygiene education and consistent parent–teacher communication significantly reduced infection risks [19], and institutionalized parental support initiatives improve adherence to school health policies [20,21]. The review therefore identifies insufficient parent–school collaboration as a critical and persistent gap within Taiwan’s preschool infection control system. Despite current policies calling for parental cooperation, they critically lack institutionalized, sustainable, and culturally responsive mechanisms to support family participation, leading to inconsistent and often superficial implementation [1,8].
Taken collectively, the findings of this review demonstrate that current infection control failures in early childhood settings are primarily structural and relational rather than due to individual ignorance. The recurrence of factors like high workload, organizational constraints, and family non-compliance underscores a fundamental need for multilayered interventions. Based on this critical synthesis, the following sections outline the limitations of the current literature and propose specific, actionable recommendations for policy makers and nursing professionals to build a more resilient infection control system.
Limitations
Several limitations of this review should be acknowledged. First, regarding the evidence base, a significant proportion of the included studies employed cross-sectional designs or relied on self-reported measures of hygiene compliance. This reliance limits the ability to establish causal relationships between specific interventions and infection reduction, and self-reporting may introduce social desirability bias. Second, methodological heterogeneity across the included literature—ranging from randomized controlled trials to policy analyses and qualitative interviews—precluded the use of quantitative meta-analysis. Consequently, the findings are based on narrative thematic synthesis rather than statistical aggregation. Third, geographical generalizability remains a consideration. While this review integrated 13 international studies to supplement the 8 Taiwanese studies, differences in cultural norms, educational systems, and parental leave policies may restrict the direct transferability of international findings to the local context. Finally, although the search strategy followed PRISMA principles, the exclusion of unpublished internal administrative reports or "grey literature" from individual preschools means that some localized, practical challenges may not be fully captured.
Implications and Recommendations
The findings of this review underscore that effective enterovirus infection control necessitates moving beyond enhancing individual knowledge to addressing structural, organizational, and relational barriers involving family cooperation. The results provide the following specific, actionable recommendations for policymakers, administrative leaders, and frontline healthcare and childcare professionals.
Policy and administrative level recommendations
These recommendations are aimed at dismantling the organizational constraints and enhancing the social safety net that limit infection control efficacy.
- Optimize Staffing and Support for Execution: Policymakers should evaluate and adjust the standard staff-to-child ratio to ensure childcare personnel have sufficient time to execute standard environmental cleaning and hand hygiene protocols consistently, especially during peak disease seasons or high-stress periods.
- Mandate Specialized Health Oversight: Local authorities should establish or fund a system of designated traveling health personnel (e.g., public health nurses) to conduct regular, mandatory audits (e.g., quarterly) of infection control practices in preschools and provide immediate, contextual professional guidance.
- Enhance Social Welfare for Isolation Compliance: The government should collaborate with labor departments to develop and subsidize more flexible, paid family sick leave or care allowance policies. This minimizes the financial incentive for parents to conceal a child’s illness, thereby encouraging strict compliance with home isolation policies.
Organizational management level recommendations
These recommendations focus on translating abstract policies into concrete, sustainable, and reliable institutional practices.
- Develop “Simple, Visible” Standardized Protocols: Administrators must translate complex national CDC guidelines into highly visual, concise “Just-in-Time Checklists” prominently displayed in critical areas (e.g., washing stations, isolation rooms). This ensures procedural adherence even under emergency or high-stress situations.
- Integrate Technological Assistance for Consistency: Institutions should incorporate simple technological aids (e.g., timers or digital reminders via an institutional application) to assist personnel in ensuring the accuracy and regularity of environmental disinfection timing, mitigating human error in manual record-keeping.
- Institutionalize Home-School Collaboration: Institutions should formalize the channels for parent-school communication by developing a unified digital platform. This platform should be used for real-time outbreak notification (e.g., anonymized case numbers) and daily reminders for parents to conduct rigorous symptom screening before dropping off children.
Clinical practice and training level recommendations
These recommendations address the challenge of converting theoretical knowledge into consistent behavioral practice.
- Implement “Contextual and Feedback-Driven” Training: Traditional, one-off knowledge lectures should be replaced by simulation-based training and drills. For instance, personnel should practice reporting and cleaning steps under simulated high-stress scenarios (e.g., a child vomiting or developing a fever) followed by immediate, constructive behavioral feedback.
- Shift to Objective Behavioral Audits: Nursing and health professionals should conduct regular (e.g., quarterly) behavioral observation audits in preschools, focusing on the observable execution of critical control measures (e.g., handwashing duration, correct use of bleach solutions), rather than relying solely on self-reported compliance. This is necessary to ensure that childcare personnel accurately translate knowledge into consistent clinical practice.
Conclusion
This narrative review successfully synthesized 21 empirical studies and policy documents to elucidate the systemic barriers to effective enterovirus infection control in preschool and childcare settings. The review’s principal conclusion is that infection control failures are primarily structural and relational—manifesting as insufficient resources, organizational constraints, and persistent family engagement gaps—rather than solely individual knowledge deficits. The findings confirm three recurrent categories of practice errors (hygiene, reporting, and procedural adherence) and delineate how they are influenced by interacting factors at the individual, organizational, and sociocultural levels. By systematically mapping these multilevel determinants, this review provides a crucial framework for shifting interventions from simple, knowledge-based training to evidence-based systemic reform. The actionable recommendations presented herein offer a roadmap for policymakers and health professionals to address the core structural issues, ultimately leading to a more resilient and effective infection control system essential for protecting public health in early childhood environments.
Funding
None.
Disclosure
The authors declare no financial relationships with any commercial entity related to the content of this article.
References
2. Liu FC, Chen BC, Huang YC, Huang SH, Chung RJ, Yu PC, et al. Epidemiological Survey of Enterovirus Infections in Taiwan From 2011 to 2020: Retrospective Study. JMIR Public Health Surveill. 2024 Sep 5;10:e59449.
3. Azor-Martinez E, Yui-Hifume R, Muñoz-Vico FJ, Jimenez-Noguera E, Strizzi JM, Martinez-Martinez I, et al. Effectiveness of a Hand Hygiene Program at Child Care Centers: A Cluster Randomized Trial. Pediatrics. 2018 Nov;142(5):e20181245.
4. Zomer TP, Erasmus V, Looman CW, Tjon-A-Tsien A, Van Beeck EF, De Graaf JM, et al. A hand hygiene intervention to reduce infections in child daycare: a randomized controlled trial. Epidemiol Infect. 2015 Sep;143(12):2494–502.
5. Hu YL, Chen CM, Wang ET, Kuo HW, Shih WL, Fang CT, et al. The secular trend of enterovirus A71 after the implementation of preventive measures in Taiwan. BMC Public Health. 2022 Aug 4;22(1):1483.
6. Taiwan Centers for Disease Control. Enterovirus prevention manual for school and preschool educators. Taiwan: Taiwan Centers for Disease Control; 2013 (Accessed on March 13, 2025). Retrieved from: https://www.cdc.gov.tw/uploads/files/184739bf-a902-49f3-8539-afd1c3d95c67.pdf.
7. Taipei City Department of Education. Standards and procedures for suspension due to enterovirus infection. Taipei: Taipei City Department of Education; 2023 (Accessed on March 13, 2025). Retrieved From: https://www.doe.gov.taipei/News_Content.aspx?n=FDDC0C0019D7F096&s=3C3BB4641126384E.
8. Taiwan Centers for Disease Control. Investigation of an enterovirus outbreak in an infant daycare center, 2022. Taiwan: Taiwan Centers for Disease Control; 2022 (Accessed on March 13, 2025). Retrieved From: https://www.cdc.gov.tw/En/Category/ListContent/dwCswoLnYw874U8oPrVAPA?uaid=iC_6X_mu8y8tjHRUCBpyxA.
9. Chen CY, Chen JK, Chio CP, Chen PC, Su TC, Chan CC. COVID-19 Infection Risk Assessment in a Kindergarten Utilizing Continuous Air Quality Monitoring Data. Indoor Air. 2024;2024(1):1779971.
10. Rosenstock IM, Strecher VJ, Becker MH. Social learning theory and the Health Belief Model. Health Educ Q. 1988 Summer;15(2):175–83.
11. Bandura A. Health promotion from the perspective of social cognitive theory. Psychology & Health. 1998;13(4):623–49.
12. Wu S, Wang RS, Huang YN, Wan TTH, Tung TH, Wang BL. Effect of Hand Hygiene Intervention in Community Kindergartens: A Quasi-Experimental Study. Int J Environ Res Public Health. 2022 Nov 8;19(22):14639.
13. Liu X, Hou W, Zhao Z, Cheng J, van Beeck EF, Peng X, et al. A hand hygiene intervention to decrease hand, foot and mouth disease and absence due to sickness among kindergarteners in China: A cluster-randomized controlled trial. J Infect. 2019 Jan;78(1):19–26.
14. Chan JH, Law CK, Hamblion E, Fung H, Rudge J. Best practices to prevent transmission and control outbreaks of hand, foot, and mouth disease in childcare facilities: a systematic review. Hong Kong Med J. 2017 Apr;23(2):177–90.
15. Willmott M, Nicholson A, Busse H, MacArthur GJ, Brookes S, Campbell R. Effectiveness of hand hygiene interventions in reducing illness absence among children in educational settings: a systematic review and meta-analysis. Arch Dis Child. 2016 Jan;101(1):42–50.
16. Chittleborough CR, Nicholson AL, Young E, Bell S, Campbell R. Implementation of an educational intervention to improve hand washing in primary schools: process evaluation within a randomised controlled trial. BMC Public Health. 2013 Aug 15;13:757.
17. Tahoun MM, Hasab AAH, El-Nimr NA. Infection control in child daycare centers: logistics, knowledge, and practices of caregivers. J Egypt Public Health Assoc. 2019 May 3;94(1):16.
18. Johansen A, Denbæk AM, Bonnesen CT, Due P. The Hi Five study: design of a school-based randomized trial to reduce infections and improve hygiene and well-being among 6-15 year olds in Denmark. BMC Public Health. 2015 Mar 1;15:207.
19. Zhang L, Qin X, Zeng J, Feng Y, Zhang N, Tan Y, et al. A kindergarten-based, family-involved intervention to improve children's hand hygiene behavior: A cluster-randomized controlled trial. Public Health Nurs. 2021 Sep;38(5):738–50.
20. Norman Å, Malek ME, Nyberg G, Patterson E, Elinder LS. Effects of Universal School-Based Parental Support for Children's Healthy Diet and Physical Activity-the Healthy School Start Plus Cluster-Randomised Controlled Trial. Prev Sci. 2024 Aug;25(6):963–77.
21. Kobel S, Lämmle C, Wartha O, Kesztyüs D, Wirt T, Steinacker JM. Effects of a Randomised Controlled School-Based Health Promotion Intervention on Obesity Related Behavioural Outcomes of Children with Migration Background. J Immigr Minor Health. 2017 Apr;19(2):254–62.
22. Graichen J, Stingl C, Pakarinen A, Rosio R, Terho K, Günther SA, et al. Improving hand hygiene of young children with a digital intervention: a cluster-randomised controlled field trial. Sci Rep. 2024 Mar 14;14(1):6157.