Abstract
Kinking of an epidural catheter is a rare complication associated with the catheter material, diameter, design and length of introduction inside the epidural space. Flushing test should be attempted before fixation of the catheter on the skin to ensure its normal function. If a kink located distal to the skin is suspected, a slight withdrawal could relieve the obstruction, but usually the complete withdrawal and new catheter placement is needed. We describe the clinical case of a laboring patient whose epidural catheter placement was complicated with a kink inside the epidural space.
Keywords
Catheter obstruction, Epidural analgesia, Epidural anesthesia
Introduction
Kinking, knotting, entrapment and breakage are very unusual complications related to epidural catheters that may prevent normal functioning or even hamper its withdrawal. There is no data regarding the incidence of epidural catheter kinking. Typically, the number of kinks is one or two, but there is a reported case of an epidural catheter presenting around 6 kinks [1-5]. We present here a clinical case of a laboring patient whose epidural catheter was found kinked in the inner body, precisely inside the epidural space, just after its placement.
Clinical Case
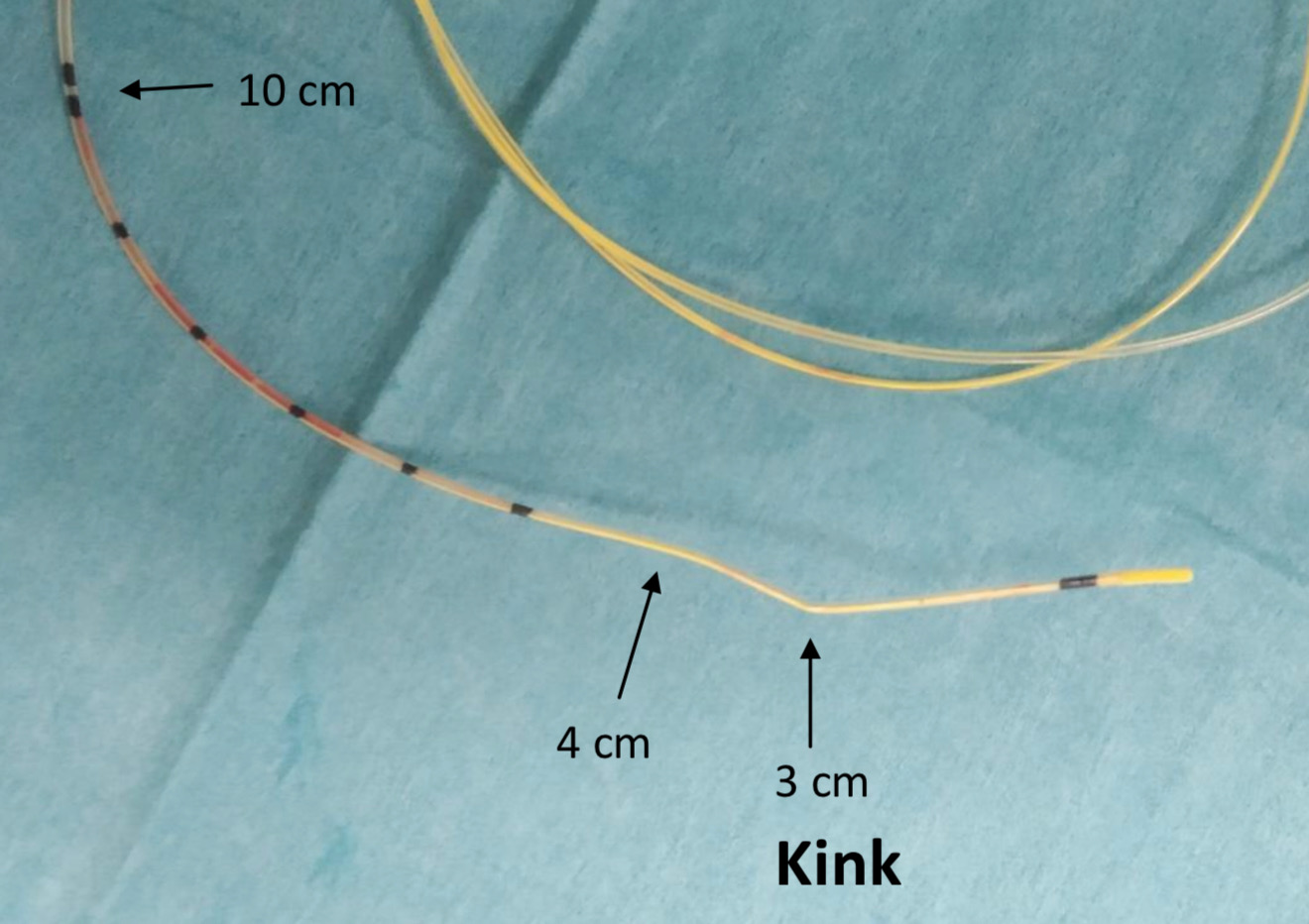
Figure 1: Original figure showing an epidural catheter with a kink at 3 cm from the distal end. As the epidural space was found at 6 cm from skin and the catheter was placed with its 10 cm mark just at the level of the skin, then the distal 4 cm of the catheter were located inside the epidural space, including the observed kink.
Discussion
Accidental kinking of an epidural catheter is very unusual and has been reported both proximal and distal to the skin entry [1-5]. Technical properties of epidural catheters such as the material, design and diameter can influence its tendency to kink, and this can be easily assessed by bending the catheter with two fingers, as suggested by Beamer and French [6].
Regarding physical characteristics, an epidural catheter should be firm enough to pass through the Tuohy needle easily and advance a few centimeters into the epidural space, but at the same time, it should be flexible enough to avoid tissue puncture, with the risk of dural puncture or intravascular cannulation. Newer catheters used nowadays are made of materials with a good balance between firmness and flexibility. Wire-reinforcement can also make catheters more resistant to kinking. The length of advancement of a catheter into the epidural space increases the risk of catheter kinking and displacement. For this reason, some authors recommend the insertion of no more than 2 cm with single end-hole catheters, and 4 cm with multiple hole catheters, as we did [1].
In our case, during catheter threading through the Tuohy needle, some resistance to introduction was felt and disappeared after pushing against resistance, as was also noted in other cases where catheter kinks were reported [4].
Baran O reported a clinical case of an epidural catheter kink where flushing was not checked after catheter placement and three hours later epidural anesthesia was required during surgery but catheter dysfunction was noted and conversion to general anesthesia was required [4]. Whenever an epidural catheter is placed, flushing should be attempted before its complete fixation on the skin, because this could ensure a normal functioning, as we performed in our case.
If a complete obstruction of an epidural catheter is found, the visible parts should be examined searching for kinks or knots formation. If no alteration is found, one possible way of relieving an occlusion is withdrawing the catheter slightly, which we did not attempt in our case. If the obstruction persists, complete withdrawal and new catheter placement may be necessary [1-5].
Conclusions
Kinking of an epidural catheter is a rare complication that usually requires the removal and new catheter placement, especially whenever the kink is located distal to the skin entry. Flushing the epidural catheter should be routinely performed after its placement to dismiss any possible kink or knot formation.
Conflict of Interest
The author declares not having any conflict of interest, and have received no funding for the work.
Informed Consent
The patient gave written informed consent for the scientific publication of her medical record and images.
References
2. Bhakta P, Olteanu DS, Zaheer H. 90° kinking of Vygon epidural catheter. J Anesth. 2017; 31:796.
3. Tandon M, Pandey CK, Pandey VK. Epidural catheter kinking over the scapular margins. Indian J Anaesth. 2013; 57(3):318-9.
4. Baran O, Kir B, Ates I, Şahin A. A kinked epidural catheter. Saudi J Anaesth. 2019; 13(2): 158–159.
5. Dhar M, Anilakumari D, Shajahan MS, Gupta V. Multiple kinking in a single epidural catheter; rare complication or a defect in the catheter?. Arch Anesthesiol Crit Care. 2021; 7(3): 199-200.
6. Beamer J, French GW. A simple method for testing for the kinking epidural catheter. Anaesthesia. 2000; 55(12):1233-4.