Abstract
Hypertension remains as one of the most important public health challenges worldwide because of the associated morbidity, mortality, and the cost to the society. Despite the availability of safe and effective antihypertensive medications and the existence of clear treatment guidelines, hypertension is still inadequately controlled in a large proportion of patients worldwide. Unawareness of lifestyle modifications, and failure to apply these were one of the identified patient-related barriers to blood pressure control. This cross-sectional study was conducted to assess knowledge, attitude and practice of life style modification in the management of hypertension among 100 conveniently selected study subjects. Average age of the patients was 36.96±13.04 years. More than half of the respondents (56%) passed SSC (Secondary School Certificate) level of education. Almost 99% of the study subjects knew that smoking is associated with hypertension. About 94% respondent told excessive salt intake is bad for health. Almost all of them knew that excessive salt intake results high blood pressure. About 93% told that physical exercise has effect on blood pressure. Three-fourth of the study subjects told that physical exercise decrease cholesterol. About 40% took part physical exercise regularly. The study found levels of knowledge on non-drug control of hypertension was quite good but practice level was poor.
Keywords
Knowledge, Attitude, Practice, Life style modification, Management, Hypertension
Introduction
Hypertension is a major risk factor for non-communicable diseases like stroke, cardiovascular disease, and chronic kidney disease. Complications of hypertension account for 9.4 million deaths worldwide every year. Hypertension is responsible for 45% of deaths due to heart disease and 51% of deaths due to stroke [1]. Hypertension, an important and common risk factor for considerable morbidity and mortality not only in the industrialized world but also in developing countries. Thus, the problem of hypertension can be truly considered as pandemic [2]. Life style modifications are universally accepted, not only as the first step in the management of hypertension but also as a way to prevent hypertension. In addition to lowering blood pressure, these measures can also reduce other cardio vascular risk factors. This cost involved is minimal and there are hardly any risks. Hypertensive patients irrespective of this stage or grade should be motivated to adopt these measures [3]. High blood pressure ranked as the leading single risk factor for global burden of disease. Additionally, high blood pressure was one of the 5 leading risk factors for Global Burden of Disease in all regions with the exception of Oceania, Eastern sub-Saharan Africa, and Western sub-Saharan Africa. In these regions, high blood pressure was ranked as the number 6 risk factor attributable to burden of disease. The high prevalence of hypertension, particularly in Asia, has contributed to the present pandemic of cardiovascular disease and death. Highly populated developing Asian countries, such as India and China, have a large absolute number of individuals with hypertension. Up to now, the epidemiology of hypertension in the Western world is well studied, but there are less data concerning the scope of the problem of hypertension in Asian countries. Hypertension is an increasing problem in Southeast Asia, particularly in Bangladesh. Although some epidemiological studies on hypertension have been conducted in Bangladesh, but awareness level on hypertension in this nation remain unclear. Increasing public awareness is the key, as is access to early detection. Raised blood pressure is a serious warning sign that significant lifestyle changes are urgently needed. People need to know why raised blood pressure is dangerous, and how to take steps to control it. To raise this kind of awareness, countries need systems and services in place to promote universal health coverage and support healthy lifestyles: eating a balanced diet, reducing salt intake, avoiding harmful use of alcohol, getting regular exercise and shunning tobacco. Access to good quality medicines, which are effective and inexpensive, is also vital, particularly at the primary care level. As with other non-communicable diseases, awareness aids early detection while self-care helps ensure regular intake of medication, healthy behaviors and better control of the condition.
Methods
This was descriptive type of cross-sectional study, conducted among hypertensive patients. Data were collected from conveniently selected places of Dhaka. This study was conducted for a period of six months. Non-probability convenient sampling technique was applied. A semi-structured pre-tested & self-administered questionnaire was used to collect data. Data were collected by pre-tested structured questionnaires and in face-to-face interview. Information about socio-demographic characteristics was also obtained. Life style modification includes smoking, physical activity, and dietary habit was obtained. The respondents were selected consecutively who met the inclusion and exclusion criteria. After data collection, data were sent to the researcher, which was sorted, scrutinized by the researcher himself by the selection criteria and then data were analyzed by personal computer by SPSS version 20.0 program. The open-ended questions were grouped and categorized. Data were analyzed by descriptive statistics. Limitations of studies are very common in social work. One of the major difficulties was the time constraint. Some respondents were incapable of understanding the importance for conducting a study. Hence, they showed deprecating attitudes toward the interviews or skip some questions. In some cases, they showed non-cooperation and considered the interviews a waste of time.
Results
Average age of the patients was 36.96±13.04. Most of the patients (68%) belonged to 26-50 years age group followed by ≤25 years 19% and 51-75 years 13% (Table 1). Male and female distribution was 73% and 27% (Figure 1). More than half of the respondents (56%) passed SSC level of education followed by graduate 31%, primary 8% and post graduate 5% (Figure 2). Housewife, shopkeeper, business, service and other type of jobs were 16%, 1%, 24%, 28%, and 31% (Figure 3). About 73% of the study subjects had monthly income 10001–20000 BDT followed by 13% family had 20001–30000 BDT, 10% family had ≤10000 BDT and 4% family had >30000 BDT (Table 2).
|
Age group (yrs) |
Number |
Percentage |
|
≤25 |
19 |
19 |
|
26-50 |
68 |
68 |
|
51-75 |
13 |
13 |
|
Total |
100 |
100 |
|
Mean±SD |
36.96±13.04 |
|

Figure 1. Gender distribution.

Figure 2. Educational status distribution.
|
Income |
Number |
Percentage |
|
≤10000 |
10 |
10 |
|
10001–20000 |
73 |
73 |
|
20001–30000 |
13 |
13 |
|
>30000 |
4 |
4 |
|
Total |
100 |
100 |
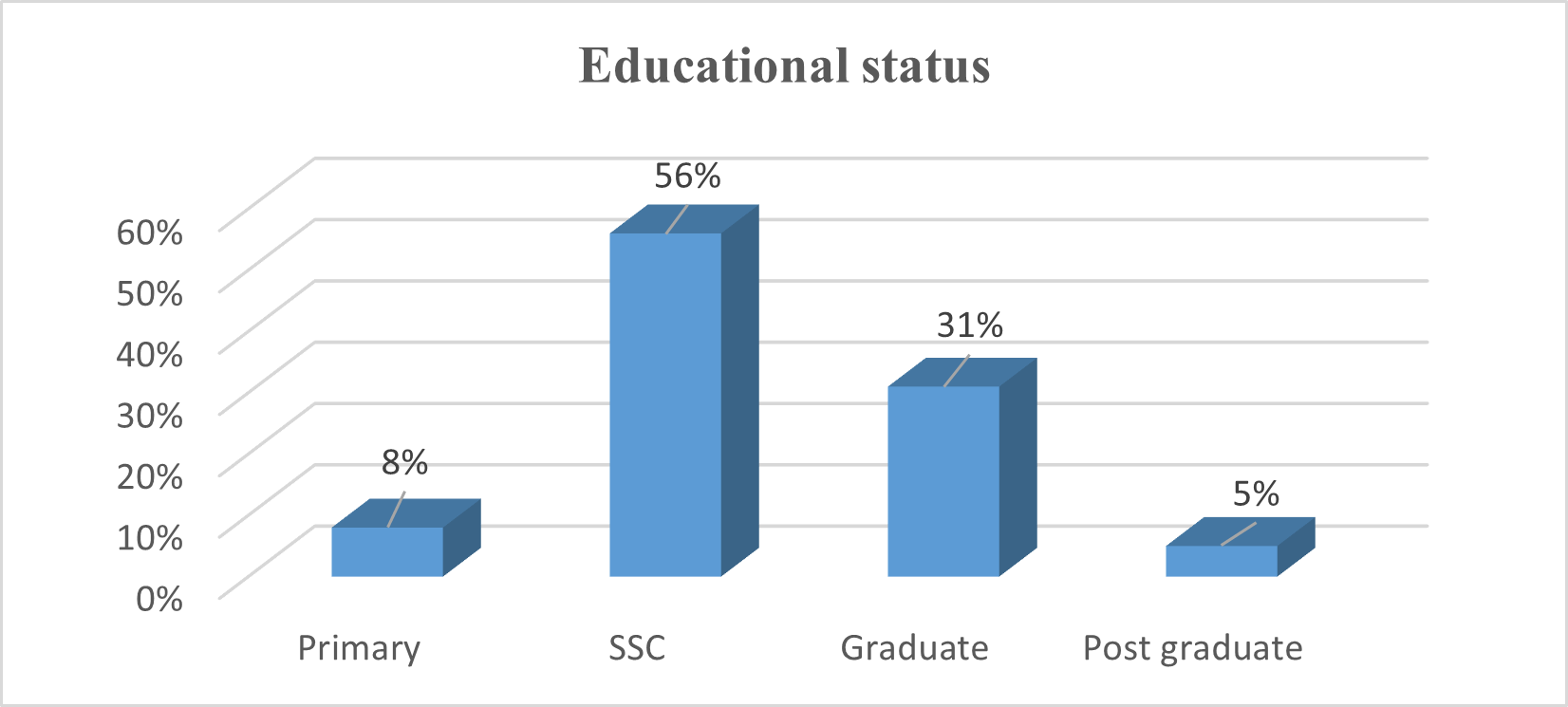
Figure 3. Occupational status of the respondents.
Almost 99% of the study subjects knew that smoking is associated with hypertension. More than half of the respondents told cancer is the effect of smoking followed by lung cancer 19%, tuberculosis 14%, stroke 8%, and hypertension 1% (Table 3). About 77% respondents did not smoke and 23% study subjects smoked. Among smokers average years of smoking was 11.74 years and average sticks 21.91 consumed per week (Table 4). About 94% respondent told excessive salt intake is bad for health. Almost all of them knew that excessive salt intake results high blood pressure. Average amount of salt intake was 2.44 tsf every day (Table 5). About 93% told that physical exercise has effect on blood pressure. Three-fourth of the study subjects told that physical exercise decrease cholesterol. About 40% took part physical exercise regularly. Average physical exercise per day was 66.20 minutes (Table 6). Normal, overweight, underweight and obese were 60%, 30%, 7%, and 3% (Figure 4). Meat, egg, milk, fish and fruits were taken by 89%, 96%, 70%, 98%, and 63% respondents (Table 7).
|
Knowledge |
Number |
Percentage |
|
Is there any association between smoking and hypertension? |
||
|
Yes |
99 |
99 |
|
No |
1 |
1 |
|
If yes, what type of association? |
||
|
Cancer |
58 |
58 |
|
Hypertension |
1 |
1 |
|
Lung cancer |
19 |
19 |
|
Tuberculosis |
14 |
14 |
|
Stroke |
8 |
8 |
|
Total |
100 |
100 |
|
Practice |
Number |
Percentage |
|
Do you smoke? |
||
|
Yes |
23 |
23 |
|
No |
77 |
77 |
|
If yes, how long in years? |
||
|
Mean±SD |
11.74±11.96 |
|
|
How many sticks every week? |
||
|
Mean±SD |
21.91±14.26 |
|
|
Total |
100 |
100 |
|
Knowledge |
Number |
Percentage |
|
|
Excessive salt intake is good or bad for health? |
|||
|
Bad |
94 |
94 |
|
|
Good |
6 |
6 |
|
|
Effect of excessive salt intake |
|||
|
Hypertension |
100 |
100 |
|
|
Average amount of salt intake every day (tsf) |
|||
|
Mean±SD |
2.44±1.68 |
||
|
Total |
100 |
100 |
|

Figure 4. Nutritional status of the study subjects.
|
Knowledge |
Number |
Percentage |
|
Is there any effect of physical exercise on blood pressure? |
||
|
Yes |
93 |
93 |
|
No |
7 |
7 |
|
If yes, what are those? |
||
|
Fitness |
26 |
26 |
|
Decrease cholesterol |
74 |
74 |
|
Do you take part physical exercise regularly? |
||
|
Yes |
40 |
40 |
|
No |
60 |
60 |
|
If yes, how long in minute? |
||
|
Mean±SD |
66.22±34.50 |
|
|
Total |
100 |
100 |
|
Food item |
Number |
Percentage |
|
Meat |
||
|
Yes |
89 |
89 |
|
No |
11 |
11 |
|
Egg |
||
|
Yes |
96 |
96 |
|
No |
4 |
4 |
|
Milk |
||
|
Yes |
70 |
70 |
|
No |
30 |
30 |
|
Fish |
||
|
Yes |
98 |
98 |
|
No |
2 |
2 |
|
Fruits |
||
|
Yes |
63 |
63 |
|
No |
37 |
37 |
|
Total |
100 |
100 |
Discussion
Hypertension is an overwhelming global challenge. Appropriate lifestyle changes are the cornerstone for the prevention of hypertension. They are also important for its treatment; although they should never delay the initiation of drug therapy in patients at a high level of risk. Lack of knowledge, attitude and practice are some of the barriers of having a healthy lifestyle and controlling high blood pressure. The present study found that 99% of the study subjects knew that smoking is associated with hypertension. More than half of the respondents told cancer is the effect of smoking. Good knowledge about salt, alcohol and smoking effect is an essential part of successful treatment of hypertension. A study showed 94.6%, 83.8%, and 59.9% participants had knowledge of the danger of salt, alcohol and smoking on hypertension management, respectively. Eighty percent, 85% and 98.5% of the participants avoid adding salt in their food, drinking alcohol and smoking, respectively [4]. The number of participants with knowledge about salt restriction and avoiding smoking are more than the findings in a research done in Ghana, (60%) and (38%), respectively. Regarding the knowledge about the balanced diet, only 39.2% know the importance of balanced diet and this finding is low when compared with research done in Ghana (59%) [5]. This study revealed that 94% respondent told excessive salt intake is bad for health. Almost all of them knew that excessive salt intake results high blood pressure. The patient’s knowledge on blood pressure and exercise was 59.2% and 67.7%, respectively [4]. The attitude toward exercise is good when compared with the result of a research done in Ghana (60%) [5]. On the contrary, knowledge about hypertension is low when compared with a research done in Kinondoni Municipality, Dar es Salaam (66.8%) [6]. It is possible to prevent the development of hypertension and to lower blood pressure levels by simply adopting a healthy lifestyle. The recommended lifestyle measures that have been shown to be capable of reducing blood pressure include: (i) salt restriction, (ii) moderation of alcohol consumption, (iii) high consumption of vegetables and fruits and low-fat and other types of diet, (iv) weight reduction and maintenance and (v) regular physical exercise. In addition, insistence on cessation of smoking should be part of any comprehensive lifestyle modification plan to reduce the risk of high blood pressure and cardiovascular disease [7,8]. Hypertensive patients irrespective of their stage or grade should be motivated to adopt these measures. Motivating patients to implement lifestyle changes is probably one of the most difficult aspects of managing hypertension. In this study 93% told that physical exercise has effect on blood pressure. Three-fourth of the study subjects told that physical exercise decrease cholesterol. About 40% took part physical exercise regularly. Average physical exercise per day was 66.20 minute. Assessment of the level of patient physical activity revealed that 10.2% of the patients reported to practice “little or no activity”, 32.0% reported occasional activity, 41.8% walked briskly or run and only 14% claimed doing regular physical activity. The number of patients who did vigorous physical activity (regular physical activity) and walked briskly or run is low when compared with a study done in Nairobi, Kenya 75.7% and 77.4% respectively [9]. Furthermore, the number of patients who walk briskly is low when compared with the finding in Nigeria (99.3%) [10]. This may be due to poor knowledge on the importance of physical activity in management of hypertension. The patient’s daily activity among study participants as measured in this study was, sitting 18.5%, standing 11.5%, walking 43.1% and heavy labor 27%. The number of patients whose daily activity include sitting was lower when compared with the study done in Nigeria (29%) [11]. The difference may be because of the fact that participants are engaged in different activity to get their daily food and most of them do not have care givers. Different studies have been conducted on lifestyle modification programs and educational interventions for patients with high blood pressure. Despite the effectiveness of educational interventions on the lifestyle of patients with high blood pressure [12], the results of one study showed that educational interventions had no significant effect on weight, blood pressure level and physical activity in people at the risk of ischemic heart diseases [13]. In another study, although health education improved the knowledge of patients with high blood pressure, it had no significant effect on the level of their blood pressure. Another study found no significant effect from educational interventions on blood pressure and another one found no significant relationship between weight changes and changes in diastolic blood pressure [14]. Generally, practice of the participants and their knowledge toward life style modification in management of hypertension is not as required. This may be because of the poor knowledge and poor adherence to the practices. In addition, health professional might not be counseling their clients by giving adequate time regarding the importance of the lifestyle in the management of hypertension and its cost effectiveness.
Conclusion
Knowledge regarding hypertension is an important measure used for decreasing the prevalence of hypertension. Life style modification is the easiest way to prevent or control high pressure. The increase level of knowledge on life style changes will help to have desired intervention goal in people who are most motivated. The study found adequate levels of knowledge on lifestyle modification in case of hypertension but found poor practice of non-drug control of hypertension. About 93% told that physical exercise has effect on blood pressure. Three-fourth of the study subjects told that physical exercise decrease cholesterol. About 40% took part physical exercise regularly. Average physical exercise per day was 66.20 minute.
References
2. Black JM. Medical surgical nursing, 7th edition. New Delhi: B. I. publications private Ltd; 2005. P. 1489–507
3. Wods LS. Cardiac nursing. 5th Edition. Philadelphia: Lippincott Williams and Wilkins publishers; 2005. P. 85
4. Tesema S, Disasa B, Kebamo S, Kadi E. Knowledge, attitude and practice regarding lifestyle modification of hypertensive patients at Jimma University specialized hospital, Ethiopia. Prim Health Care. 2016;6(1):218–21.
5. Marfo AF, Owusu-Daaku FT, Addo MO, Saana II. Ghanaian hypertensive patients understanding of their medicines and life style modification for managing hypertension. Int J Pharm Pharm Sci. 2014;6(4):165–70.
6. Linda M. Knowledge, attitude and practices towards risk factors for hypertension in Kinondoni municipality, Dar es Salaam. Dar Es Salaam Medical Students' Journal. 2007;14(2):59–62.
7. Appel LJ. Lifestyle modification as a means to prevent and treat high blood pressure. Journal of the American Society of Nephrology. 2003 Jul 1;14(suppl_2):S99–102.
8. Wexler R, Aukerman G. Nonpharmacologic strategies for managing hypertension. American Family Physician. 2006 Jun 1;73(11):1953-6.
9. Joshi MD, Ayah R, Njau EK, Wanjiru R, Kayima JK, Njeru EK, et al. Prevalence of hypertension and associated cardiovascular risk factors in an urban slum in Nairobi, Kenya: a population-based survey. BMC Public Health. 2014 Nov 18;14:1177.
10. Awotidebe TO, Adedoyin RA, Rasaq WA, Adeyeye VO, Mbada CE, Akinola OT, et al. Knowledge, attitude and practice of exercise for blood pressure control: a cross-sectional survey. Journal of Exercise Science and Physiotherapy. 2014 Jun;10(1):1–10.
11. Li J, Zheng H, Du HB, Tian XP, Jiang YJ, Zhang SL, et al. The multiple lifestyle modification for patients with prehypertension and hypertension patients: a systematic review protocol. BMJ Open. 2014 Aug 1;4(8):e004920.
12. Dekkers JC, van Wier MF, Ariëns GA, Hendriksen IJ, Pronk NP, Smid T, et al. Comparative effectiveness of lifestyle interventions on cardiovascular risk factors among a Dutch overweight working population: a randomized controlled trial. BMC Public Health. 2011 Jan 24;11(1):49.
13. Pandit AU, Tang JW, Bailey SC, Davis TC, Bocchini MV, Persell SD, et al. Education, literacy, and health: Mediating effects on hypertension knowledge and control. Patient Educ Couns. 2009 Jun;75(3):381–5.
14. Reuther LØ, Paulsen MS, Andersen M, Schultz-Larsen P, Christensen HR, Munck A, et al. Is a targeted intensive intervention effective for improvements in hypertension control? A randomized controlled trial. Fam Pract. 2012 Dec;29(6):626–32.