Commentary
In an earlier publication, gastronomy is proffered, although rarely considered, as having a place in clinical practice of medicine and surgery with an indirect role in conferring interventions to compensate for the adverse effects of smell and taste alterations in cancer chemotherapy on nutrient intake [1].
Eating involves multimodal integration of diverse disciplines such that any loss of sensory functions occurring can impact the ingestive process. Heston Blumenthal on his tasting menu at his Fat Duck Restaurant at Bray espouses that:
“eating is the only thing that invokes all the senses. I don’t know that we realize just how much influence the senses have on the way we process information from the mouth to the brain” [2].
These senses can be disrupted through physiological, psychological, social, diseases, and treatment factors. Major changes occur in chemotherapy in which all of the senses become challenged by the nature of the treatment to greater or lesser extents, with those commonly reported being smell and taste alterations and peripheral neuropathies.
In considering the management of the side effects of chemotherapy including smell and taste alterations (STAs) and nausea the extensive scope of multimodal influences and cues on ingestive behaviors need to be considered. Some act as direct influences, whereas others confer indirect effects. This commentary considers the scope of intrinsic influences involved in consuming a meal influenced by chemotherapy, along with the role of oral function and considers the benefits of extrinsic aspects of gastronomy as potential interventions.
In oncology, nutrition care is vital as nutrition-related issues significantly impact clinical and patient outcomes. Implementation of nutrition care is inconsistent, which can lead to inequalities in care [3]. Despite modern cancer care leading to improved survival times, nutrition care, a simple supportive measure, remains largely overlooked. Malnutrition is a common side-effect resulting from smell and taste alterations arising from chemotherapy which when compounded with malignant cachexia provides poor outcomes for patients.
A major problem exists in some cancer treatments in which patients have lost their appetite through several routes, considered to be altered eating. A common factor in altered eating is loss or smell and taste along with altered ‘mouthfeel’ resulting in loss of the pleasure of ‘the meal’ with subsequent diminished nutrient intake or inappropriate intake. Altered eating with alterations of smell, taste and touch become a major problem to the patient and those involved with its management as they are notoriously difficult to overcome directly.
The clinical nutrition market offers different food supplements, whilst addressing nutrition these products do not fulfil pleasure and purpose (self-esteem) of ‘a meal’ by addressing holistic requirement [1].
Eating is greatly influenced by non-homeostatic signals that convey information relating to learning and experience, hedonics, stress, the social situation opportunity and many other factors [4]. Flavor is recognized for its role in ingestive behaviors, comprising 85–95% smell [5], on a backbone of taste and haptic somatosenses along with small input of the senses of sight and hearing.
The complex nature of the ingestive process considered to govern a meal represents multimodal and multidisciplinary inter-twined actions ranging from the physiology of eating, knowledge, social and psychosocial influences. Accordingly, a meal is holistic and involves more than the act of eating and drinking and comprises many multimodal influences and cues including not only the food itself, but the process involved and the environment in which it is consumed. The act of eating cannot be restricted to nutritional and sensory aspects alone. It also includes a psychoaffective dimension, which relates to the context in which the meal is served [6].
Currently, the emphasis of intervention to ameliorate smell and taste alterations and improve nutrient intake have been directed mainly to the intrinsic properties of food and beverages comprising flavor and texture, being product specific attributes. Results with this approach have been incomplete and lacking consistency in improving effective appetite and nutritional intakes [7]; the outcomes appear to be little changed and current data is lacking.
The multidisciplinary nature of this commentary precluded the use of reporting systems commonly applied to health interventions, e.g., PRISMA. The literature cited emanated through extensive searching of various topics including Scopus, Web of Science, PubMed and Google Scholar and developing personal databases within EndNote. Major topics were classified as sensory studies with a focus on the chemical senses, influences of cancer treatment on smell and taste, altered eating, gastronomic studies of eating behavior including neurogastronomy and gastrophysics, and ‘the meal’. A cautious approach was taken to minimize bias. This commentary hopefully evokes thought and comment in an area with little crosspollinated research.
Flavor & intrinsic properties of food and beverages
The multimodal influences and cues on ingestive behaviors of a meal are shown in Figure 1 with flavor and oral function representing properties and factors contributing to the release and perception of the intrinsic properties.
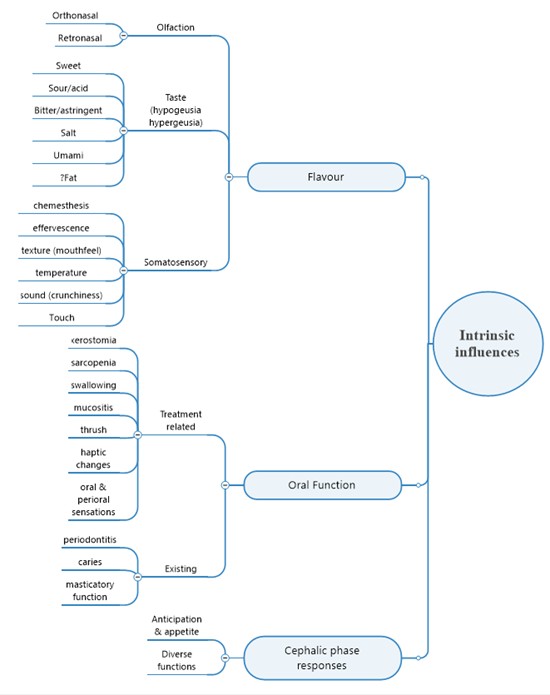
Figure 1. Displays the senses and their scope of involvement in the perception of the intrinsic properties of flavor of food and beverages -- considered as ‘product specific attributes’. Chemotherapy can alter any of these senses.
Oral function is important in the generation of flavors but is compromised by side effects of chemotherapy and preexisting conditions.
Cephalic phase responses are influenced by changes in the perception of intrinsic properties with impacts on many covert function but noticeable in anticipation and appetite.
The intrinsic influences of ‘a meal’ are derived from the inherent odorants and tastants of the food and beverages. To reiterate, flavor generation involves all of the senses to greater or lesser extents with smell, olfaction representing the major contributor on an essential backbone of physiological taste, gustation, influenced by the somatosenses, haptic senses, and influence by visual and auditory cues. Flavor can be considered as a neural image resulting from the melding of the various senses in the brain and referred to the mouth where it is perceived [8,9].
Olfaction, the sense of smell, is obtained through two routes. Through the front of the nose, the nares, from the external environment influencing anticipation and appetite, and via the choanae from the mouth through the nasopharynx with smell originating from the intrinsic properties of food and beverages and those derived through oral processing.
Vision and sound can attenuate this image. Plating of food is well recognized to enhance perception of flavor, as is the crispness of chewed food demonstrated in study with Pringles® [10].
Other factors important for flavor release comprising are the temperature of food and the effects of effervescence.
Oral processing and function
Food is masticated, lubricated with saliva and formed into a bolus to enable safe swallowing. During this process odorants and tastants are directly released from the food (and beverage) or through various enzyme or microbiome actions in the mouth.
Oral processing and function are important areas both in normal life and become disrupted during chemotherapy. Commonly reported effects of chemotherapy are xerostomia, dry mouth and changes in saliva volumes and composition, impacting both the generation of flavor perception and influencing the microbiome composition responsible for the generation of flavor.
Oral health is necessary for oral sensations, but deviation from good oral hygiene and health status can significantly impact oral sensation. The number of teeth and healthy supporting structures, periodontium, are essential for effective masticatory function to comminute food and release odorants and tastants and obtain texture suitable for bolus formation to facilitate swallowing.
Cephalic phase responses
The cephalic phase responses are closely related to the cues derived from smell and from visual and anticipatory cues. Along with their numerous responses, they directly influence salivation, and responses involved in anticipation and appetite. The role of cephalic phase optimal assimilation of ingested food, especially glucose, is presented in a recent article [11].
Extrinsic factors
Extrinsic factors influencing a meal are represented in Figure 2 as the external attributes of eating and drinking comprising diverse factors which can have significant influences on meaningful eating and drinking. Many of these are considered to be within the remit of gastronomy and gastrophysics.
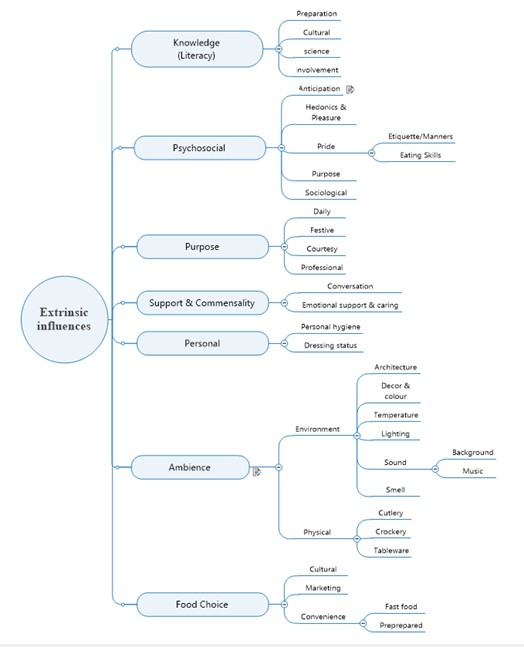
Figure 2. Outlines the various factors considered as extrinsic factors involved in 'a meal'. It comprises a range of factors, not considered to be complete, including knowledge, psychosociology, purpose, support, personal, and ambience along with food choice.
Gastronomic aspects
The current use of the term ‘gastronomy’ is bandied around in marketing, tourism and ‘snobbery’ resulting in a departure from its scientific origins. Barbara Santich 2007 [12] clearly annunciates that the etymology of the term and the study of its historical usage demonstrates that gastronomy is not directly focused on food and that the study of gastronomy is not the study of food per se, but is focused on people through the involvement of humans in diverse aspects associated with ‘consumption’ and she cites from Brillat-Savarin’s 1826/1865 [13] interpretation of gastronomy ‘la connaissance rationnée de tout ce qui a rapport à l’homme, en tant qu’il se nourrit’ (the reasoned understanding of everything that concerns us insofar as we sustain ourselves. Fischler 1980 [14] considers that gastronomy represents the set of rules, norms, and meanings associated with food (and beverages) and acting as constraints upon food habits.
In short, gastronomy involves why we eat, how we eat, with whom we eat, where we eat and what we eat. In the context of this commentary, it is considered as an all-encompassing term.
In relationship to the relevance and value of extrinsic factors in conferring a role in amelioration of STAs in chemotherapy various aspects will be reviewed below (Figure 2).
Knowledge and literacy
Knowledge of food and beverages represents an essential aspect of gastronomy and covers the obtaining and preparation of foods and beverages along with cultural implications encompasses preparation, culture and science. It covers nutrition and dietary needs and is strongly influenced by culture and religion.
Involvement to enhance knowledge and literacy can involve several directions. On successful program with patients with head and neck cancers involved ‘food play’ [15]. The kitchen is proposed as therapy [16] in which chemotherapy-treated patients participating in an integrative cuisine workshop program showed improved quality of life outcomes, including emotional-related symptoms along with a reduction in nutritional and functional concerns. Increased knowledge and awareness of nutrition benefited patients at home.
Psychosocial
Chemotherapy induces significant psychosocial stresses, including high rates of anxiety, depression, cognitive impairment ("chemo-brain"), and fear of recurrence. Patients often experience diminished quality of life, role changes, and severe treatment-related side effects. Addressing these needs through psycho-oncology support, counselling, and social support is crucial. Support helps patients and families manage the emotional, social, and cognitive impacts of cancer, offering counselling for anxiety, depression, and treatment-related distress.
Depression is significant effect of both cancer, and its treatment, with loss of olfactory sense being commonly associated with depression [17,18].
An excellent overview is presented by covering the Emotions Studied in Context and the role of the Eating Environment [19].
Purpose
In relation to loss of smell and taste alterations, reinforcement of the purpose of the occasion of eating can be directed to encourage involvement in the occasion and should be considered as a meaningful activity be it a family meal or a special event.
A significant part of daily eating behaviors consists of habits [20] and that eating at a regular times encourages metabolic stability, and the harnessing social norms are encouraged to promote healthier eating [21]; maintaining habits should be used to encourage nutritional intake in STAs.
Eating behavior is strongly influenced by social context. We eat differently when we are with other people compared with when we eat alone [21]. We also eat differently depending on the reason for a meal, be it daily routine, festive such as a celebration of a birthday, etc. Some meals encompass a courtesy or a professional role.
The contextual factors relating to the setting of a meal contributes significantly to food acceptance this is demonstrated when identical food is presented in various settings ranging from army training camps through to hotel four-star restaurants receiving higher ratings the ‘better’ the dining facility [19].
Support and commensality
As eating behavior is profoundly affected by social influences and that dynamic interplay exists between eating companions [22] involvement of person with STAs could benefit through social mimicry rather than eating in isolation. Conversation can provide meaningful benefits in detracting from the problem of eating.
Personal
In cases of STAs, personal hygiene may become a problem which is unrecognized by the subject [17] and is associated with depression and diminished self esteem. Encouring dressing for a meal and indeed relinquishing casual or night attire enhances self-esteem (Pers Obs).
Ambience and atmosphere
Ambience and atmosphere comprise a large component of extrinsic factors in enhancing both psychological and sensory modulation. Ambience has a major influence on eating behavior [23]. Gastrophysics consider many of these interactions.
Ambience and atmosphere are well recognized in the restaurant and hospitality industries, and much can be emulated within healing environments, in both clinical facilities and in the homes of chemotherapy patients.
The scope ranges from aspects of the environment through to the physical elements involved in ‘the table’.
Architecture
Despite much is undertaken concerning hospital architecture regarding the logistics of clinical facilities, limited scientific research exists confirming design solutions for creating healing spaces and the cross-disciplinary aspects of ‘ingestive behaviors’ in determining hospital design to facilitate patient healing and recovery [24]. ‘The environment cannot cause healing to occur but can facilitate engagement in behaviours and emotions that support healing; the environment can induce physical and emotional responses such as happiness, joy, and relaxation; and the built environment can enhance individual control and functionality, all of which are antecedents to healing’ [25].
Décor
Hospitals primarily use calming, nature-inspired colors such as soft blues, greens, and neutral tones (beige, warm grey) to reduce stress, lower heart rates, and promote healing in patient rooms and waiting areas, their influence on ingestive behaviors appears to be lacking.
Use of drapes and carpets are good at buffering sounds common in clinical situations but are constrained through infection control.
Temperature
The ambient temperature in which eating and drinking occurs can influence appetite and diminish calorie intake. A comfortable temperature, considered to be between 20 to 25oC encourages a slower more leisurely pace.
Lighting
Lighting impacts not only the ambiance and mood of a dining space but also food choices, consumption speed, and the perception of taste; it affects what is consumed and the calorie intake. Dim lighting creates a relaxing atmosphere; bright lighting used in quick turnover cafes creates a faster paced environment, whereas warm lighting sets a more inviting environment and enhances the visual appearance of food. The concept of lighting in the healing environment in relation to eating and drinking is largely absent in the literature.
Sound
Music and sound impinge upon our body and our mind, and we can react to both either positively or negatively. Much depends on the frequency spectrum and the level of the sound stimuli, which may sometimes make it possible to set music apart from noise [26].
Noise
Background sounds include clutter, machinery, gongs, PA systems and in most healing environments which are concrete and glass lacking buffering with fabrics can have adverse effects on the senses and wellbeing.
Music
Concordant sounds of music have significant influences on flavor of food and beverages. Wine and beer flavors are modulated by music [27,28]. The concept of ‘sonic seasoning’ refers to the way in which music can influence multisensory tasting experiences by triggering a combination of cross-modal and emotional effects on multisensory tasting [29]. Music can support relaxation or change mood and seems to influence the amount of food and fluid consumed [23].
Smell of environment
Smell and taste alterations affect patients in diverse ways and the various smells in a healing environment can heighten anxiety and trigger stress with sick-building syndrome [30] recognized in some environments including hospitals and dental surgeries.
Physical aspects of “the table” – tablescape
The table setting should be considered as important in the clinical setting as it is in restaurants.
Cutlery
Each component of the setting confers properties to the perception of food.
Cutlery weight is known to enhance flavor perception as well recognized in the comparison between plastic knives, forks, and spoons. A very common set of utensils, present on tables around the world, can potentially make the food ‘taste’ better (or worse) [31]. This is well recognized in BBQ events and in airline travel. Many of the studies in this respect have been undertaken by Spence and various coworkers and some are recorded in Gastrophysics [32]. Heavy cutlery may be advantageous to patients with motor tremor problems and finger sensory alterations. In cases of ‘metal-mouth’ metal cutlery is considered as inappropriate [33] literature regarding metallic taste among chemotherapy treated cancer patients is scarce, but it likely originates from the chemotherapy rather than the cutlery.
In certain instances, hands are used to transfer food to the mouth instead of cutlery, remembering that the hands represent a significant proportion of the sensory homunculus followed closely by the lips and the tip of the tongue. This tactile sensation with certain foods, breaking bread, eating croissants, hamburgers and chips is rewarding and enhances the eating experience although effects with patients having peripheral neuropathies affecting fingers are not reported.
Crockery
The shape and color of the plate on which the food is served can affect how much diners enjoy food. Plate shape and color interact to influence taste and quality judgments [34].
Tableware
Table linen is considered to have a significantly positive impact on the meal experience as compared to a paper one [35]. Other considerations are the presence of discrete floral and other arrangements.
Food choice and involvement
Food choice and active involvement in nutrition during chemotherapy are crucial for managing side effects, maintaining strength, and supporting immune function. Choice must reflect cultural and religious aspects of eating. Involvement in the obtaining and preparation also relate to ‘food-play’ [15]. Convenience foods should not form a staple diet. Continue with normal life and involve family, carers, friends should be promoted.
An excellent overview is presented by covering the Emotions Studied in Context and the role of the Eating Environment [19].
Discussion
The diagnosis and treatment of cancer have devastating effects on the sufferer and are further compounded with loss of enjoyment of food resulting from smell and taste alteration on the ingestive process.
The problem of smell and taste alterations in chemotherapy arise from the complex nature of smell, taste and somatosensation (haptic sensation) which are modulated by both intrinsic (product specific attributes) and extrinsic (external attributes) contextual effects and further subjected to psychosocial influences.
The scope of the complex nature in the consumption of a meal (as distinct to snacking) is presented with the recommendation that the spectrum be considered rather than limited to individual factors.
Currently most intervention studies have focused on modification of the intrinsic properties of foods, however rarely considered are the diverse range of extrinsic factors influence the perception of foods and drinks; may other extrinsic factors can be represented in the classical tenets of gastronomy.
Psychosocial principles directed towards counselling, education and involvement of both patients and carers have displayed promising results through various strategies.
There is need for multidisciplinary approach involving meaningful active input from clinicians, from nurses, dieticians and nutritionists, oral health practitioners, gastronomers and gastrophysicists, occupational therapists and other allied health workers, in conjunction with sensory physiologists and psychologists along with appropriate restauranteurs. Institut Lyfe in Lyon is providing leadership in this field.
Biomedical gastronomy is proposed as a direction in which healing establishments can meld the principles of health care and healing to the classical tenets of gastronomy along with gastrophysics.
Gastrophysics, a term popularized by Charles Spence, a researcher in experimental psychology at Oxford University, considers:
- how all of the senses influence the perception of food and beverages such as the weight of cutlery or the color of a plate can alter the perceived flavor of food.
- psychophysics and cognition investigate how the brain processes sensory cues, expectations, and memories to determine the enjoyment of a meal.
In essence, gastrophysics explains that the "flavor" of food is created in the brain, not just on the tongue, and is heavily influenced by the environment.
Gastrophysics represents the scientific study of eating and drinking combining gastronomy with psychophysics providing an understand how all our senses, emotions, and surroundings shape flavor perception. It explores extrinsic factors, such as environment and ambience, table settings, lighting, and sound, to enhance dining experiences, improve health, and influence food choices.
Gastrophysics has practical applications in field and is used by chefs, marketers, and food designers to create more immersive dining experiences. It can also promote healthier eating by making healthier foods more appealing and has a potential use in healing environments as biomedical gastronomy.
As mentioned in a former paper, a need exists to have information and an understanding of the incidence and relationship, and specific impacts of smell and taste alterations currently encountered in chemotherapy. Of importance is data concerning the nature of olfactory changes including the classes of smells impacted, the influences of the classes of tastes impacted and the haptic changes in and around the mouth (stereognosis) and the impact of the various chemotherapy agents. This would enable better understanding and potential to prescribe appropriate interventions.
Many of the extrinsic factors are untested in the management of altered eating of chemotherapy patients, but given their values recognized in the literature and in the restaurant industry, they are worthy of investigation. Two decades ago, Stroebele et al. 2004 [23] suggested that the manipulation of various external factors such as social and physical surroundings, including the presence of other people and sound, temperature, smell, color, time and distraction affect food intake and food choice. These ambient factors as a whole or individually may be used therapeutically to alter food intake and that more attention needs to be paid to ambience in nutrition related research.
Testing these concepts would be easier in patients’ own homes, whereas in clinical situations they would require extensive changes in patient and clinical management and organizations. However, if malnutrition can be largely prevented and with patients requiring less hospital time the savings in the healthcare budget would be considerable. Above all, by enhancing the well-being and quality of life of patients and those closely associated would far outweigh changes necessary.
Constraining factors in a biomedical gastronomic approach are in the management of patients in acute phases of treatment and patients with advanced neurocognitive declines. In the former group treatment priorities over-ride this approach, and in the latter group special care related to hazard avoidance preclude many aspects. In these cases, special approaches are essential.
Conclusions
A promising area for study is that of gastrophysics and its involvement in biomedical gastronomy. Biomedical gastronomy requires the potential involvement of specialists yet requires a ‘jack-of-all-trades’ approach encompassing, nutrition, psychology, oral function and sensory connected between mouth and the brain.
The concepts proffered in this article, although directed toward cancer chemotherapy, have relevance in other instances in ageing in which sensory declines occur in olfaction and the somatosenses and complicated by various neurocognitive declines.
In this commentary, an holistic approach is proposed to consider the scope of sensory factors encompassing influences on eating behaviour with an emphasis on extrinsic factors which may in part compensate for loss of intrinsic properties and cues from food and beverages. The scope highlights a need for a multidisciplinary approach to be developed involving the clinicians nursing staff, nutritionists and dieticians, gastronomists, oral health practitioners, and other allied health workers.
In the acute phases of management, involvement in biomedical gastronomy is precluded by the clinical management imperatives. By introducing biomedical gastronomy early in rehabilitation, the patient is on the road to recovery with involvement in food skills, education and rituals.
Accomplishment of biomedical gastronomy would not be easy within the existing structures of hospital catering along with the current constraints of clinical needs, but should be encouraged to evolve within the concept of the healing space [25] “the environment cannot cause healing to occur but can facilitate engagement in behaviours and emotions that support healing; the environment can induce physical and emotional responses such as happiness, joy, and relaxation; and the (built) environment can enhance individual control and functionality—all of which are antecedents to healing”. This statement, with the omission of the word ‘built’ in the original statement, can be extended to the food experiences of patients with smell and taste alterations arising through chemotherapy and apply to many other patients. The cost savings involved would likely outweigh the cost of implementation and provide benefits in public health budgets.
By providing pride, purpose and recovered pleasure in ‘the table’, has the potential to enhance nutrient intake and reverse the ravages of malnutrition and combat malignant cachexia.
This commentary aims to evoke the consideration of multidisciplinary topics considered rarely owing to the specialist nature of patient care not only in cancer therapy but in cases where malnutrition is a risk factor.
References
2. Spence C, Piqueras-Fiszman B. The perfect meal: The multisensory science of food and dining. John Wiley & Sons; 2014.
3. Erickson N, Sulosaari V, Sullivan ES, Laviano A, van Ginkel-Res A, Remijnse W, et al. Nutrition Care in Cancer: An Overlooked Part of Patient-Centered Care. Semin Oncol Nurs. 2025 Feb;41(1):151799.
4. Woods SC, Begg DP. Regulation of the Motivation to Eat. Curr Top Behav Neurosci. 2016;27:15–34.
5. Spence C. Just how much of what we taste derives from the sense of smell?. Flavour. 2015 Nov 2;4(1):30.
6. Divert C, Laghmaoui R, Crema C, Issanchou S, Wymelbeke VV, Sulmont-Rossé C. Improving meal context in nursing homes. Impact of four strategies on food intake and meal pleasure. Appetite. 2015 Jan;84:139–47.
7. Cohen J, Wakefield CE, Laing DG. Smell and Taste Disorders Resulting from Cancer and Chemotherapy. Curr Pharm Des. 2016;22(15):2253–63.
8. Shepherd GM. Smell images and the flavour system in the human brain. Nature. 2006 Nov 16;444(7117):316–21.
9. Shepherd G. Neurogastronomy: how the brain creates flavor and why it matters. New York: Columbia University Press; 2012.
10. Zampini M, Spence C. The role of auditory cues in modulating the perceived crispness and staleness of potato chips. J. Sens. Stud. 2004 Oct;19(5):347–63.
11. Langhans W, Watts AG, Spector AC. The elusive cephalic phase insulin response: triggers, mechanisms, and functions. Physiol Rev. 2023 Apr 1;103(2):1423–85.
12. Santich B. The study of gastronomy: A catalyst for cultural understanding. Int J Humanit. 2007 Nov 20;5(6):53–8.
13. Brillat-Savarin JA. Physiologie du goût. Paris: Charpentier; 1865. p. 42.
14. Fischler C. Food habits, social change and the nature/culture dilemma. Soc. Sci. Inf. 1980 Dec;19(6):937–53.
15. Burges Watson DL, Lewis S, Campbell M, Bryant V, Storey ST, Deary V. Food play: A novel research methodology for visceral geographers and health researchers. Health Place. 2019 May;57:139–46.
16. Ben-Arye E, Keshet Y, Shahbar IM, Aharonson ML, Preis L, Agour O, et al. The kitchen as therapy: qualitative assessment of an integrative cuisine workshop for patients undergoing chemotherapy. Support Care Cancer. 2016 Apr;24(4):1487–95.
17. Croy I, Nordin S, Hummel T. Olfactory disorders and quality of life--an updated review. Chem Senses. 2014 Mar;39(3):185–94.
18. Croy I, Hummel T. Olfaction as a marker for depression. J Neurol. 2017 Apr;264(4):631–38.
19. Edwards JS, Hartwell HJ, Giboreau A. Emotions Studied in Context: The Role of the Eating Environment. In: Meiselman HA, (Ed.) Emotion Measurement. Woodhead Publishing; 2016 Jan 1. p. 377–403.
20. van’t Riet J, Sijtsema SJ, Dagevos H, De Bruijn GJ. The importance of habits in eating behaviour. An overview and recommendations for future research. Appetite. 2011 Dec 1;57(3):585–96.
21. Higgs S, Thomas J. Social influences on eating. Curr. Opin. Behav. Sci. 2016;9:1–6.
22. Hermans RC, Lichtwarck-Aschoff A, Bevelander KE, Herman CP, Larsen JK, Engels RC. Mimicry of food intake: the dynamic interplay between eating companions. PLoS One. 2012;7(2):e31027.
23. Stroebele N, De Castro JM. Effect of ambience on food intake and food choice. Nutrition. 2004 Sep 1;20(9):821–38.
24. Olsen TD, Kirkegaard PH, Fisker AM. Healing Architecture: how hospital food environments can help improve patient recovery - an integrative literary review. 2010.
25. DuBose J, MacAllister L, Hadi K, Sakallaris B. Exploring the Concept of Healing Spaces. HERD. 2018 Jan;11(1):43–56.
26. Reybrouck M, Podlipniak P, Welch D. Music and Noise: Same or Different? What Our Body Tells Us. Front Psychol. 2019 Jun 25;10:1153.
27. North AC. The effect of background music on the taste of wine. Br J Psychol. 2012 Aug;103(3):293–301.
28. Reinoso Carvalho F, Velasco C, van Ee R, Leboeuf Y, Spence C. Music Influences Hedonic and Taste Ratings in Beer. Front Psychol. 2016 May 6;7:636.
29. Reinoso-Carvalho F, Gunn LH, Horst ET, Spence C. Blending Emotions and Cross-Modality in Sonic Seasoning: Towards Greater Applicability in the Design of Multisensory Food Experiences. Foods. 2020 Dec 17;9(12):1876.
30. Spence C. Using Ambient Scent to Enhance Well-Being in the Multisensory Built Environment. Front Psychol. 2020 Nov 19;11:598859.
31. Michel C, Velasco C, Spence C. Cutlery matters: heavy cutlery enhances diners’ enjoyment of the food served in a realistic dining environment, Flavour. 4(1):26.
32. Spence C. Gastrophysics: a new scientific approach to eating. Viking: Penguin; 2017.
33. Ijpma I, Renken RJ, Ter Horst GJ, Reyners AK. Metallic taste in cancer patients treated with chemotherapy. Cancer Treat Rev. 2015 Feb;41(2):179–86.
34. Stewart PC, Goss E. Plate shape and colour interact to influence taste and quality judgments. Flavour. 2013 Oct 25;2(1):27.
35. Liu J, Petit E, Brit AC, Giboreau A. The impact of tablecloth on consumers’ food perception in real-life eating situation. Food Qual. Prefer. 2019 Jan 1;71:168–71.