Abstract
Cryoablation of breast cancer offers an alternative to surgery for women who are not ideal surgical candidates. It is a minimally invasive procedure that has already had success in fibroadenoma treatment with good tumor reduction and cosmesis. The findings of cryoablation as treatment for early-stage, low-risk breast cancer has been previously discussed in the recently published article ‘Cryoablation: A promising non-operative therapy for low-risk breast cancer’. This commentary updates on the previous study and expands on potential therapeutic benefits of cryoablation as a whole.
Keywords
Breast Cancer, Cryoablation, ER+PR+HER2+, Abscopal effect
Commentary
Cryoablation of breast cancer offers an alternative to surgery for women who are not surgical candidates due to comorbidities, age, or refusal of surgery. Cryoablation is a minimally invasive procedure that induces target tissue necrosis through freeze/thaw cycles while preserving surrounding tissue architecture. The procedure is performed using ultrasound in two orthogonal views to ensure that the probe tip is advanced through the center of the tumor mass for accurate ice-ball formation to completely freeze diseased tissue with minimal effect on healthy tissue [1]. Imaging changes during cryoablation ice-ball formation include decreased echogenicity on ultrasound and increased density on mammogram [1]. Measuring the image modality changes during the procedure and comparing it to tumor sizing can be used as an indicator for complete cryoablation [1]. The procedure only requires local anesthetic and can be completed in outpatient clinic between 30 min to an hour. Additionally, cryoablation provides a more financially feasible option for patients with less potential health risks posed due to its completion in the clinic as opposed to the operating room.
Prior to our study, cryoablation already had success in fibroadenoma treatment with good tumor volume reduction and cosmesis [2]. It has been shown that fibroadenoma lesions less than 2 cm show the most optimal response, without residual tumor tissue [2,3] In Sheth et al., most fibroadenomas were resorbed by 18 months post cryoablation, becoming indistinguishable from the background echotexture on ultrasound follow-up [3]. Poplack et al. found that cryoablation in invasive ductal carcinomas (IDCA) up to 15 mm was well tolerated by patients with a failure rate of 15% [4]. Recurrence was associated with ductal carcinoma in situ (DCIS) presence outside of the original cryoablation field [4]. Sabel et al. agreed with the patient tolerability of cryoablation and stated that cryoablation be limited to patients with IDCA <1.5 cm and <25% DCIS [5]. Currently, there are two major clinical trials assessing cryoablation in breast cancer patients: Cryoablation of Small Breast Tumors in Early-Stage Breast Cancer (FROST) and Cryoablation of Low-Risk Small Breast Cancer (Ice3 Trial) [6,7]. FROST examines the use of cryoablation for treatment in early-stage invasive breast cancer [6] while Ice3 Trial focuses on the use of cryoablation without lumpectomy and its impact on local and distant recurrence of breast cancer [7].
For our study, we recruited patients >50-year-old with estrogen receptor-positive (ER+), progesterone receptor-positive (PR+), and HER 2-negative (HER2-) IDCA that had a unifocal tumor without excessive in situ component and were visible on ultrasound [8]. Up to the time of this commentary, 34 patients met the eligibility criteria and 15 (44.1%) agreed to participate in the study. All 15 patients underwent the cryoablation procedure outlined in the original article [8] with minimal post-procedure complaints including mild soreness and bruising. There were no cases of infection or skin necrosis. Only one of these patients underwent sentinel node biopsy for staging. All patients were given adjuvant systemic endocrine therapy. Thirteen of 15 patients (86.7 %) had 6-month imaging (mammogram, ultrasound, and MRI) and clinical follow-up with no identifiable residual disease and 5 patients (33.3%) have completed a 2-year follow-up with no residual disease at the primary site. One patient presented with axillary disease at 2-year follow up and underwent axillary dissection with 2 out of 17 nodes positive. She had remained non-compliant with endocrine therapy after three doses. Seven patients consented to a 6-month follow-up biopsy of primary tumor bed, which showed fat necrosis and no identifiable viable tumor.
Ablative techniques may serve as viable alternatives to surgical resection, particularly in the case of early-stage, low-risk cancers. Of these, cryoablation is the best visualized due to the phase change during ice-ball formation. The margins of low-density, solid ice are visualized well with various imaging modalities, including US, CT, and MRI [9-11]. Additionally, cryoablation provides an analgesic effect compared to other ablation techniques due to its freezing of surrounding tissue [12]. Lanza et al. found that compared to radiofrequency, cryoablation can be done on an outpatient basis while still providing a good margin for small (<15 mm) ductal tumors and is a competitive alternative to surgical resection [13]. Our experience is in agreement in regards to the effectiveness of cryoablation compared to surgical resection on short-term follow up. However, it is important to note that patients with extensive cancer with indefinite margins are not good candidates for cryoablation [12].
An additional advantage of cryoablation is that unlike thermal-heat ablation which denatures tumor antigens, cryoablation rapidly deep-freezes (<-40ºC) the tumor killing it while preserving potential cancer antigens. Since the ablated tumor remains in the patient, this introduces the potential for augmentation of an immune response to tumor antigens still present [14]. Kumar et al. shared a case highlighting the potential abscopal effect of cryoablation [15]. The abscopal effect is the phenomenon where local treatment of the primary tumor leads to an increased systemic immune response thereby affecting potential metastases [Figure 1]. However, the magnitude of immune stimulation needed to provide a successful systemic immune response to prevent metastasis may be insufficient from cryoablation alone [16]. Additional immune stimulation may be needed to allow recognition of the new cryoablated tumor-associated antigens and respond to potential metastases. Currently, the use of immune modulators such as checkpoint inhibitors that target PD-1, PD-L1 or CTLA-4 are being explored in conjunction with cryoablation to enhance the anti-tumor response. Checkpoint inhibitors may be particularly advantageous for more immunogenic tumors such as high risk metastatic triple-negative and HER2+ subtypes. McArthur et al. previously demonstrate that a preoperative single dose of Ipilimumab (anti-CTLA4 antibody) in combination with cryoablation was safe with potentially favorable intra-tumoral and systemic immunological effects [17].
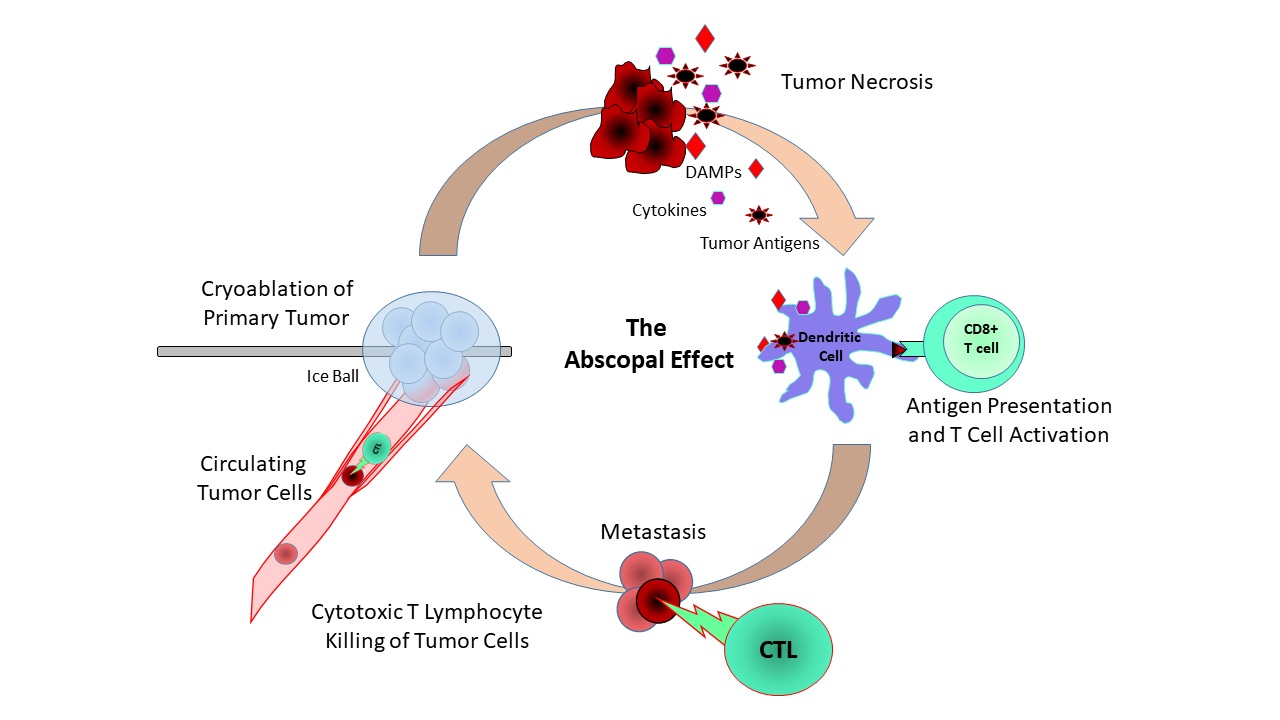
Figure 1: The Abscopal Effect. Cryoablation of the primary tumor induces necrosis. The dying tumor releases tumor antigens, damage signal molecules (DAMPs) and cytokines. Antigen presenting cells take up theses antigens and then activate T cells. These anti-tumor cytotoxic T cells (CTLs) then target circulating tumor cells (CTCs) and distant cancer metastasis.
As interest in cryoablation as an alternative to breast cancer surgery increases including high-risk cancers, new approaches to identify best candidates and monitor the patient will be needed. The immunological tumor microenvironment, tumor infiltrating lymphocytes (TILs), and the cytotoxic T cell (CTL) responses in breast cancer are becoming increasingly relevant as predictive/prognostic biomarkers as well as new therapeutic targets. Post-cryoablation biopsy of the tumor microenvironment could be analyzed via RNA-sequencing to determine immunological response changes to predict long-term outcomes. RNA-sequencing analysis could be paired with already established breast cancer databases such as Tumor IMmune Estimation Resource (TIMER) to analyze the immune and TIL responses with emphases on activated CD8+ T cell (CTLs) gene signatures. Circulating tumor cells (CTCs) are gaining promise as a liquid biopsy approach for the prognosis and personalized treatment of cancer [18]. A patient’s blood sample could be collected pre- and post-cryoablation and its CTCs enumerated using a combination of biomarkers such as, epithelial cellular adhesion molecule (EpCAM), N-cadherin, CD44 and negative for CD45 [19]. CTL counts in conjunction with CTCs could then be used to measure the effectiveness of the immune response post-cryoablation (quantifying the abscopal effect). An effective treatment would result in increased activated CTLs with decreased number of CTCs post therapy compared to pretreatment levels.
The use of cryoablation to treat breast cancer is starting to get more attention. Our recent clinical study showed cryoablation without tumor resection of early-stage, low-risk (ER+, PR+, and HER2-) breast cancer is a safe alternative to surgery. With improved cryoablation techniques and the use of combination immunotherapy, it is conceivable the abscopal effect could be maximized to target highly immunogenic cancers such as triple-negative and HER 2-positive breast cancer.
Conflict of Interest
There are no conflicts of interests.
References
2. Kaufman CS, Littrup PJ, Freman-Gibb LA, Francescatti D, Stocks LH, Smith JS, et al. Office-based cryoablation of breast fibroadenomas: 12-month followup. Journal of the American College of Surgeons. 2004 Jun 1;198(6):914-23.
3. Sheth M, Lodhi U, Chen B, Park Y, McElligott S. Initial Institutional Experience With Cryoablation Therapy for Breast Fibroadenomas: Technique, Molecular Science, and Post‐Therapy Imaging Follow‐up. Journal of Ultrasound in Medicine. 2019 Oct;38(10):2769-76
4. Poplack SP, Levine GM, Henry L, Wells WA, Heinemann FS, Hanna CM, et al. A pilot study of ultrasound-guided cryoablation of invasive ductal carcinomas up to 15 mm with MRI follow-up and subsequent surgical resection. American Journal of Roentgenology. 2015 May;204(5):1100-8.
5. Sabel MS, Kaufman CS, Whitworth P, Chang H, Stocks LH, Simmons R, et al. Cryoablation of early-stage breast cancer: work-in-progress report of a multi-institutional trial. Annals of Surgical Oncology. 2004 May;11(5):542-9.
6. Clinicaltrials.gov. Cryoablation of Small Breast Tumors in Early Stage Breast Cancer (FROST). Identifier: NCT01992250. Available from: https://clinicaltrials.gov/ct2/show/NCT01992250..
7. Clinicaltrials.gov. Cryoablation of Low Risk Small Breast Cancer- Ice3 Trial. Identifier: NCT02200705. Available from: https://clinicaltrials.gov/ct2/show/NCT02200705.
8. Habrawi Z, Melkus MW, Khan S, Henderson J, Brandi L, Chu V, Rahman RL. Cryoablation: a promising non-operative therapy for low-risk breast cancer. The American Journal of Surgery. 2021 Jan 1;221(1):127-33.
9. Kaiser WA, Pfleiderer SO, Baltzer PA. MRI-guided interventions of the breast. Journal of Magnetic Resonance Imaging: An Official Journal of the International Society for Magnetic Resonance in Medicine. 2008 Feb;27(2):347-55.
10. Littrup PJ, Ahmed A, Aoun HD, Noujaim DL, Harb T, Nakat S, et al. CT-guided percutaneous cryotherapy of renal masses. Journal of Vascular and Interventional Radiology. 2007 Mar 1;18(3):383-92.
11. Permpongkosol S, Nicol TL, Khurana H, Link RE, Zhai QJ, Kavoussi LR, et al. Thermal maps around two adjacent cryoprobes creating overlapping ablations in porcine liver, lung, and kidney. Journal of Vascular and Interventional Radiology. 2007 Feb 1;18(2):283-7.
12. Pusceddu C, Paliogiannis P, Nigri G, Fancellu A. Cryoablation in the management of breast cancer: evidence to date. Breast Cancer: Targets and Therapy. 2019;11:283.
13. Lanza E, Palussiere J, Buy X, Grasso RF, Zobel BB, Poretti D, et al. Percutaneous image-guided cryoablation of breast cancer: a systematic review. Journal of Vascular and Interventional Radiology. 2015 Nov 1;26(11):1652-7.
14. Lees JS, Dooley WC. Nonsurgical ablation of primary breast cancer. Surgical Oncology Clinics. 2005 Feb 1;14(1):33-44.
15. Kumar AV, Patterson SG, Plaza MJ. Abscopal Effect following Cryoablation of Breast Cancer. Journal of Vascular and Interventional Radiology: JVIR. 2019 Mar 1;30(3):466-9.
16. Sabel MS. Cryo-immunology: a review of the literature and proposed mechanisms for stimulatory versus suppressive immune responses. Cryobiology. 2009 Feb 1;58(1):1-1.
17. McArthur HL, Diab A, Page DB, Yuan J, Solomon SB, Sacchini V, et al. A pilot study of preoperative single-dose ipilimumab and/or cryoablation in women with early-stage breast cancer with comprehensive immune profiling. Clinical Cancer Research. 2016 Dec 1;22(23):5729-37.
18. Alix-Panabieres C. The future of liquid biopsy. Nature. 2020 Mar 1;579(7800):S9.
19. Barriere G, Fici P, Gallerani G, Fabbri F, Zoli W, Rigaud M. Circulating tumor cells and epithelial, mesenchymal and stemness markers: characterization of cell subpopulations. Annals of Translational Medicine. 2014 Nov;2(11).