Abstract
Approximately 35 million women worldwide have silicone breast implants. Like all medical devices, breast implants are not lifelong, and all will eventually need to be removed, with or without replacement. In 2019, the U.S. Food and Drug Administration (FDA) updated its guidance on breast implant surveillance to include HRUS screening for silent rupture. In-office high-resolution ultrasound (HRUS) is becoming increasingly common in plastic surgery practices. Local and regional training programs, along with numerous studies, support the sensitivity and specificity of HRUS in detecting breast implant complications. As a result, plastic surgeons are increasingly incorporating HRUS into their daily routines for the screening and diagnosis of patients with breast implants.
Keywords
Breast implant surveillance, High Resolution Ultrasound (HRUS), Breast Implant Associated Anaplastic Large Cell Lymphoma (BIA_ALCL), Lateral flow assay
Introduction
Approximately 35 million women worldwide currently have a breast implants, with an estimated 1.8 million women undergoing a breast implant procedure in 2023 [1,2]. Silicone implants, like other medical devices, have a lifespan and eventually all will need to be removed or replaced due to implant failure. Rupture of a silicone implant may be due to a small pin-point hole, or a larger visible tear with complete disruption of the silicone shell. Implant rupture rates vary between manufacturers and the generation of breast implant with increasing frequency as the implant ages. Most ruptures are clinically undetectable, and the Food and Drug Administration (FDA) refers to this as a “silent” rupture. The incidence of silent rupture has been reported to be as high as 8% [3]. In 2019, the FDA issued updated guidance on silicone breast implant surveillance. The current FDA recommendation is Magnetic Resonance Imaging (MRI) or High-Resolution Ultrasound (HRUR) at year five and every two-three years after to screen for silent rupture [4]. In-office HRUS is becoming a common practice among board certified plastic surgeons. The rapid advancement of handheld ultrasound technology, combined with expanded training of plastic surgeons in breast implant imaging, has substantially improved the ability of plastic surgeons to provide close follow-up for patients with breast implants.
Ultrasounds and Breast Implant Imaging
Ultrasounds are increasingly used in medical and surgical sub-specialties. Systems transmit a focused sound wave to a specific depth and then interpret the returning echoes. Diagnostic ultrasound probes range between 1–12 megahertz (cycles per second) [5]. Most breast implants are located less than 5–6 cm below the skin and require an ultrasound setting with a range from 7–12 megahertz and a linear array. Curriculum covering ultrasound theory and hands-on interpretation of common breast implant complications is now offered in plastic surgery residency programs and scientific meetings throughout the world [6,7].
Breast Implant Surveillance versus Standard Breast Imaging
The role of HRUS in a plastic surgery practice is best described as breast implant surveillance and not breast cancer screening. Studies have demonstrated high sensitivity and specificity of ultrasound to detect implant ruptures and to diagnose other local complications associated with breast implants [8] (Figures 1 and 2). In-office HRUS does not replace the need for women to undergo routine cancer screening by mammography or ultrasound. Patients are encouraged to follow the recommendations of the American College of Radiology for women ages forty and continuing past 74 without an upper age limit [9]. In the United States, silicone breast implants are available to women at age 22, yet the first screening mammogram for breast cancer does not begin until age 40. This younger demographic often has little to no implant follow-up [10]. Another group of women who are not routinely followed for implant rupture are patients who have undergone implant-based breast reconstruction. They are generally advised that no further breast imaging is required post-mastectomy. HRUS offers many advantages for patients over MRI; it is affordable, eliminates claustrophobic concerns, there are no restrictions for metal ports or hardware, and most importantly, makes patients more likely to comply with recommended implant screening.
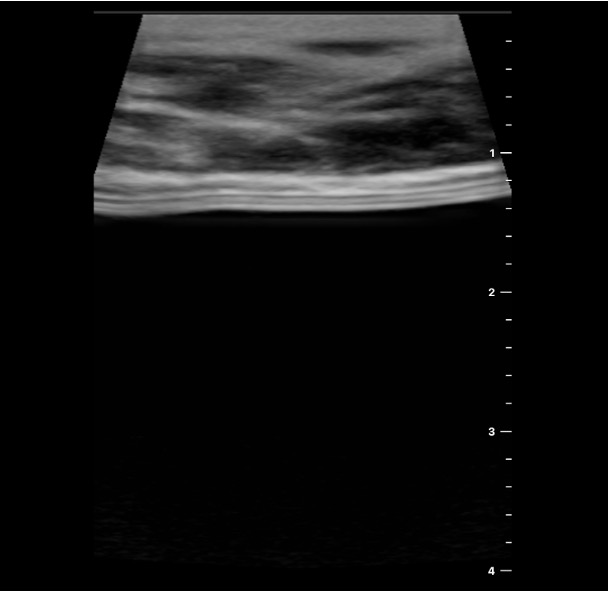
Figure 1. Intact implant.

Figure 2. Ruptured implant.
The Learning Curve
It is important that the ultrasound findings be accurately interpreted to make a proper diagnosis, and the surgeon is able to demonstrate and explain the findings to the patient. Studies have demonstrated a rapid learning curve for plastic surgeons using HRUS to examine breast implants. In a recent study, Ferenz, et al. evaluated the learning curve by reviewing 340 sequential readings in two breast augmentation practices shortly after purchasing their first ultrasound. The pre-operative readings were checked for accuracy by comparing to the subsequent operative findings. It was found that the surgeons were able to reach over 97% sensitivity and 100% specificity for diagnosing breast implant rupture after only 60 HRUS readings (30 patients). There was also a continued improvement in overall accuracy of HRUS over time (100%), demonstrating better sensitivity and specificity than the standard reported by board certified radiologists. Findings such as a new mass or suspicious finding within the breast are referred to a radiologist for further breast imaging [11].
Clinical Indications
Prior to the development of the two US breast implant registries, The American Registry for Breast Implant Surveillance (ARISE) and the National Breast Implant Registry (NBIR), patients frequently were unaware of their implant information or procedural data [12,13]. In-office HRUS can provide valuable information about a patient’s implants, including the surface of the breast implant, smooth or textured, and the surgical pocket location, above or beneath the pectoralis major muscle (Figures 3 and 4). HRUS is valuable in the evaluation of various implant complications. Deep folds in older generation or underfilled silicone implants can be mistaken for rupture on mammogram. Gentle pressure applied to the implant during the ultrasound exam can distinguish folds from rupture (Figures 5 and 6).
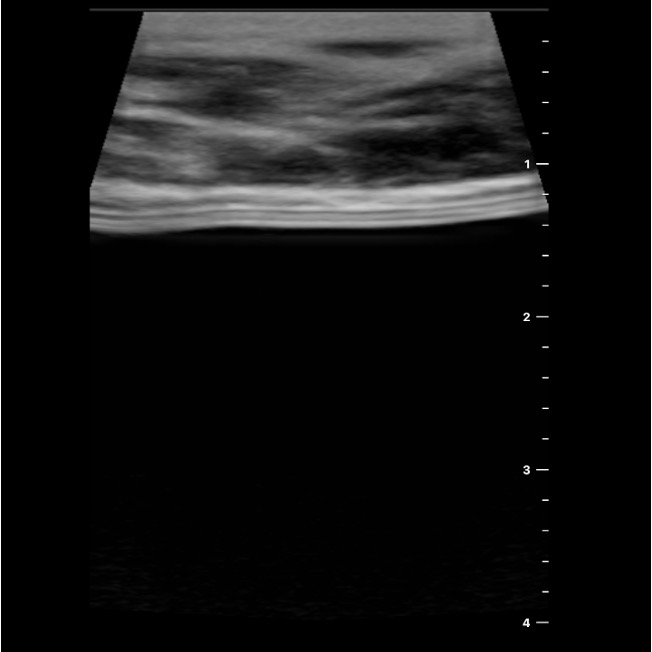
Figure 3. Smooth implant subpectoral (below the muscle).
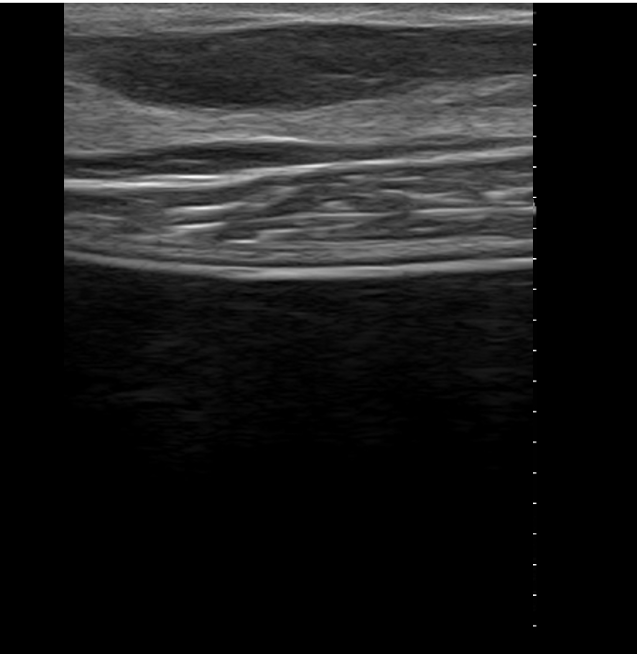
Figure 4. Textured implant subglandular.
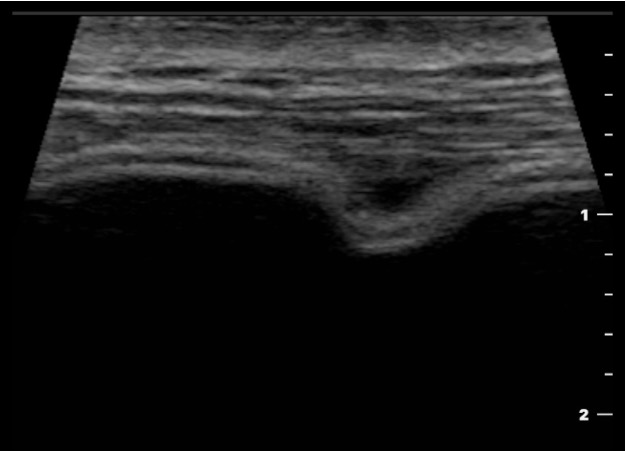
Figure 5. Fold in intact implant.
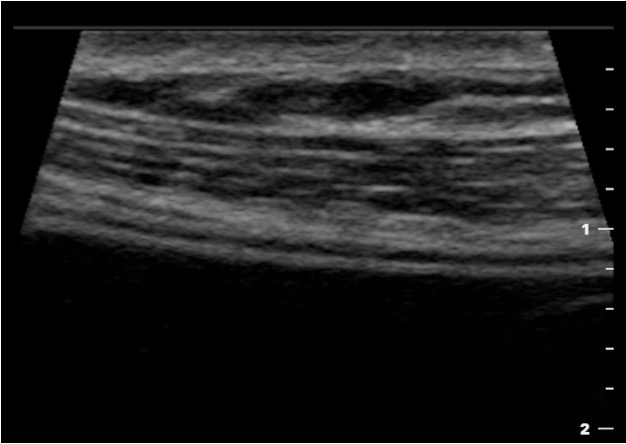
Figure 6. Gentle pressure flattens fold.
Another indication for in-office HRUS is the evaluation of the swollen breast. Seromas can be distinguished from hematomas in the early post operative period. Seromas can appear as anechoic periprosthetic fluid collections while hematomas are more heterogeneous with debris within the fluid (Figure 7). Aspiration of bloody versus clear fluid distinguishes between the two. Fluid collections around an implant should be sent for cytology, when clinically indicated. A late seroma is defined as occurring more than one year after implantation. All late seromas require a diagnostic work-up to distinguish between a benign or potentially malignant peri-prosthetic fluid collection. Breast Implant Associated Anaplastic Large Cell Lymphoma (BIA-ALCL) is a rare T-cell lymphoma associated with certain textured breast implants. Early detection allows surgical planning and treatment before local invasion or distant metastasis occurs. More advanced disease requires radiation, chemotherapy and/or immunotherapy. Rapid evaluation of seromas with in-office ultrasound expedites fluid aspiration and diagnostic cytology, immunohistochemistry, and flow cytometry [14]. Currently a minimum or 25-50 cc of aspirated fluid is required for the diagnosis of BIA-ALCL. Point of care research is currently underway to develop a lateral flow assay (LFA) to detect lymphoma biomarkers in seromas with as little as 10cc of aspirate within 20 minutes. In a recent study by Xu, et al. Carbonic Anhydrase IX (CA IX) was found to be significantly increased in malignant seromas compared to benign seromas [15]. A second study established CD30 and IL-10 as paired diagnostic biomarkers for BIA-ALCL [16]. Proficiency in HRUS and the future development of LFA to screen seromas may dramatically speed the diagnosis of BIA-ALCL.
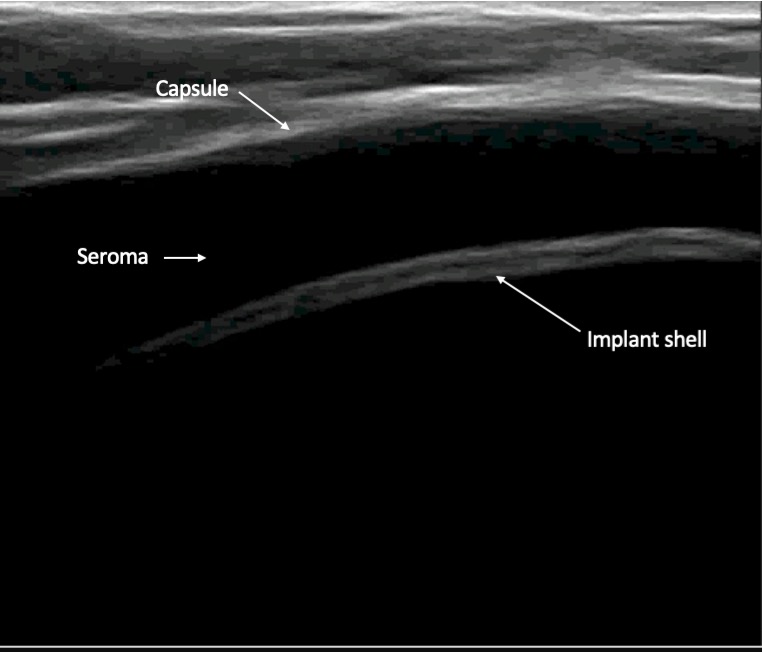
Figure 7. Diagnosis of hematoma vs Seroma.
Conclusion
As plastic surgeons become increasingly proficient in performing HRUS, it has become an indispensable component of patient follow-up. Patients seeking revision procedures or presenting with complications often lack surgical or implant records. Information on implant surface, fill, and pocket location can all be determined with in-office HRUS and provide the surgeon with a more accurate diagnosis and aid in surgical planning. The rapid evaluation of a swollen breast by HRUS and fluid aspiration is an essential part of a diagnostic work-up. Perhaps the most important benefit of breast implant surveillance with HRUS is the peace of mind provided to all implant patients. HRUS is safe, with high sensitivity and specificity, and can assure asymptomatic patients that there are no problems with their implants.
Conflicts of Interest/Disclosures
Dr Glicksman is the medical director for Motiva US Breast Implant Clinical Trial (Establishment Labs, Alajuela, Costa Rica) and is the Principal US investigator for Becton Dickinson GalaFlex STANCE Study.
Dr McGuire is a clinical investigator and consultant for Establishment Labs (Alejuela, Costa Rica).
Sarah Ferenz, MD is a plastic surgery resident at University of South Florida and has no disclosures.
References
2. Sieber DA, Adams WP Jr. What's Your Micromort? A Patient-Oriented Analysis of Breast Implant-Associated Anaplastic Large Cell Lymphoma (BIA-ALCL). Aesthet Surg J. 2017 Sep 1;37(8):887–91.
3. Hedén P, Nava MB, van Tetering JP, Magalon G, Fourie le R, Brenner RJ, Lindsey LE, Murphy DK, Walker PS. Prevalence of rupture in inamed silicone breast implants. Plast Reconstr Surg. 2006 Aug;118(2):303–8; discussion 309–12.
4. U.S. Food and Drug Administration. Breast implants: certain labeling recommendations to improve patient communication. Guidance for industry and Food and Drug Administration staff. Silver Spring (MD): U.S. Food and Drug Administration; 2020 Sep 29 [cited 2025 Dec 18]. Available from: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/breast-implants-certain-labeling-recommendations-improve-patient-communication
5. Clarius. Clarius AI [Internet]. Vancouver (BC): Clarius Mobile Health; 2025 [cited 2025 Dec 15]. Available from: https://clarius.com/technology/clarius-ai/
6. Schafer ME. Fundamentals of High-Resolution Ultrasound in Breast Implant Screening for Plastic Surgeons. Clin Plast Surg. 2021 Jan; 48(1):59–69.
7. Bengtson BP. Instructional Course: Officed-Based High-Resolution Ultrasound for the Plastic Surgeon. Clin Plast Surg. 2021 Jan; 48(1): xiii–xxix.
8. Glener AD, Sergesketter AR, Adams WP Jr. Outcomes of In-Office, High Resolution Ultrasound Silicone Breast Implant Surveillance by Plastic Surgeons. Aesthet Surg J. 2024 Dec 12; 45(1):48–55.
9. US Preventive Services Task Force; Nicholson WK, Silverstein M, Wong JB, Barry MJ, Chelmow D, Coker TR, et al. Screening for Breast Cancer: US Preventive Services Task Force Recommendation Statement. JAMA. 2024 Jun 11; 331(22):1918–30.
10. Monticciolo DL, Malak SF, Friedewald SM, Eby PR, Newell MS, Moy L, et al. Breast Cancer Screening Recommendations Inclusive of All Women at Average Risk: Update from the ACR and Society of Breast Imaging. J Am Coll Radiol. 2021 Sep; 18(9):1280–8.
11. Ferenz S, McGuire P, Glicksman C. The Efficacy and Associated Learning Curve of Office-Based High-Resolution Ultrasound to Detect Shell Failure in Breast Implants. Aesthet Surg J. 2023 May 15; 43(6):657–61.
12. American Registry for Breast Implant Surveillance and Evaluation (ARISE). ARISE annual report. Garden Grove (CA): ARISE Registry; 2025. Available from: https://aestheticfoundation.sfo3.cdn.digitaloceanspaces.com/docs/arise-annual-report.pdf
13. National Breast Implant Registry (NBIR) Annual Report 2023. Arlington (VA): The Plastic Surgery Foundation; 2023. Accessed on December 22, 2025. Available from: https://www.thepsf.org/documents/Research/Registries/NBIR/NBIR-Annual-Report-2023.pdf
14. Keane GC, Keane AM, Diederich R, Kennard K, Duncavage EJ, Myckatyn TM. The evaluation of the delayed swollen breast in patients with a history of breast implants. Front Oncol. 2023 Jul 5;13:1174173.
15. Xu P, Kourentzi K, Willson R, Hu H, Deva A, Campbell C, et al. Lateral Flow Assay to Detect Carbonic Anhydrase IX in Seromas of Breast Implant-Associated Anaplastic Large Cell Lymphoma. Cancers (Basel). 2025 Jul 21; 17(14):2405.
16. Xu P, Brosamer K, Kourentzi K, Willson R, Hu H, Deva A, et al. Multiplex Lateral Flow Assay Combining CD30 and IL-10 for the Detection of BIA-ALCL. Aesthet Surg J. 2025 Aug 18;45(9):893–8.