Abstract
Background and Aims: Chronic kidney disease (CKD) constitutes a significant global health burden due to its association with kidney failure, cardiovascular morbidity, and premature mortality. Despite incremental advancements in nephrology, technological innovation has progressed more slowly than in other clinical fields. Information and communication technology (ICT) offers the potential to address inefficiencies in hemodialysis (HD) care through enhanced monitoring, communication, and data management. This study examines current ICT interventions in HD, evaluates their effectiveness, and identifies limitations and opportunities for further development.
Results: Findings from the systematic review indicate that ICT integration including telehealth, remote surveillance systems, electronic documentation platforms, and mobile-based self-management tools provides measurable benefits in HD care. These interventions are associated with improved clinical outcomes, optimized treatment delivery, greater patient satisfaction, and reduced healthcare expenditure. In the context of home hemodialysis (HHD), ICT enhances patient autonomy, fosters continuous connectivity with healthcare teams, and supports adherence. The incorporation of ICT aligns with the principles of 4P medicine by enabling predictive analytics, precision dosing, and preventive risk monitoring, and personalized treatment strategies.
Conclusion: ICT is poised to play an increasingly central role in the evolution of HD and HHD. While current evidence underscores its value, significant gaps remain in interoperability, standardization, and the integration of real-time clinical decision support. Continued research and technological advancement are essential to fully realize the transformative potential of ICT in nephrology.
Highlights:
• HD Therapy in which ICT intervention is present were reviewed.
• The factors that contribute to enhancing the impact of ICT solutions on nephrology practice were identified and analyzed.
• Different types of ICT interventions in nephrology practices were analyzed and verified.
• Research gaps and limitations regarding ICT interventions on nephrology were identified and listed.
Aim: The aim of this study was to review and synthesize the available literature on the role of ICT in HD in nephrology units in global healthcare settings. The systematic review was conducted to examine the content and results of publications on the use of information and communication technologies to improve the health care of HD patients, available for healthcare professionals (HCPs) and patients.
Keywords
Information and Communication Technology intervention in hemodialysis, Systematic review, Home hemodialysis, Remote Patient Monitoring / management, End-stage renal disease, Chronic kidney disease
Abbreviations
ICT: Information and Communication Technology; CKD: Chronic Kidney Disease; DKD: Diabetic Kidney Disease; eGFR: Estimated Glomerular Filtration Rate; uACR: Urine Albumin-Creatinine Ratio; ESRD: End-Stage Renal Disease; KDIGO: Kidney Disease: Improving Global Outcomes; PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses; RRT: Renal Replacement Therapy; RPM: Remote Patient Monitoring; HD: Hemodialysis; PD: Peritoneal Dialysis; HHD: Home Hemodialysis; RTS: Renal Replacement Therapy; TX: Transplantation; RMT: Remote Management Therapy; RTS: Renal Therapy Services; EKHA: European Kidney Health Alliance; ICHD: In-Center Hemodialysis; THC: Tele-Homecare; PGHD: Patient-Generated Health Data; AAKP: American Association of Kidney Patients (AAKP); PAHO: Pan American Health Organization; WHO: World Health Organization; PC: Personal Computer; PGHD: Patient-Generated Health Data; HCP: Health Care Professional
Introduction
Worldwide, there are two million people with CKD. According to EKHA (htts://ekha.eu;2024 [accessed on Oct 22, 2024]), between 2020 and 2030, kidney patients will witness the accelerating evolution away from the tired status quo of bricks-and-mortar dialysis as we know it and toward a future defined by patient choice; targeted therapies that inhibit kidney disease and prevent kidney failure [1]; greater access to donated organs and new devices—including artificial wearable and implantable kidneys.
Kidneys are responsible for the processes of filtration of toxic waste products for maintaining acid–base (pH) and electrolytes balance in the human body. When a patient reaches the ERSD and is not (yet) eligible for renal transplantation, is dependent on others RRT treatment modalities, such as peritoneal dialysis (PD) or HD [2]. HD use to be performed intermittently for about 4 hours 3 days a week.
The development of ICT has been constant in recent years, at various levels and in various areas of healthcare. In nephrology and, particularly, in RRT, this evolution has also been seen. ICT has assumed a predominant role in the different levels of health management [3], characterized by their ability to aggregate, organize, store data, and make it available immediately, with lower cost and greater efficiency for clinical decision-making.
Nowadays ICT systems are a necessary and integral part of HD therapy, supporting monitoring patients and collecting automatic registration of treatment data given the scope of the CKD population, the complexity of CKD care, and the limited number of nephrologists.
The efficient use of ICT in Nephology requires HCP capacitation and patient training to develop a variety of self-management skills to effectively deliver and manage their disease at home [4]. ICT interventions may provide the HCP with tools to better assist the patients and the patients with accessible information to develop the skills and knowledge they require to manage their treatment. This review aims to identify and evaluate ICT interventions in supporting clinicians and patients of nephrology units.
As CKD is an extremely complex disease, multidisciplinary care is needed to provide complete and continuous care. The use of ICT in nephrology aims to improve the cooperation between several Health Care Professionals and the patient self-management intervention to improve the care and facilitate an individual’s ability to make lifestyle changes as needed. The effectiveness of these interventions on patients with kidney disease is limited by the integration of these new tools into the common procedure [5] of the nephrology units. In this study, we applied a systematic review to investigate whether the ICT intervention improves HD healthcare in the nephology units.
The ultimate goal of ICT intervention would be to reduce adverse events (i.e., hospitalization), and improve survival, and patient-reported outcomes such as treatment satisfaction and quality of life while reducing healthcare resources and costs [6].
The reports concerning peripheral HD centers which were connected to a reference hospital by videoconferencing give very good expectations. Subsequently, ICT intervention was used in home dialysis in some countries with encouraging results. However, despite these reports, long-term experience is scarce [6,7].
HHD use, supported by ICT can improve patients' management and quality of life with chronic disease. In addition, using ICT [7] to educate patients will be important in a connected world while trying to decrease face-to-face interactions.
Research in context and evidence before this study
CKD, especially end-stage renal disease (ESRD), represents a major public health problem in developed and developing countries.
To prepare for our review we looked for several reviews concerning specific types of ICT intervention in HD.
The current evidence is mainly based on disparate case reports and small observational studies [8]. In this study, we aimed to ascertain the studies exploring the use of ICT in the context of HD therapy.
The main purpose of information and communication technologies is to increase efficiency and to achieve the quality of healthcare, its modernization, and improvement.
Inclusion and Exclusion Criteria
Objective
In the Nephrology field, ICT was originally utilized for Remote Patient Monitoring (RPM), the patients in a single type of RRT - Peritoneal dialysis. This Systematic Review aims to determine how ICT can contribute to improving the Healthcare for HD Patients. The main purpose of ICT is to increase efficiency and to achieve the quality of healthcare, its modernization, and improvement.
Proposals or key questions
- Is ICT effective in improving care for patients in HD?
- How can ICT support the Healthcare professional treating patients in HD?
- Can the use of ICT contribute to improving the health care of patients in HD?
- Can the use of ICT contribute to improving the quality of life of HD patients?
- Can the use of ICT influence early detection or even contribute to avoiding starting HD?
Study Selection
Inclusion criteria
- To be included the objective of the article should include the evaluation of HD supported by ICT intervention.
- The article should refer to ICT tools used by healthcare professionals and/or patients to support or manage HD treatment.
Exclusion criteria
- All articles that refer to HD but do not relate it to any kind of ICT.
- All articles that refer to ICT but do not use it to support or manage patients in HD type of “literature” review about ICT intervention in HD.
Methods
Search strategy
We decided to perform an exhaustive search in several databases such as Web of Science, PubMed, Scopus, ScienceDirect, SciELO, and Cochrane Library to find papers concerning ICT applied to HD Therapy. To strengthen the research, we contacted numerous experts in Nephrology, from societies and organizations of Nephrology, and EKHA (European Kidney Health Alliance). We also participated in several scientific events on the subject of Nephrology, around the world.
This review search was conducted by searching for studies published from 2005 to May 2022 in several electronic databases as mentioned above. Randomized, Non-randomized, Qualitative and Quantitative controlled trials describing an improved intervention using some kind of ICT (e.g., Home based HD) RPM; Patient Portal, wearable devices, Nanotechnology; Tele-nephrology (Telemedicine applied to Nephrology); Home Care Treatment; mHealth, Self-Management, Artificial Intelligence in patients with some stage of kidney disease were included. Studies that assessed patients and/or HCPs using ICT (e.g., smartphone applications, Software applications, internet, Tablet & PC based) and/or studies that involve HD therapy were eligible.
The primary search term used was ‘Information and Communication Technology in HD Therapy”.
In addition, to refine and determine the appropriate search terms, the study employed the ICT and HD types above, specifically considering the several ICT interventions that were relevant to this research field. The reference list of the identified papers was also checked.
The refined search terms were performed by combining ICT and HD. Thus, the specific search terms were as follows:
• ‘*Dialysis’ AND ‘Information and Communication Technology intervention’
• ‘HD’ AND ‘ RPM’
• ‘Remote Patient*’ AND ‘*Dialysis’
• ‘Tele*’ AND ‘HD’
• ‘Hemodialysis’ AND ‘ICT’
• ‘HD’ AND ‘ICT’
• ‘Renal*’ AND ‘ICT’
• ‘HHD’ AND ‘ICT’
• ‘*Dialysis’ AND ‘ICT’
The publications collected by utilizing the above search terms in the databases referred to above were not all entirely within the scope of this study.
In this systematic review, the outcome measures were deliberately kept broad to include all potential outcomes of ICT intervention in HD therapy described in the literature. The review included qualitative studies, quantitative studies, including observational, quasi-experimental, and mixed-method study designs, as well as grey literature. Once duplicates were removed, the titles and abstracts were screened and, after that, full-text articles were assessed to establish eligibility for inclusion. Finally, verification was performed to avoid discrepancies.
Therefore, the publications were filtered several times, independently, by two reviewers who evaluated study quality and extracted characteristics, aims, outcomes, limitations, and among patients under HD within the intervention of ICT for each trial. Reference lists from relevant review articles and reviews were also searched. Studies were first screened according to title and abstract, and the full texts of any study considered relevant according to the selection criteria were assessed for eligibility by both reviewers (AML and ARP). Disagreements between the reviewers concerning decisions to include or exclude studies were resolved by consensus, and if necessary, consultation with a third reviewer (JJSO).
Results
The search strategy yielded 2,774 records (Figure 1). After removing 248 duplicates, 129 removed for other reasons, such as full version not available, not an original research article, or considered as secondary sources, and excluding 2,397 articles in the title and abstract screening, we assessed 49 full-text articles for eligibility, including 8 records identified from searching the reference lists of included articles. Forty-two articles did not meet the inclusion criteria, which led to 15 articles being included in the systematic review (Supplementary Table 1).
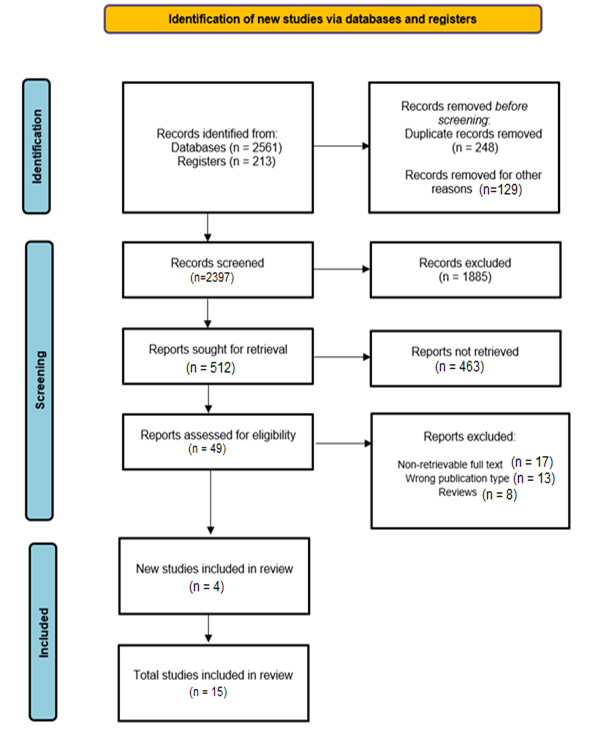
Figure 1. Flow chart of search and study selection process.
The main problems and burdens on the way to the implementation of ICT in HD treatment have been analyzed and compiled in the column of Limitations and Future Research in Supplementary Table 1.
Fifteen studies met the inclusion criteria involving, comprising a total of 2,028 patients at any type of HD treatment. The number of HCPs involved was only mentioned in a few studies [6,14].
Of those studies, some were quantitative, some used qualitative methods, and others adopted mixed methods.
As shown in Figure 2 most of the research originated in USA (5) and Australia (3) followed by Italia (2). The rest of the countries are the Netherlands, Brazil, Australia, Japan, South Korea, United Kingdom, and Canada with one publication each.

Figure 2. The geographic distribution of publications around the world. Notice that some publications are shared by more than one country.
Figure 3 shows that in some studies, more than one ICT Intervention is combined to improve HD management. We found “Telehealth” in 4 studies; Remote Patient Management present in 3 studies; Home Dialysis and PC/Tablet/Mobil Phone applications was found in 3 studies as well. Web or Patient Portal, Telemedicine, Remote Management Therapy Tele-homecare, and Artificial Intelligence in one study each. The objective of ICT intervention in all these studies was to improve healthcare for HD patients.
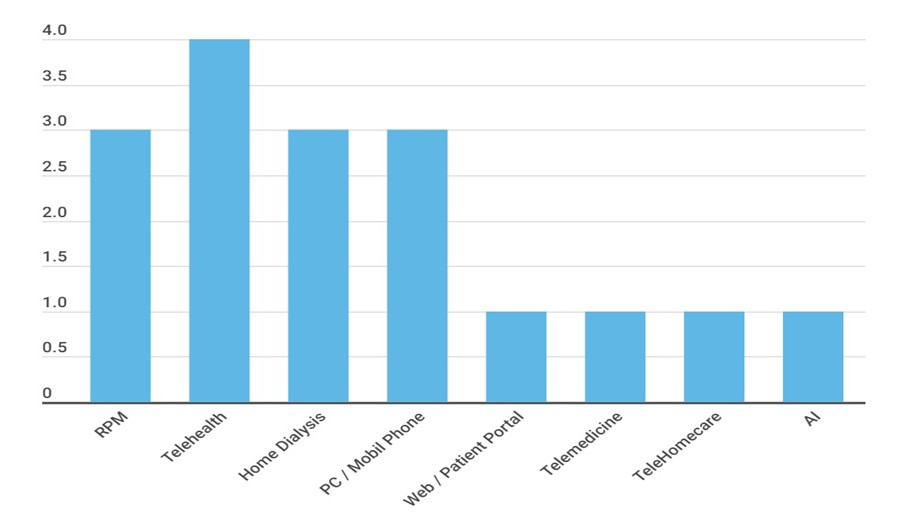
Figure 3. The distribution of ICTs used in the included studies.
Most Platforms are better organized and geared to support patients in peritoneal Dialysis at Home and patients towards in-center hemodialysis (ICHD), but multiple hurdles exist in educating and training a patient to perform HHD. We describe in the last column of Supplementary Table 1 the limitations and future research to tackle these challenges and adopt strategies to overcome some of these limitations and expand home dialysis.
The available results from included studies suggest that, in general, ICT can influence positively the healthcare of patients with kidney disease [9] (e.g. improve access to healthcare services [10], enhance the quality of life [11], empower the individual to follow a healthy lifestyle [12], significantly reduce the rate of readmissions, decrease costs, and so forth [13]).
Findings and types of outcomes
ICT intervention types included in our review were: RPM, Telehealth, mHealth, Home Dialysis, Telemedicine, Web/Patient Portal, Tele-homecare, Self-management. All aimed to highlight the effects of using ICT tools to improve HD therapy modalities.
Overall, the evidence suggests that ICT has the potential to bring several improvements, as indicated in the Findings, Outcomes, and Results column of Supplementary Table 1.
Figure 4 shows the evolution of publications from 2005 to 2022. The year 2020, with 4 publications, was the most productive followed by 2019 with 3; however, articles on this topic are still scarce.
Supplementary Table 2 shows the number of studies and the most relevant outcomes considering the type of ICT intervention.
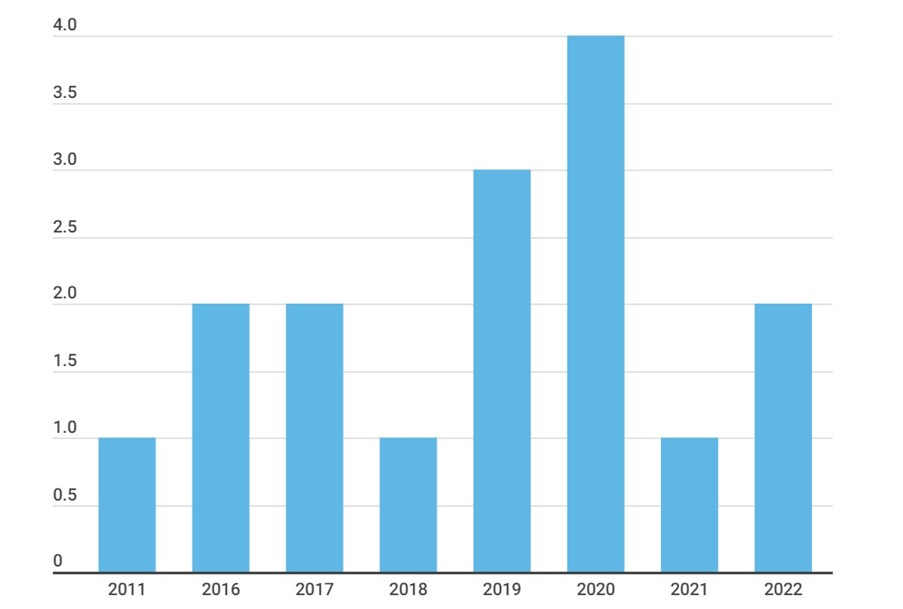
Figure 4. Number of publications per year from 2005 to 2022.
ICT intervention in HD therapy
Many types of ICT tools were found in the included studies, such as Remote Patient Management, Telehealth, mHealth, Home Dialysis, Telemedicine, Patient/web Portal, Tele-Homecare, Self-Management, Artificial Intelligence, and Remote Management Therapy. Some studies use a mix of two or more kinds of ICT looking for a better outcome [14] or to cover more needs.
The main propose of this review is to identify and summarize the published empirical evidence on the effects of ICT [15] tools on HD patients care. The insight gained is discussed in terms of how ICT interventions can optimize nephrology care and identify areas for future research.
The most common ICT tools involved in HD therapy
The included studies reported a wide range of ICT interventions associated with kidney disease. Some studies focused on specific ICT interventions and others use mixed ICT inventions in order to achieve a common goal: improving healthcare outcomes in Nephrology.
Nephrology adopted various types of ICT that span from simple charting to more advanced decision support and integration with medical technology.
Remote patient management
RPM is a subcategory associated with homecare telehealth that enables patients to use PC, tablet or mobile-related ICTs and technology to gather patient-generated health data (PGHD) and make it available to healthcare professionals. Common physiological data that can be collected with RPM programs include vital signs, weight, blood pressure, and heart rate. Once collected, patient data is available to a physician’s office through the use of a telehealth computer system or software application that can be installed on a computer, smartphone, or tablet.
RPM is frequently used to assist healthcare professionals and their patients who require chronic or acute care. By connecting high-risk patients with remote monitoring, it can notify healthcare organizations of potential health issues or keep track of patient data between visits [1,2,4,5,11].
More specifically, non-invasive technologies are now being commonly integrated into disease management strategies to provide additional information about patients, with the goal of improving healthcare decision-making.
Telehealth and telemedicine (Tele-nephrology)
Telehealth is defined as the use of electronic Information and Telecommunication Technologies to support long-distance clinical health care, health-related instruction or training of patients and health professionals, public health and administration. Technologies include video conferencing, store-and-forward imaging, streaming media, and terrestrial and wireless communications.
Telehealth is different from telemedicine, given that the first refers to a broader scope of remote healthcare services and the latter. Also, telehealth may include remote non-clinical services, such as provider training, administrative meetings, and continuing medical education, in addition to clinical services.
Telemedicine encompasses the use of telecommunications technologies and systems to administer healthcare to patients who are geographically separated from providers. We identified studies concerning Telehealth and Telemedicine [1,4,6,13].
mHealth
mHealth or mobile health refers to healthcare applications and programs, which patients use on their smartphones, tablets, or laptops. These applications allow patients to track health measurements, set medication and appointment reminders, and share information with clinicians. mHealth (or m-health) is short for mobile health, the practice of medicine and health care over mobile devices, tablets, PDAs, and computers.
mHealth focuses on obtaining information immediately to diagnose illnesses, track diseases, and provide timely information to the public in underserved countries. Mobile health is especially important in remote areas where doctors and nurses may not be present to provide treatment.
We identified some studies concerning mHealth [4,7–9].
Home Dialysis (Home Hemodialysis)
Home dialysis means dialysis performed at home by an ESRD patient or trained caregiver who has completed an appropriate course of training.
Home dialysis, including home hemodialysis (HD) and peritoneal dialysis (PD), in many papers, is associated with increased patient autonomy and treatment satisfaction.
We identified several studies concerning home dialysis [7,11–15].
Patient/web portal
A patient portal or web Portal is an internet-based platform that allows the patient to view medical records and connect with the healthcare professional. Patient portals can help the patient access medical records, schedule appointments, communicate with the healthcare professional, and pay medical services.
A patient portal or web Portal is typically a secure online website set up by a health care system, hospital, or clinic that gives patients convenient, 24-hour access to personal health information from anywhere with an Internet connection.
We identified the following study concerning the patient portal or web Portal [4].
Tele-HomeCare
Tele-homecare (THC) is a subfield within telehealth. It involves the delivery of healthcare services to patients at home through the use of telecommunications technologies, which enable the interaction of voice, video, and health-related data. Care management is performed from an external site by a healthcare professional. It is often interchanged with remote patient monitoring; however, Tele-HomeCare is not strictly patient monitoring because it incorporates a range of health care delivery through education, emotional and social support, information dissemination, and self-care help and suggestions.
Artificial Intelligence
Artificial intelligence (AI) healthcare is the use of machine learning, natural language processing, deep learning, and other AI-enabled tools to assist and, ideally, improve the patient experience, including diagnosis, treatment, and outcomes.
For clinical outcomes, AI analytics provides a faster, more in-depth examination of information without the risk of human error. In turn, physicians and surgeons can leverage these results into better treatment options that can translate to improved outcomes.
During the COVID-19 pandemic, for example, AI could be used to analyze new variants and create new, effective treatments faster than human-based research and assessment. AI also helps medical organizations stay in compliance with enhanced security and safety. These inputs can be used to determine high-risk patients and create actionable outcomes.
The result of ICT intervention on the HD therapy performance
In this section, we analyze the selected publications, listing the effects of ICT interventions in HD. Moreover, after a detailed investigation of the literature, we found the following results that deserve to be highlighted:
Outcome improvements were found in several studies (Supplementary Table 1) affecting important treatment issues such as adherence to treatments, therapy confidence, quality of life, patient autonomy and education.
An increase in patient satisfaction and acceptance appears as the outcome in the following studies [1,6,15] in which telemedicine enabled increasing the nephrologist’s coverage area and was positive mainly because it increased patient confidence and sense of care during HHD, reduces patient anxiety and increases confidence in the management of their chronic disease condition.
Michel Rosner et al. (2019) [1] mentioned that costs (economic and environment) associated with patient travel were alleviated using RPM or Telemedicine. Some studies found that healthcare costs decreased when using RPM tools for APD [4,5] or mHealth for supporting CKD in general.
RPM can improve outcomes and confidence in HD therapy and is a useful tool to increase Satisfaction and confidence in home dialysis [6].
In some studies authors detected that RPM improves adherence to follow-up and reduces healthcare utilization and in-presence visits for emergencies. Telehealth emphasizes its role in reducing hospital visits. Post-discharge nurse-led telephone support is helpful for some aspects of quality of life and reducing readmission and clinic visits of patients in home dialysis programs.
The ecological advantages are debated but are likely to be relevant especially if patients live far from dialysis unit [14].
This study also suggests the need for additional HCP training and support to help ensure that mobile health communication can lead to significant improvements in patient experience with home dialysis care. Also found that Tele-Nephrology may afford potential opportunities to reduce the cost of healthcare in patients with multiple renal conditions.
Discussion
This systematic review summarizes the literature on ICT intervention in HD therapy. Results Section show that current studies in this field of research demonstrate a limited focus on home hemodialysis. In addition, most studies also had a significant preference towards hemodialysis therapies supported by RPM, telehealth, home dialysis, and PC and cell phone technologies, and healthcare personnel are not aware of how ICT can promote significant cost savings and quality of life for patients.
The results show that further studies focusing on the long-term use, acceptance and outcomes of PROM are needed in the future. In addition, data mining tools should be developed to allow the user to extract reports or queries with specific information. Therefore, prevention support and management tools push nephrologists to actively encourage the development of ICT tools focused on CKD prevention.
In the future, we can say: a study to investigate the efficacy of electronic consultation compared to face-to-face in the case of CKD.
Beyond that, sustaining and disseminating the telecare application that will be useful in guiding the development, implementation, and evaluation of future virtual care applications aimed at improving quality of care, outcomes, time savings, and patient experiences [4].
The increasing use of ICT is leading to the need for healthcare professionals and patients to incorporate technological competence into HHD practice. This results in improved quality of life and significant cost savings, as well as being beneficial to the environment [12].
Our review of the studies in the previous section finds that all research, related to ICT intervention in HD therapy, has arrived at an optimal solution to improve healthcare by relying on ICT-based tools adapted to support HD therapies. This type of research also helps to realize that ICT intervention in HD can contribute to minimizing human errors, improve patient safety, report generation, improve access to test results, improve communications between all clinical staff and patients, etc., increase and improve access to HD, so forth.
Our review of the studies in the previous section finds that all research, related to the ICT intervention in HD therapy, has reached an optimal solution to improve healthcare relying on ICT-based tools adapted to support HD Therapies. This type of research also helps to realize that ICT intervention in HD can contribute to minimizing human error, improve patient safety, report generation, improve the access to tests results, improve communications between all clinical staff and patients and so forth, increase and enhance the access to the HHD.
Some reported evidence is limited due to the short duration of the studies and the small number of participants because of restricted access to personal data and mandatory ethical approval. However, the duration of follow-up and the number of participating subjects are very small in these types of studies; in other words, the evaluation process for these types of studies is complex and time-consuming. This may be the main reason why investigators prefer to conduct studies in subjects with easy-to-evaluate CKD.
We focused on the main characteristics of the included studies (Supplementary Table 1) taking into account, objective, lead author, countries and year of publication, technologies used in ICT tools, sample size and duration, when reported, findings, results, and finally, gaps or limitations and future research.
Future design changes and larger scale studies are being developed. Researchers have also applied remote monitoring to HHD with encouraging but limited results [7]. In addition, future research should focus on identifying and addressing barriers to patient participation in portal use [10].
Currently, many dialysis units are still unable to offer home dialysis, so the implementation and widespread use of telehealth continue to pose challenges. The future outlook for advancing the use of telehealth in home dialysis depends on integrating the technology with an efficient home program workflow, addressing Internet infrastructure, technological literacy, and socioeconomic determinants of health [13].
Based on the above discussion, the main conclusion is that there is a lack of uniform methods to evaluate ICT intervention in telehealth. Future studies will need to focus on long-term use, uptake and outcomes of RM. Larger, prospective studies will be useful to better explain the effect of RM on HHD [14]. At present, the cost of technology to improve EHD treatments [15] is too high for the public health system to support and scale up to a large number of patients.
We agree that future research should focus on tools designed to support CKD prevention, because ICT can do more for renal patients before the need for RRT.
The novelty of the current review
To prepare for our review, we started by looking for several reviews in the same field. We noted that recently published review papers concerning the ICT interventions to improve HD are fewer than ICT intervention in PD. Most of these reviews included diverse topics, resulting in varying degrees of novelty. Although some studies have explored the impact of ICT intervention overall RRT, most of them only focus on RPM in Peritoneal Dialysis. As such, the other type of RRT such as HD, with other types of ICT interventions remains under-exploited. Additionally, only one research quantitatively analyzes the energy performance of ICT in terms of percentage range, and it only concerns one ICT type. Studies that utilize geographic distribution analysis have also only performed superficial evaluations of the number of publications in each geographic region.
Compared to the analyzed review papers, the novelty aspects of our research could be summarized as follows:
- It critically evaluates all kinds of ICT intervention in HD (at home or in-center).The focus is put on compiling the achieved outcomes and gaps detected.
- It identifies the factors that should be considered to improve patient outcomes and cost savings.
- It provides an overview of the geographical distribution characteristics of the included studies.
- It identifies the benefits results from the ICT intervention in HD and outlines the future research recommended, as well.
The authors recognize several limitations. Several significant databases, and logically combined search terms were employed in our review, however there may be other relevant papers not included. All the evidence suggested that the enormous benefits to HD patients should be focused on a different approach [16].
These articles are congruent with other systematic reviews on the intervention of a specific type of ICT research in HD, which has shown many improvements to HD patient care. Limitations and Future Research are listed in Supplementary Table 1, with a detailed list of situations that need to be addressed.
There is a need for longer-term studies in order to determine whether the benefits demonstrated in time and participant limited trials are sustained [17,18].
Limitations
The ICT interventions among HD patients should include both qualitative and quantitative evaluations of patient-reported outcomes. RPM will be an important adjunct in shaping the expansion of “tele-nephrology” [18] (telemedicine applied to nephrology). RPM faces a lack of acceptance and education among physicians, support from family and friends, and difficulty organizing trips to the necessary periodic assessments by the HCP [19]. The RPM system [20] without data mining does not provide HCP with tools to extract easily useful information. The most important limitation of home-based dialysis therapies is the lack of contact between the clinician and the patient [21].
In the field of Tele-nephrology applied to HD, the initial resistance of nurses was probably greater than that of patients due to the possibility of evaluating their care performance [22], generating a feeling of discomfort.
Older patients tend to refuse Tele-nephrology, and connection difficulties usually bother the teleconsultations [23] presumably due to telephone network overload. A potential barrier to wider uptake of this kind of ICT intervention in HD may be limited internet connectivity for some patients.
Self-Management program for HD patients should include a nursing intervention program that involves a mobile application to improve [24] the self-management of hemodialysis patients.
When considering Telehealth by an inter-professional Team for HD patients, it usually presents some limitations such as older population [25], mostly men, and potentially underpowered. The web-based eHealth portal for delivery of care to home dialysis patients is limited by the small sample size and limited response rate.
For telematics homecare dialysis, there are some design considerations and technical limitations [26] in existing solutions that prohibit the widespread adoption of such services [27].
Future Research
Our review identified several avenues of research for ICT intervention in HD therapy for bioengineers interested in this field (Supplementary Table 1). Development of fluids with nanoparticles with specific thermal and optical properties [2], additional oversight to provide education, periodic assessment by the care team to ensure patient safety while using the RPM, performing studies focused on longer-term use, acceptance, and outcomes of RPM [3]. In the future, RPM should include data mining tools that allow the user to extract reports and consultations with specific information. Smart wearable sensors for real-time monitoring of dialysis patients are something that can help achieve 4P medicine [3] (i.e., Predictive, Precise, Preventive, and Personalized) [3]. It is strongly recommended to investigate the effectiveness of electronic consultation or teleconsultation when compared to face-to-face.
An in-deep study that can gather useful information to guide the most efficacies in the use of telehealth applied to dialysis [5]. Further studies are needed to show the impact of telemedicine on Nephrologists, nurses, and all HCPs participating in an HHD program [6].
For self-management more precise information is expected regarding the cases in which conditions are not good and further investigations will be required to find the best balance between detail and simplicity. It is also necessary to develop a nursing intervention program that involves a mobile application to improve the self-management of hemodialysis patients [28] and promote research regarding nursing interventions for hemodialysis patients to improve their self-management based on various theoretical frameworks.
Future outlook for advancing the use of telehealth in home dialysis depends [29] on the integration of the technology with an efficient home program workflow. Self-management mobile applications should be developed by analyzing and deepening the needs of home hemodialysis (HDD) patients.
Conclusion
This global context-based systematic review of ICT intervention in HD therapy will address significant outcomes, gaps, and ideas for future research. ICT can bring multiple benefits in various aspects (e.g., outcome improvements, lower improvements, increased patient satisfaction and acceptance, cost saving, patient and HCP time saving, increased patient independence, remote monitoring, patient education, and so forth). Although this study is framed as an ICT intervention in HD review, the major goal is to evaluate the better role that ICT can play in HD therapy.
This systematic review found that the ICT intervention in HD therapy brings many benefits and provides an overview of studies investigating ICT-based interventions to improve the care of patients in need of hemodialysis.
Several types of ICT interventions contribute to improving the care of patients on HHD by improving the outcomes, reducing hospitalization, improving treatment adherence, improving quality of life, reducing the cost of patient travel and the consequent footprint, improving the autonomy and confidence of the patient, better adequacy of the prescription, time-saving for HCP and the patient as well. All the benefits listed come from the integration of ICT in the procedures of the HHD therapy. Furthermore, ICT interventions can play a very important role in patient education, CKD self-management, improve home Dialysis, tele-nephrology, and remote monitoring of patients, which is a key factor for an effective management strategy to increase patient independence from nephrology units.
There was a small but statistically significant reduction in patient hospitalizations after the adoption of ICT tools. Patients and clinicians found the ICT interventions easy to use and were satisfied with the improvements achieved.
The results collected through this systematic review led to the identification of different advantages concerning the use of ICT in HD therapy in general. It is remarkable to conclude that more than twenty-five percent of the included studies have health cost reduction (Supplementary Table 1) as the outcome, and twenty percent showed quality of life improvement (Supplementary Table 1). Another inference from these studies is that the promise of better outcomes and lower costs can be realized with ICT tools intervention.
This study has several strengths: the analysis of various types of ICT interventions in HD therapy and the list of all identified benefits of ICT interventions on the HD that represent a big challenge worldwide for the current decade. Our study also listed the limitations of the ICT interventions on HD therapies, and this can be guide for future researches.
We concluded that there are about 8 most common types of ICT interventions in HD therapy, and this may provide a reference for the future of ICT interventions in HD. In addition, identified several benefits that ICT interventions bring to HD therapy. Overall, we conclude that ICT intervention in HHD is the cornerstone of kidney disease management optimization.
Implications for practice and research
This systematic review showed that ICTs can make a significant contribution to HD therapy, improving treatment adherence, outcomes, and quality of life; reducing costs and geographical burdens; saving time for patients and HCP, etc. However, the authors believe that ICTs should be applied to manage and prevent kidney disease in its earlier stages to minimize the number of patients whose life expectancy depends on HD therapy. Additionally, the prevention will contribute to reducing the environmental effects of hemodialysis treatment.
Relevance for Clinical Practice
- ICT intervention in HD therapy enhanced patient access to care
- Improved communication and increased adherence to treatment
- Reduced travel needs and environmental mpact
Author Contributions
CTB-UPM1 conceived, conducted reviewed and edited the study. CTB-UPM2&CIBRBBN-ISCIII and HDES reviewed, commented and edited and approved the final version of the manuscript. All authors contributed significantly to the study design. Material preparation, data collection, verification, and validation. The analyses were performed by CTB-UPM1, CTB-UPM2&CIBRBBN-ISCIII and HDES. The first draft of the manuscript was written by CTB-UPM1 and all authors commented on previous versions of the manuscript. All authors read and approved the final version of the manuscript, no other contributors assisted the authors in this work.
Ethics Approval and Consent to Participate
Not applicable.
Funding
The authors did not receive financial support for the research, authorship, and/or publication of this article.
Consent for Publication
Not applicable.
Supplementary Information
The list of included articles is available in Supplementary Table 1.
Acknowledgments
Special thanks to the professor Herlander Mata-Lima for the reviews and comments on the study. Thank Nieves Linares for assisting with the language review and exporting the search into EndNote and removing the duplicates. We would like to thank the experts in this area who recommended studies for potential inclusion in this review.
Conflict of Interest Statement
The lead / Corresponding author (Abel Mata-Lima) affirms that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
The authors declared that there is no potential conflict of interest concerning the research, authorship, and/or publication of this article.
References
2. Sharma MK, Wieringa FP, Frijns AJ, Kooman JP. On-line monitoring of electrolytes in hemodialysis: on the road towards individualizing treatment. Expert Rev Med Devices. 2016 Oct;13(10):933–43.
3. Wieringa FP, Kooman JP. Smart sensors for real-time monitoring of patients on dialysis. Nat Rev Nephrol. 2020 Oct;16(10):554–5.
4. Nicdao MA, Kim J, Baldacchino T, Jung YH, Mikaheal M, Patekar A, et al. 'My Home Hemo'app-a new telehealth tool for remote monitoring of patients on home haemodialysis. Renal Society of Australasia Journal. 2016 Jul;12(2):41–7.
5. Wallace EL, Rosner MH, Alscher MD, Schmitt CP, Jain A, Tentori F, et al. Remote Patient Management for Home Dialysis Patients. Kidney Int Rep. 2017 Jul 29;2(6):1009-–17.
6. Scofano R, Monteiro A, Motta L. Evaluation of the experience with the use of telemedicine in a home dialysis program-a qualitative and quantitative study. BMC Nephrol. 2022 May 19;23(1):190.
7. Hussein WF, Bennett PN, Pace S, Chen S, Legg V, Atwal J, et al. The Mobile Health Readiness of People Receiving In-Center Hemodialysis and Home Dialysis. Clin J Am Soc Nephrol. 2020 Dec 31;16(1):98–106.
8. Sota Y, Yamamoto K, Hirakawa M, Doi S, Yamamoto Y. Support of self-management for chronic kidney failure patients. InProceedings of the 2011 Visual Information Communication-International Symposium 2011 Aug 4 (pp. 1-7).
9. Park OL, Kim SR. Integrated self-management program effects on hemodialysis patients: A quasi-experimental study. Jpn J Nurs Sci. 2019 Oct;16(4):396–406.
10. Hazara AM, Durrans K, Bhandari S. The role of patient portals in enhancing self-care in patients with renal conditions. Clin Kidney J. 2019 Nov 18;13(1):1–7.
11. Morosetti M, Famà MI. MO029 Clinical and social advantages of remote patient monitoring in home dialysis. Nephrology Dialysis Transplantation. 2020 Jun 1;35(Supplement_3):gfaa140-MO029.
12. Cozzolino M, Piccoli GB, Ikizler TA, Ronco C. The COVID-19 infection in dialysis: are home-based renal replacement therapies a way to improve patient management? J Nephrol. 2020 Aug;33(4):629–31.
13. Lew SQ, Wallace EL, Srivatana V, Warady BA, Watnick S, Hood J, et al. Telehealth for Home Dialysis in COVID-19 and Beyond: A Perspective From the American Society of Nephrology COVID-19 Home Dialysis Subcommittee. Am J Kidney Dis. 2021 Jan;77(1):142–8.
14. Liu N, Kim J, Jung Y, Arisy A, Nicdao MA, Mikaheal M, et al. Remote Monitoring Systems for Chronic Patients on Home Hemodialysis: Field Test of a Copresence-Enhanced Design. JMIR Hum Factors. 2017 Aug 29;4(3):e21.
15. Kiberd J, Khan U, Stockman C, Radhakrishnan A, Phillips M, Kiberd BA, et al. Effectiveness of a Web-Based eHealth Portal for Delivery of Care to Home Dialysis Patients: A Single-Arm Pilot Study. Can J Kidney Health Dis. 2018 Sep 7;5:2054358118794415.
16. Wang SM, Hsiao LC, Ting IW, Yu TM, Liang CC, Kuo HL, et al. Multidisciplinary care in patients with chronic kidney disease: A systematic review and meta-analysis. Eur J Intern Med. 2015 Oct;26(8):640–5.
17. Hall YN, Larive B, Painter P, Kaysen GA, Lindsay RM, Nissenson AR, et al; Frequent Hemodialysis Network Trial Group. Effects of six versus three times per week hemodialysis on physical performance, health, and functioning: Frequent Hemodialysis Network (FHN) randomized trials. Clin J Am Soc Nephrol. 2012 May;7(5):782–94.
18. Ladino MA, Wiley J, Schulman IH, Sabucedo AJ, Garcia D, Cardona JM, et al. Tele-Nephrology: A Feasible Way to Improve Access to Care for Patients with Kidney Disease Who Reside in Underserved Areas. Telemed J E Health. 2016 Aug;22(8):650–4.
19. Schrauben SJ, Appel L, Rivera E, Lora CM, Lash JP, Chen J, rt al. Mobile health (mHealth) technology: assessment of availability, acceptability, and use in CKD. Am J Kidney Dis. 2021 Jun 1;77(6):941–50.
20. Nygård HT, Nguyen L, Berg RC. Effect of remote patient monitoring for patients with chronic kidney disease who perform dialysis at home: a systematic review. BMJ Open. 2022 Dec 7;12(12):e061772.
21. Walker RC, Howard K, Morton RL. Home hemodialysis: a comprehensive review of patient-centered and economic considerations. Clinicoecon Outcomes Res. 2017 Feb 16;9:149–61.
22. Richard Bodington, Xenophon Kassianides, Sunil Bhandari, Point-of-care testing technologies for the home in chronic kidney disease: a narrative review, Clinical Kidney Journal, Volume 14, Issue 11, November 2021, Pages 2316–31
23. Valentijn PP, Pereira FA, Ruospo M, Palmer SC, Hegbrant J, Sterner CW, et al. Person-Centered Integrated Care for Chronic Kidney Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Clin J Am Soc Nephrol. 2018 Mar 7;13(3):375–86.
24. Mattila E, Lappalainen R, Pärkkä J, Salminen J, Korhonen I. Use of a mobile phone diary for observing weight management and related behaviours. J Telemed Telecare. 2010;16(5):260–4.
25. Crowley ST, Belcher J, Choudhury D, Griffin C, Pichler R, Robey B, et al. Targeting Access to Kidney Care Via Telehealth: The VA Experience. Adv Chronic Kidney Dis. 2017 Jan;24(1):22–30.
26. Donald M, Kahlon BK, Beanlands H, Straus S, Ronksley P, Herrington G, et al. Self-management interventions for adults with chronic kidney disease: a scoping review. BMJ Open. 2018 Mar 22;8(3):e019814.
27. Ahmad M, Wallace EL, Jain G. Setting Up and Expanding a Home Dialysis Program: Is There a Recipe for Success? Kidney360.
28. Vegesna A, Tran M, Angelaccio M, Arcona S. Remote Patient Monitoring via Non-Invasive Digital Technologies: A Systematic Review. Telemed J E Health. 2017 Jan;23(1):3–17.
29. Jayanti A, Nikam M, Ebah L, Dutton G, Morris J, Mitra S. Technique survival in home haemodialysis: a composite success rate and its risk predictors in a prospective longitudinal cohort from a tertiary renal network programme. Nephrol Dial Transplant. 2013 Oct;28(10):2612–20.