Abstract
Fungal infections are among the most difficult diseases to diagnose and manage and can cause significant morbidity and mortality. It is estimated that globally, fungal infections occur in at least 13 million people and cause more than 1.5 million deaths every year, costing billions of dollars. Out of millions of fungal species, only several hundred species cause diseases among humans, primarily in immunocompromised and critically ill individuals, and only a very few fungal species can affect healthy individuals. The number of at-risk individuals is unfortunately increasing globally over time due to the rise in immunocompromised population, like diabetes, along with genetic predisposition and environmental factors (e.g., globalization, urbanization, overcrowding, poor living conditions, socioeconomic conditions, climate change). These factors increase mold-infested buildings, exposure to inhibitants, and mold-related health complications. Molds, spores, and hyphal fragments cause variety of allergies among people living or working in mold-infested buildings; exposure to mycotoxins can also cause systemic toxicities to many organs like respiratory and nervous systems, liver, kidney, and developing fetuses; some of them are proven carcinogens. Exposure to mycotoxins can also make individuals susceptible to microbial infections/diseases. To estimate mold infestation inside a building, levels of mold spores and hyphal fragments, is determined in air and dust and compared with the background levels. To understand if other microorganisms may also be responsible for adverse health effects, samples are also collected and analyzed for the presence of pathogenic bacteria and endotoxins. Exposure of inhabitants is estimated by determining levels of mycotoxins in urine (and sometimes in blood) and levels of bacteria and molds in feces. This paper compiles and describes commonly detected molds, their components, mycotoxins, and bacteria from inside of over 800 suspected mold infested buildings and over 2000 residents for the benefit of researchers and those working in this area.
Keywords
MMold, Mycotoxin, Molds indoor, Toxicity of mycotoxins, Adverse health effects of molds, Mold exposure, Mold risk assessment, Mycotoxin exposure, Mycotoxin risk assessment
Introduction
Molds are microscopic fungi, ubiquitous in nature that grow on any moist and/or damp surface containing organic matters. In the presence of considerable moisture (≥ 60% relative humidity) and appropriate temperature (25-30°C, some molds are capable to grow at refrigerator temperatures as well), almost any organic substance will support mold growth. Molds, therefore, can grow on materials like raw and cooked food, wood, paper, carpet, drywall, insulation, plants, soil, wallpaper, fabric, and upholstery (https://www.fsis.usda.gov/food-safety/safe-food-handling-and-preparation/food-safety-basics/molds-food-are-they-dangerous). Body of molds is called thallus, which can range in size and cellularity (single cell or multicellular). Cells within thallus are coated with a wall made of a strong polysaccharide called chitin. Long, branched filaments of molds are called hyphae that form the tangled web, called mycelium, giving mold the characteristic fussy or cottony appearance. Hyphae are made of an outer cell wall and an inner lumen. Molds produce microscopic reproductive bodies (spores) ranging 2-10 μm in size; several types of sexual and asexual spores are produced by molds for their propagation. Spores formed by hyphal fragmentation are called arthrospores, spores surrounded by a thick wall before hyphal fragmentation are called chlamydospores, and spores developed within a sac (sporangium) at the tip of hyphae are called sporangiospores (https://www.uwyo.edu/virtual_edge/lab13/fungi.htm). Spores float in both outdoor and indoor air and start growing into molds when land on moist surfaces; none of the molds grow in the absence of moisture.
Hydrolytic enzymes are secreted from the tips of the hyphae that break complex organic matters into simpler substances for absorption by hyphae, in this way, molds play a major role in decomposing organic materials and recycling nutrients in the ecosystems. Usually during late in growth, many filamentous molds produce complex secondary metabolites, notable among them are antibiotics and mycotoxins. Secondary metabolites are not directly involved in molds’ normal survival and/or growth but often linked to their development by stimulating sporulation, improving survivability of spores, and enhancing the fitness of fungal community through ecological interactions with other organisms [1,2].
Outdoors, molds breakdown dead organic matter like fallen leaves and dead trees. Indoors, under favorable conditions, molds grow and damage common materials like wood, paper, and organic fibers. Indoors, molds remain viable long after the source of moisture is removed resulting in molds and their components (i.e., hyphal fragments, spores, and mycotoxins), referred herein as biotoxins, with the potential to cause adverse health effects, remain in indoor air for an extended period of time [3]. Molds grow outdoors in humid environments and indoors, they are usually found in damp/steamy and dark areas with poor ventilation (e.g., basements, bathrooms, recently flooded areas, cluttered storages, and kitchens) [1,2].
Levels of biotoxins in outdoor air do not normally rise above the health concern, even in high humidity, due to wind mediated dispersal, heat and sun light mediated degradation, and relatively brief durations of exposures of most of the individuals. Indoors, the presence of mold spores is generally not problematic [4], as they are always present, unless they land on a wet or damp surface and begin growing. Levels of biotoxins in indoor air are mostly lower or equal to that of the outdoor air [5]; however, can easily reach unsafe levels from the growth of mold spores under high humidity, inadequate ventilation, and poor lighting, with possibility of causing adverse health effects [6]. This conclusion is supported by the fact that many people, especially susceptible individuals (e.g., immunocompromised and/or genetically predisposed) living or working in mold-infested buildings commonly complain of a variety of adverse health effects. These adverse health effects range from allergies (e.g., hay fever-type symptoms [sneezing, runny nose, red eyes], inflammation, and skin rash) to adverse effects, less commonly, to many organs and systems [1,2,7-24]. Exposure to mycotoxins has been reported to cause fatigue, nausea, immunotoxicity, neurotoxicity (e.g., dizziness, increased anxiety, depression, and cognitive deficits), pulmotoxicity, nephrotoxicity, hepatotoxicity, birth defects, and cancer, usually following high levels of exposure for prolong periods of time [1,18,21,23,25]. Furthermore, exposure to mycotoxins can make individuals vulnerable to microbial diseases [25].
Global prevalence of buildings with dampness and molds is ~47%; as high as 27, 47, 47, and 12% of homes in Europe, America, New Zealand, and China, respectively, have been reported to have moisture and mold issues [26-40]. Mold-affected buildings are persistent and common global problems with evidence of an upward trend due to factors like overcrowding from increasing world population, poor living conditions, socioeconomic conditions, globalization, urbanization, energy efficient buildings, and climate change [15,23,41-51]. Consequently, a rise in fungal infections among humans [52] is seen with climate change (i.e., rise in global temperature, humidity, and population growth). Due to these factors, a further increase in mold-infested buildings and rise in biotoxin-related health effects is anticipated.
To assess mold infestation inside a building, levels of several mold spores and hyphal fragments are determined in air and dust and compared with the background (i.e., outside). Similarly, to determine if exposure to the occupants has occurred and crossed the threshold of adverse health effects, several biological samples (e.g., urine, feces, and blood [rarely]) are collected and analyzed for molds, mycotoxins, and bacteria [24]. Additionally, to cover other microorganisms that may be responsible for adverse health effects, samples are also collected and analyzed for the presence of pathogenic bacteria and endotoxins. This paper reviews specific molds, mycotoxins, and bacteria that the collected samples are routinely analyzed for and/or detected in the collected samples during the inspection of buildings for mold infestation and exposure of occupants.
Sampling and Analysis of Molds, Spores, and other Particulates
Approximately 5 g of dust samples are collected from inside the buildings that are representative of majority of the indoor areas of the building in question, for example, dust by vacuuming, from the ceiling fans, from vacuum cleaner, from heating, ventilation, and air conditioning (HVAC), air inlets/air outlets/filters, or by gathering settled dust from other objects. Samples are preserved and placed into sterile containers and shipped to a microbiology laboratory for the analysis using mold-specific genes with quantitative real-time polymerase chain reaction (qPCR). Samples are routinely analyzed for 36 mold species, 26 of these species are known to thrive in water damaged buildings, designated as “Group 1” mold species, and 10 species are found inside all buildings, with or without water damage, designated as “Group 2” mold species (Table 1). Based on the abundance, buildings are scored for environmental relative moldiness index (ERMI) using the difference between “Group 1” and Group 2” log-transformed values [53]. The list contained 11 species of Aspergillus, 7 species of Penicillium, 4 species of Cladosporium, 2 species of Scopulariopsis and Rhizopus, and 1 species of Acremonium, Alternaria, Aureobasidium, Chaetomium, Epicoccum, Eurotium, Paecilomyces, Stachybotrys, Trichoderma, and Wallemia. Abundance of two species of nonpathogenic molds (Aspergillus flavus, Penicillium purpurogenum) is also determined. In addition to determining ERMI from the generated data, these authors opine that each mold should also be assessed for its toxicity and potential health hazards by knowing number of spores and biotoxins they produce, and their ability to cause short- and long-term adverse health effects mentioned in the preceding section (see “Introduction” above).
|
Mold Species Determined in Collected Dust Samples by Mold-Specific qPCR |
|||
|
Species |
Pathogen |
Species |
Pathogen |
|
Acremonium strictum (g2) |
Y |
Chaetomium globosum |
Y |
|
Alternaria alternata (g2) |
Y |
Epicoccum nigrum (g2) |
Y |
|
Aspergillus flavus |
N |
Eurotium (A.) amstelodami |
Y |
|
A. fumigatus |
Y |
Mucor-Rhizopus Group (g2) |
Y |
|
A. niger |
Y |
Paecilomyces variotii |
Y |
|
A. ochraceus |
Y |
Penicillium brevicompactum |
Y |
|
A. penicllioides |
Y |
P. chrysogenum (g2) |
Y |
|
A. restrictus |
Y |
P. corylophilum |
Y |
|
A. sclerotiorum |
Y |
P. crustosum (group 2) |
Y |
|
A. sydowii |
Y |
P. purpurogenum |
N |
|
A. unguis |
Y |
P. spinulosum |
N |
|
A. ustus (g2) |
Y |
P. variabile |
Y |
|
A. versicolor |
Y |
Rhizopus stolonifer (g2) |
Y |
|
Aureobasidium pullalns |
Y |
Scopulariopsis brevicaulis |
Y |
|
Cladosporium* cladosporioides I (g2) |
Y |
S. chartarum |
Y |
|
C. cladosporioides II (g2) |
Y |
Stachybotrys chartarum |
Y |
|
C. herbarum (g2) |
Y |
Trichoderma viride |
Y |
|
C. sphaerospermum |
Y |
Wallemia sebi |
Y |
|
qPCR, quantitative real-time polymerase chain reaction; Pathogen, pathogenicity; Y, yes; N, no. "(g2)" are "Group 2" species commonly found inside buildings, others are "Group 1" species found in water-damaged buildings. Cladosporium sometimes may not be determined as pathogenic; however, it produces fine and ultra-fine particulates known to cause asthma, lung collapse, and respiratory failure via 1-3-β-D glucan overload in the respiratory system. |
|||
Other samples from inside of buildings are also collected to determine mold spores, hyphal and insect fragments, pollen, and yeast. For this purpose, air and dust samples are collected using sticky slides, tape-lifts, and swabs [24]. The collected samples are analyzed for fungal spores, fungal structures, hyphal fragments, pollen, insect fragments, skin fragments, and fibrous particulate matters/fibers by optical microscopy. (Table 2) shows routinely detected mold spores inside the buildings; the list presents molds that are detected inside of even one out of over 800 buildings sampled by the Mold Case Consulting in the last four years. Molds with no or unknown pathogenicity are not described in this paper.
|
Spores & Mold Particulates in Collected Air, Swab, Tape-Lift, & Bulk Samples Via Optical Microscopy |
|||||
|
Type |
Pathogen* |
Type |
Pathogen* |
Type |
Pathogen* |
|
Acremonium |
Y |
Flosculomyces |
NK |
Scolecobasidium |
NK |
|
Alternaria (Ulocladium) |
Y |
Fusarium |
Y |
Scopulariopsis/Microascus |
Y |
|
Arthrinium |
Y |
Fusicladium/Venturia |
NK |
Smuts/Periconia |
Y |
|
Arthrobotrys |
NK |
Ganoderma |
N |
Spegazzinia |
N |
|
Arthrospores |
NK |
Humicola |
NK |
Spadicoides |
NK |
|
Ascospores |
Y |
Mammaria |
NK |
Sporidesmium |
Y |
|
Ascotricha/Dicyma** |
NK |
Monodictys |
NK |
Sporormiella |
NK |
|
Aspergillus/Penicillium |
Y |
Mucor |
Y |
Sporoschisma |
NK |
|
Basidiospores |
Y |
Mycoenterolobium |
NK |
Stachybotrys/Memnoniella |
Y |
|
Beltrania |
NK |
Myrothecium |
NK |
Sterigmatobotrys |
NK |
|
Bipolaris |
Y |
Myxomycetes |
N |
Stemphylium |
Y |
|
Bispora |
NK |
Myxotrichum |
N |
Syncephalastrum |
Y |
|
Blakeslea/Choanephora |
N |
Nigrospora |
Y |
Tetraploa |
Y |
|
Botrytis |
Y |
Oedocephalum |
NK |
Torula-like |
Y |
|
Cercospora |
Y |
Oidiodendron |
Y |
Triadelphia |
Y |
|
Cephaliophora |
Y |
Oidium |
NK |
Trichoderma |
Y |
|
Chaetoconis |
NK |
Oncopodiella |
NK |
Trichothecium |
Y |
|
Chaetomium |
Y |
Paecilomyces |
Y |
Tripospermum |
NK |
|
Chromelosporium |
NK |
Papulaspora |
Y |
Unidentifiable Spores |
Y |
|
Chrysonilia/Neurospora |
Y |
Peronospora |
N |
Virgaria |
NK |
|
Cladosporium |
Y |
Penicillium/Talaromyces |
Y |
Wallemia |
Y |
|
Coelomycetes |
Y |
Pestalotia/Pestalotiopsis |
Y |
Zygomycetes |
Y |
|
Corynespora |
Y |
Phaeotrichoconis |
Y |
Zygophiala/Schizothyrium |
N |
|
Curvularia |
Y |
Pithomyces |
Y |
Hyphal Fragment |
Y |
|
Dictyosporium |
NK |
Polythrincium |
NK |
Insect Fragment |
Y |
|
Diplocladiella |
NK |
Pyricularia |
NK |
Pollen |
Y |
|
Endophragmia |
NK |
Rhizopus |
Y |
Particulate Matters |
Y |
|
Epicoccum |
Y |
Rust |
Y |
Yeast/Fern |
Y |
|
Pathogen, pathogenicity; Y, yes; N, no; NK, not known - no information found in the literature. *Spores and hyphae of every species of mold are capable of causing common allergies, e.g., respiratory tract, eyes, skin. **When spores of two genus not differentiable under optical microscope, both are listed with "/" in between them. |
|||||
Description of Commonly Detected Molds, Spores, and Particulates
Acremonium
Acremonium grows moderately rapidly with compact and moist colonies containing loose cottony white, gray, or rose hyphae when fully grown. Acremonium grows well indoors under very wet conditions. Acremonium causes nausea, vomiting, and diarrhea in occupants of infested buildings (https://hsrm.umn.edu/node/901). Acremonium infection occurs mostly to immunocompromised individuals. Acremonium is associated with endocarditis, pneumonia, meningitis, cerebritis, peritonitis, arthritis, osteomyelitis, sepsis, and infection of gastrointestinal (GI) tract, eyes, skin, nails, and mouth; because of disseminated infection fungus reaches bloodstream and spread throughout the body [54-58]. It triggers type I allergies (e.g., hay fever, asthma, rhinitis, eye infections, dermatitis, and onychomycosis) and type III hypersensitivity; pneumonitis [57-59]. Type I allergic reactions are mediated by IgE antibodies whereas, type III reactions are mediated by IgM and IgG antibodies.
Several species of Acremonium can produce colonies in human lungs producing pulmonary fungal ball (aspergilloma, a mass of fungus that grows in a lung cavity) sometimes even in immunocompetent individuals; Acremonium can grow colonies in the GI tract and produce bezoars [54]. Acremonium is also known to produce trichothecene mycotoxins which are potent inhibitors of DNA, RNA, and protein syntheses and are known carcinogens [60,61]. Trichothecenes are often linked to both acute and chronic toxicoses including alimentary canal toxic aleukia (nausea, vomiting, diarrhea, leukopenia, hemorrhaging, skin inflammation, and sometimes death) and Kashin-Beck disease [62]. For details about trichothecenes, readers are directed to “Description of the Mycotoxins…” section below.
Alternaria
Alternaria grows rapidly, colonies are grayish white in color at the beginning and darken later, becoming greenish black or olive brown with a light border. Alternaria often grows on carpets, textiles, and horizontal surfaces such as window frames [63]. Alternaria can grow at temperatures ranging from 1–35°C and pH between 2.5–10, with optimum growth at 20–25°C. Spores of Alternaria are large and readily found in air samples, they are capable of depositing in the nose, mouth, and upper respiratory tract [64,65]. They usually attack immunocompromised individuals undergoing prolong steroid treatment or those with very weak immune system. Species of Alternaria can cause hypersensitive pneumonia, bronchial asthma, and allergic sinusitis and rhinitis [66]. They can cause sores in the nose, ulceration of skin, and nail infections. Acute symptoms include edema and bronchospasms, chronic cases may develop pulmonary emphysema [67]. More than 70 mycotoxins have been reported to be produced by Alternaria [68]. Mycotoxins produced by Alternaria are suspected to be mutagenic, genotoxic, teratogenic, fetotoxic, estrogenic, cytotoxic, and carcinogenic [69,70].
Arthrinium
Arthrinium colonies grow rapidly into grape-like masses that appear woolly or cottony white with brown spots. Arthrinium is widespread saprobe commonly found feeding/decomposing dead and decaying wood, leaves, litter, and other organic matter. It is often detected in air near grassy places, especially in fall when plants start to die due to cold weather. At least one species of Arthrinium is allergenic. Arthrinium produces many secondary metabolites (e.g., xanthones, peptides, diterpenes, sesquiterpenes, and quinines). Mycotoxin, 3-nitropropionic acid (3-NPA), a highly toxic compound, produced by Arthrinium, has been reported to cause noninflammatory encephalopathy, preceded by vomiting, nausea, diarrhea, that may lead to coma and death in 10% of the exposed individuals and in some individuals may result in lifelong disabilities [71-73].
Arthrospores
Arthrospores are formed by hyphal fragmentation and are capable of producing allergies in certain individual, especially those prone to getting allergies (e.g., immunocompromised individuals).
Ascospores
Ascospores are sexual spores of Ascomycetes which grow well under a variety of conditions and commonly found growing indoors on damp materials. Ascospores can be single- or multi-cellular and extremely variable in size and shape. Many Ascospores are allergenic, commonly cause coughing, wheezing, nasal congestion, and eye irritation; they are considered potential opportunistic pathogens and producers of toxins. Ascospores have not been studied extensively and therefore only a few are known to cause diseases; however, Ascospores can cause severe irritation and have high allergenic potential - can severely damage organs following long-term exposure [19].
Aspergillus
Aspergillus colonies are generally fast growing, may be woolly or cottony in texture, and in the shades of green, brown, or black. It is found on organic materials like soil, plant debris, compost, stored grain, wood, paper, house dust, ventilation systems, water-damaged building materials (e.g., clothing, carpets). Out of about 300, 16 species of Aspergillus have been reported to cause human diseases. Aspergillus is a common cause of extrinsic asthma, symptoms include edema and bronchospasms, chronic cases may result in pulmonary emphysema. Aspergillosis is the second most common fungal infection requiring hospitalization in the United States. A. fumigatus releases copious amounts of spores which become airborne and can reach alveoli following inhalation. Many Aspergillus species produce mycotoxins (e.g., aflatoxins, ochratoxin A [OTA], sterigmatocystin) capable of causing developmental toxicity, stunted growth, immune suppression, DNA damage, hepatotoxicity, nephrotoxicity; aflatoxins are known hepatocarcinogen. Aflatoxins also cause occasional outbreaks of acute aflatoxicosis that may result in death shortly after exposure [74-81; https://www.adelaide.edu.au/mycology/]. Aflatoxins are known to cause mutation in p53 gene which is also known as the guardian of genome [82]. For details about aflatoxin, OTA, and sterigmatocystin, readers are directed to “Description of the Mycotoxins…” section below.
Aureobasidium
Aureobasidium grows moderately rapidly and is covered with slimy masses of spores. Aureobasidium is yeast like, start with cream to pink in color and become dark brown and velvety with age. It is detected in soil, freshwater, marine estuary sediments, plants, and woods. Aureobasidium spores can be transferred by water droplets when wet and by wind when dry. This mold is, therefore, widespread inside buildings where moisture accumulates, particularly in bathrooms and kitchens, on shower curtains, tile grout, windowsills, textiles, and liquid waste materials. Aureobasidium causes type I allergies and Type III hypersensitivity pneumonitis; it has also been isolated, rarely though, from skin lesions, keratitis (inflammation of the cornea), spleen abscess, and blood of immunocompromised individuals [83; https://library.bustmold.com/aureobasidium/].
Basidiospores
Basidiospores are sexual spores produced by Basidiomycetes, ubiquitous in gardens, forests, and woodlands. Basidiospores are produced on club shaped cells called basidia, each containing four small outgrowths, sterigmata, each producing one spore. Basidiospores are often actively and forcefully released into the surrounding air. They cause type I allergies, type III hypersensitive pneumonitis, and are rare opportunistic pathogens causing eye, skin, and nail infections [84]. Cryptococcus belongs to Basidiomycete, some of which are known to cause severe forms of meningitis called cryptococcosis, especially in immunocompromised individuals, with fatality rates of 9% in high-income regions to over 70% in sub-Saharan Africa [85]. Basidiospores produce many mycotoxins like amanitins, monomethyl-hydrazine, muscarine, ibotenic acid, and psilocybin.
Bipolaris
Bipolaris grows rapidly, even in semi-dry environments, to initially white to grayish brown velvety to woolly turning into olive green to black colonies with raised grayish peripheries as they mature. Bipolaris is a ubiquitous dry spore producing mold; spores are disseminated by wind. It is often found on decaying plants, grasses, and in soil. Bipolaris causes infections of cornea, skin, heart, bone, lungs, and central nervous system causing brain lesions often in immunocompromised but also in young and healthy individuals (https://library.bustmold.com/bipolaris/). In some individuals with severe allergies, large spores of Bipolaris can lodge and attach to the mucus in the sinuses or upper respiratory tract and grow, producing perpetual allergy that can progressively and permanently damage sinuses. Bipolaris, along with Aspergillus, produce mycotoxin sterigmatocystin that is known to cause liver and kidney damage in animals following oral dosing [76; https://www.adelaide.edu.au/mycology/]. For details about sterigmatocystin, readers are directed to “Description of the Mycotoxins…” section below. At least two other mycotoxins (prehelminthosporal and sorokinianin) are also produced by Bipolaris, whose effects on humans are not known [86].
Botrytis
Botrytis initially appears as a white growth on plants that turns to gray quickly. Botrytis produces "dusty" smoky-gray spores that spread by wind or water. Spores of Botrytis can remain dormant on plant surfaces for a very long period of time, sometimes throughout the plants’ life. Botrytis has a low prevalence, both outdoors and indoors. Even with low prevalence, Botrytis causes sensitization with a high prevalence. Species of Botrytis (e.g., B. cinerea) causes allergic rhinitis in children and adults, asthma and hypersensitivity in children, and pneumonitis in individuals working in horticulture/cultivation and harvesting of grapes [87].
Cephaliophora
Cephaliophora has been isolated from soil and animal dung, and found to grow on teak, cotton, poplar, and other plants [88-91]. It is also called “cup fungi” due to macro-structure it forms which is like the shape of a cup [92]. Cephaliophora grows vegetative hyphae which is colorless with copious branching and produces pale to brownish spores [93]. Cephaliophora has been reported to cause mycotic keratitis in humans [94].
Cercospora
Cercospora is a plant parasite, it causes leaf spot mostly in higher plants. Distinctive spores of Cercospora spread through wind and is commonly found outdoors in agricultural areas, especially during harvest; it seldom grows indoors. Cercospora species (e.g., C. apii) has been isolated from patients with cutaneous and subcutaneous lesions involving face, ears and nasal mucosa, failure of therapeutic interventions can lead the infection for many years [95]. Cercospora does not produce any known potential toxins.
Chaetomium
Chaetomium is readily found growing on the damp or water damaged drywalls. Chaetomium produces cottony and white to grey to olive color colonies and grows rapidly. Chaetomium is the third most common indoor mold [96,97]. Chaetomium is allergenic and causes skin and nail infections [98,99]. C. globosum is known to cause pulmonary mycosis, severe brain abscesses, and fatal cerebral infections in immunocompromised individuals [100]. C. globosum is also one of the primary Chaetomium found in the homes of asthmatics individuals [101] with reported invasive Chaetomium infections in the lungs [102]. Chaetomium is known to inhibit cell division and is shown to be fatal to rodents [103]. Chaetomium produces several mycotoxins (e.g., sterigmatocystin, O-methylsterigmatocystin, chaetochromin, chaetoglobsins A and C, chaetocin, chetomin, cochliodinols, and mollicellin G), many are developmental toxicants and carcinogens [104]. For details about sterigmatocystin and chaetoglobsins A, readers are directed to “Description of the Mycotoxins…” section below. These mycotoxins are extremely toxic and potentially fatal to cattle when present as contaminants in feed; Chaetomium extract caused spleen, liver, and kidney toxicity in mice [105-107]. One study isolated 25 secondary metabolites from building materials that are produced by the strains of C. globosum alone including major (chaetoglobosin A, C and F, chaetomugilin D, and chaetoviridin A) and minor (chaetomugilin I, chaetoviridin E, azaphilones, and other chaetoglobosins) mycotoxins [108]. Strains of C. globosum and other species of Chaetomium have been reported to produce many other secondary metabolites (e.g., chetomin, chaetocin, cochliodinol, epipolythiodioxopiperazines, xanthones, anthraquinones, chromones, depsidones, terpenoids, and steroids) [97,108,109].
Chrysonilia/Neurospora
Chrysonilia/Neurospora grows fast to form pink colonies; Neurospora is holomorph of Chrysonilia (http://website.nbm-mnb.ca/mycologywebpages/Moulds/Chrysonilia.html). Both Chrysonilia and Neurospora are found on the soil surface after grassfire in forest. A single case of endophthalmitis (inflammation of the intraocular cavities) with Chrysonilia is reported [110].
Cladosporium
Cladosporium is relatively slow growing powdery or velvety olive-green to olive-brown colonies, grows well between 0-35°C. Some species of Cladosporium infect plants or other mold pathogens; some live on plants without causing infections, and some can cause mycosis of lungs, eyes, skin, and nails in mostly immunocompromised individuals [111]. Cladosporium is the most frequently detected molds found in ~70% of the houses tested [112,113]. Indoors, it is often detected in dirty refrigerators, on moist window frames, paint, paper, fabrics stored under humid conditions, and ventilation systems. The optimal temperature for Cladosporium growth is 18-28°C; however, some species can live below freezing temperatures with the ability to reproduce even on frozen meat [114]. Cladosporium spores are easily airborne and transported over long distances. Cladosporium is a well-known allergen, commonly causes hay fever and asthma. In immunocompromised individuals, Cladosporium may cause corneal infections and mycetoma involving cutaneous and subcutaneous tissue, fascia, bone abscesses, granulomata, and draining sinuses [115].
Coelomycetes
Coelomycetes is a term used for asexual forms of Ascomycota and Basidiomycota (previously known as anamorphs) that produce conidia (mitospores) within fruiting bodies called conidiomata [116]. Coelomycetes grow on plants or other fungi and are ubiquitous in soil, salt and freshwaters, and in sewage [117]. There are reports of increasing cases of cutaneous/subcutaneous and invasive disease, keratitis, and deep tissue infection, especially in immunocompromised individuals [118,119].
Corynespora
Corynespora is a plant pathogen that causes leaf-spotting and rarely causes human infections [120-122]. However, Corynespora has been reported to cause serious subcutaneous infection in humans [122-125].
Curvularia
Curvularia grows rapidly to form white to pinkish gray woolly colonies which turn to olive brown or black upon maturation. Spores of Curvularia are relatively large and often remain in the nose or sinuses of humans following inhalation. Curvularia is found in soil, plant debris, stored grains as well as often indoors – mostly on wooden structures. Curvularia is a plant pathogen [126]. Curvularia is an allergenic and opportunistic pathogen, especially among immunocompromised individuals. Curvularia occasionally causes onychomycosis, mycetoma, keratitis, sinusitis, mycetoma, pneumonia, endocarditis, peritonitis, and cerebral abscess, mostly in immunocompromised individuals but also in healthy individuals [127-130].
Epicoccum
Epicoccum grows rapidly at 37°C (with capability to grow from –3°C to 45°C) producing woolly, cottony, or felty yellow, orange, red or pink colonies that turn greenish brown to black with aging. It is occasionally present in dust collected from inside the buildings and frequently found in indoor air. Epicoccum spores survive for extended periods of time in dry weather and grow under optimal conditions. Epicoccum causes skin infection, respiratory tract allergies like rhinitis, sinusitis, and asthma; systemic diseases from Epicoccum are rare [131]. Elevated spores of Epicoccum are known to induce or worsen asthma attacks in children (https://www.inspq.qc.ca/en/moulds/fact-sheets/epicoccum-purpurascens); they cause severe allergies like hypersensitivity, pneumonitis, and allergic fungal sinusitis in 5-7% of global population [131]. Epicoccum produces a wide array of secondary metabolites [132].
Eurotium
Eurotium is the sexual state of Aspergillus containing characteristic whitish to bright yellow spherical fruiting bodies. Aspergillus, when growing for a long period of time on nutrition rich substrate that is conducive for the conversion to sexual phase, produces related Eurotium. It is one of the most frequently found mold constituents found in household dust [131]. It generally grows on substrates low in moisture like stored grains, textiles, leather, and materials coated with resins and lacquers, like furniture. Allergenicity and toxicity of Eurotium closely resemble Aspergillus; Eurotium has not been studied separately from its asexual stage, i.e., Aspergillus. Still species of Eurotium are known to cause opportunistic infections of ears, eyes, skin, mycetoma, asthma, bronchopulmonary mycosis, cerebral abscess (in one healthy individual) [133,134].
Fusarium
Fusarium grows rapidly to form white, tan, cream, yellow, salmon, cinnamon, pink, red, violet, or purple colonies. Fusarium is found in soil, plants, and grains. Its growth requires very wet conditions and normally does not appear in air samples. Fusarium produces many bioactive and volatile metabolites; some produce strong musty smell in water-damaged building materials. Fusarium is allergenic and often causes eye, skin, and nail infections; it readily infects burn victims.
Species of Fusarium produce three of the most important classes of mycotoxins: trichothecenes (nivalenol, deoxynivalenol, T-2 toxin, fusarenon-X, and related compounds), fumonisins (B1, B2, B3 and B4 with B1 and B2 are classified as possible human carcinogens), and zearalenones and four less studied but emerging mycotoxins: fusaproliferin, beauvericin, enniatins, and moniliformin [135-137]. Other potentially important secondary metabolites not exclusively produced by Fusarium include: acuminatum, butenolide, culmorin, cyclonerodiol, equisetin, fusaprolieferins, fusarochromanones, fusaric acids, fusarins, napthoquinones, sambutoxin, and wortmannin [138].
Fumonisins are associated with esophageal cancer in humans from ingestion of Fusarium contaminated corn and classified as Group 2B carcinogens (possibly carcinogenic to humans) [135]. Fumonisins are poorly absorbed with oral bioavailability of <5% and the absorbed fraction is rapidly distributed and eliminated in bile following glucuronidation; elimination half-life (t½) of fumonisins has been reported 0.3 to 3.2 h [139-140]. Fumonisins cause liver and kidney toxicity and cancer in rodents; they are also neurotoxic. More recently, fumonisins have also been implicated in birth defects (neural tube) in humans and animals. Fumonisins produce these effects by inhibiting activity of ceramide synthase, which converts sphinganine to sphingosine resulting in increased tissue concentration of sphinganine, thus affecting cellular growth, differentiation, and cell communication resulting in toxicity and carcinogenicity [75,141]. To ensure safety, a maximum tolerable daily intake (TDI) for all fumonisins was set at 2 μg/kg [142] and for FB1 and FB2 at 1 μg/kg [143]. For details about trichothecenes and zearalenones, readers are directed to “Description of the Mycotoxins…” section below.
Hyphal fragments
Hyphal fragments or mycelia are fruiting structures of molds. They normally settle quickly and therefore are found in indoor dust; they are also found in outdoor air. Their presence in indoor air, especially in large quantities, is suggestive of active mold growth. Hyphal fragments may cause allergic reactions in some individuals.
Insect fragment
Insect fragment, presence of large quantities of carpet beetle larvae hair, fly hair, and insect scale are indicative of enough moisture to support insect and mold growth even if not visible. Insect scales and hair can be highly allergenic, causing itching, redness, and irritation; they can also be contact and/or respiratory sensitizer resulting in severe allergic reactions involving immune system, such as swelling and difficulty breathing.
Mucor
Mucor is a member of the class of fungi known as Zygomycete (see below for details about Zygomycete) which grows rapidly to dark gray or light olive gray colonies. Mucor is one of the most quickly invading and spoiling molds for many kinds of stored food products. Mucor is often found in dust of inside buildings, stored grains, hay, and horse manure. High concentrations of Mucor spores are frequently detected in indoor air samples, accumulated dust in HVAC systems, and poorly maintained carpeting. High exposure to Mucor spores (through inhalation, ingestion, surgical and accidental wounds, ears, nose, nails, and eyes) can cause extrinsic allergic alveolitis, a type III allergic response to exposure associated with elevated temperature, flu-like symptoms, general malaise, difficulty breathing, and asthma. In immunocompromised individuals, Mucor can cause severe infections characterized by vascular invasion, thrombosis, infarction, and tissue necrosis (https://library.bustmold.com/mucor/). Mucor can cause mucormycosis (infection mostly of respiratory and central nervous system but may also be of skin, GI tract). Mucormycosis pneumonia is the most dangerous Mucor-related infections usually associated with pulmonary or nose, paranasal sinuses, and brain, with prolonged neutropenia, elevated serum iron in almost always in immunocompromised individual but have also been reported in immunocompetent individuals. The mortality rate of mucormycosis pneumonia is 60% or greater, much higher than many other molds [144]. Mucor infection in healthy individuals is rare [145-147].
Nigrospora
Nigrospora grows rapidly to white woolly colonies turning to gray and eventually black upon maturation. Nigrospora is ubiquitous, especially in warm climates. It grows on decaying plant material and soil; its spores are dispersed by an active discharge mechanism without the aid of wind or rain. It normally does not grow indoors. Nigrospora is allergenic with rare cases of human infection causing allergies of the respiratory tract as well as of skin, nail, and eye, especially in immunocompromised individuals [148-150].
Oidiodendron
Oidiodendron is detected in living and decomposing plants, animals, soil, wood, decomposing human hair, and indoor air and dust samples. At least one species of Oidiodendron has been reported to cause atopic eczema in one individual [151].
Paecilomyces
Paecilomyces is regularly found in soil and dust and less often in air; several species cause food spoilage detected in edible oils, peanuts, margarine, cereals, bread, and meat products. Paecilomyces can also grow indoors on water damaged building materials and is commonly detected in indoor samples. Paecilomyces can grow in the presence of moisture at temperatures ranging from 1°C to 60°C and even can withstand 80-100°C for a brief period of time, up to 15 min [131,152]. Paecilomyces can also grow on creams, lotions, cosmetics, plastics, vinyl and diagnostic materials even when containing antifungal agents [131]. Paecilomyces is an opportunistic pathogen [153] responsible for pulmonary, cutaneous infections, endocarditis, peritonitis, and sinusitis; some species of Paecilomyces cause pneumonia. Paecilomyces causes infections in organ transplant, HIV and immunosuppressed patients and detected in respiratory secretions, tissue biopsies, blood, and isolated from abscesses [154].
Particulate matters/fibers
Depending on the size and shape, fibers/particulate matters (airborne particles) can reach and deposit in various regions of the respiratory tract [155]. Larger particles are deposited in the extra thoracic region of the respiratory tract, coarse particles (PM10) in the tracheobronchial region, and the smallest particles (PM2.5) in the pulmonary region. The smallest particles can reach the alveolar region and exchange with blood. Toxicity of the airborne particles depends on their chemical composition and their capacity to produce reactive oxygen species, they may be mutagenic, carcinogenic, or acutely inflammatory, depending on their organic, elemental, and water-solubility characteristics [155].
Papulaspora
Species of Papulaspora have been reported to cause ocular or systemic infection resulting from exposure [156].
Penicillium
Penicillium grows with a velvety, wooly, or cottony texture, colonies grow rapidly to initially white and with time turn to blue green, gray green, olive green, yellow, or pinkish in color. It is normally found in soil, food, cellulose, paint, grains, and compost. Inside buildings, Penicillium is found in wallpaper, carpet, and inside the duct insulation, it is often found inside water damaged buildings [107,157]. Genus Penicillium is comprised of over 300 species and is one of the most frequently detected molds in the world. Spores of Penicillium are easily airborne and inhaled by inhabitants. Many species of Penicillium are known to cause human diseases including skin allergy, keratitis, penicilliosis, mycosis, otomycosis, allergic alveolitis, hay fever, asthma, and hypersensitive pneumonitis in susceptible individuals [158,159]. Long-term exposure can lead to chronic sinusitis. Penicillium exposure can worsen symptoms and lead to health complications in people with immune disorders and/or genetically predisposed to mold toxicity. Penicillium species produce more than 30 different mycotoxins (e.g., citrinin, cyclopiazonic acid, OTA, patulin, penicillic acid, penitrem A, roquefortine, frequentin, palitantin, mycophenolic acid, viomellein, gliotoxin, citreoviridin, and rubratoxin B) [160-162]. For details about citrinin, OTA, mycophenolic acid, and gliotoxin, readers are directed to “Description of the Mycotoxins…” section below.
Pestalotia/Pestalotiopsis
Pestalotia/Pestalotiopsis is a plant pathogen found on plant leaves, stems, twigs, and barks as lesions or gray spots. Some species of Pestalotia/Pestalotiopsis can grow on synthetic polymer found inside many buildings. Pestalotia/Pestalotiopsis has been reported to cause keratitis in an older individual [163]. No additional information about allergenicity, toxicity or adverse health effects of Pestalotia/ Pestalotiopsis is available.
Rhizopus
Rhizopus is often found on bread, fruits, in soil and dust that looks like a dense layer of cotton. Rhizopus is a member of the class of fungi known as Zygomycete (see below for details about Zygomycete). Rhizopus is a fast-growing deep grey to black mold that can grow in a wide range of settings and in harsh conditions [164]. Rhizopus often causes spoilage of food and is pathogenic to humans. It is allergenic, especially to sensitive individuals, causes coughing, wheezing, runny nose; in immunocompromised individuals, it can cause mucormycosis. Rhizopus infection in healthy individuals is rare [145-147].
Periconia
Periconia forms pale to dark brown spores; Periconia is difficult to differentiate from Smuts, Myxomycetes and other molds that produce brown spores [165,166]. It is commonly found outdoors and less indoors; only 1-5% (~0.6%/m3) of total spores usually belong to Periconia [168,169]. Periconia is allergenic and known to cause keratitis [169]. Periconia produces several bioactive compounds (e.g., periconin A, B, C, D, coumarin, benzaldehyde, piperine, taxol) with antibacterial, antifungal, anticancer activities [170-174].
Phaeotrichoconis
Phaeotrichoconis is a plant pathogen found as endophytic fungi on healthy leaves [175]. Species of Phaeotrichoconis are found in Africa, Asia, Australia, North America, and South America [175]. Phaeotrichoconis crotalariae has been reported to cause mycotic keratitis in animals [176].
Pithomyces
Pithomyces produces cottony suede-like fast growing white to cream or olive colonies that turn tan to brown with age. It grows optimally at ~24°C and above 80% relative humidity, mainly on decaying plants, grasses, and soils [177]. Pithomyces may grow on paper, but they are not prolific indoors. Pithomyces is pathogenic, reported to cause sinusitis, peritonitis, onchomycosis, and asthma, especially in immunocompromised individuals [178-181]. One study found Phitomyces more frequently in higher concentrations in homes with asthmatic children than in homes without asthmatic children [19]. Pithomyces produces mycotoxin sporidesmin A which causes liver damage and facial eczema in animals [177].
Pollen
Pollen is plant particles, not mold spores. Pollen is not restricted outdoors, and at least some typically find their way indoors and frequently detected in indoor air samples. Presence of pollens in indoor air when they are not expected in outdoor air is likely indicative of dust and pollen reservoir inside the building such as in a dirty HVAC system. Levels of pollen vary widely, even indoors, with season, wind, weather, temperature, rainfall. Pollen is the most common cause of allergies globally. Pollen often causes runny nose, itchy and/or watery eyes, sore throat, cough, and decreased sense of taste and/or smell, they may also trigger respiratory illness and/or some forms of asthma.
Rust
Rust grows on grass, flowers, trees, and living plant materials, it doesn’t grow indoors without the presence of host plants. It produces red, rusty to orangish spores. Rust causes type I allergic reactions in humans.
Scopulariopsis
Scopulariopsis grows moderately rapidly at 25°C to white velvety to powdery textured colonies which become light brown to tan as colonies mature. In indoors, it is found on drywalls, cellulose board, wallpaper, wood, mattress dust, carpets, shoes, and wood pulp [182-184]. It is commonly found indoors. Certain species of Scopulariopsis may cause nail infection, pulmonary mycoses, infection of soft tissues, bones and rarely pneumonia, keratomycosis, otitis, and septicemia, especially in immunocompromised individuals [185,186]. Many species of Scopulariopsis can release garlicky smelling arsine gas from the growing substrate that contains arsenic [187].
Smuts
Smuts form black powdery spore masses resembling soot, and therefore, called smuts. They are indistinguishable from Myxomycetes and Periconia under microscope at 600x magnification. Smuts are plant pathogens requiring living host (e.g., corn, grass, weeds, flowering plants, and other fungi) to complete their life cycle and distributed by wind [188,189]. They are therefore usually not found growing indoors. Smuts are type I allergens in immunocompromised individuals or those who work or live near farms infested with smuts causing asthma, bronchitis, hay fever, hypersensitivity pneumonitis [190-193].
Sporidesmium
Sporidesmium infects dead plants in pasture. Sporidesmium produces sporidesmins (a potent hepatotoxin) that causes facial eczema in sheep and cattle [194].
Stachybotrys
Stachybotrys rapidly grow to produce cottony white colonies that turn to dark green and black upon maturation. Stachybotrys is not commonly found outdoors. Indoors, it flourishes on water damaged cellulose rich materials such as drywalls, ceiling tiles, cellulose-containing insulation, and wallpaper and is commonly associated with a multitude of illnesses. Stachybotrys produces many mycotoxins like trichothecenes (e.g., Satratoxin F, G, H, Isosatratoxin F, Roridin A, E, H, L-2, Verrucarin A, J). Stachybotrys exposure has been reported to cause debilitating respiratory symptoms, including, pathological changes in the lungs at even low concentrations [195-197]. Allergic sensitization, inflammation, and cytotoxicity of the respiratory tracts of animals have been reported from the exposure to biotoxins of S. chartarum [197-201]. S. chartarum has been linked with infant pulmonary hemosiderosis at six locations (Cleveland, Texas, Kansas City, Belgium, and Quebec) [9,198,202,203]. For details about trichothecenes, readers are directed to “Description of the Mycotoxins…” section below.
Stemphylium
Stemphylium grows rapidly forming velvety to cottony gray, brown, or brownish-black colonies. Stemphylium grows in soil, wood, and decaying vegetation; some species grow on leaves. Stemphylium is a plant pathogen. Stemphylium rarely grows indoors, however, it is detected in dust that is tracked indoors with foot traffic. Stemphylium is one of the most important fungal allergens in the world causing type I allergies that include rhinitis and asthma in children, and angioedema, conjunctivitis, allergic sinusitis, and bronchopulmonary mycosis in sensitive individuals [204; https://newtonlaboratory.com/mold/stemphylium/].
Syncephalastrum
Syncephalastrum belongs to the class Zygomycetes and order Mucorale. Syncephalastrum is often responsible for opportunistic fungal infections in immunocompromised individuals [205,206]. Syncephalastrum usually causes skin and nail infection [207], there have been reports of mucormycosis in immunocompromised individuals [208] with potentially fatal outcomes [206].
Tetraploa
Tetraploa colonies are brownish in color. Tetraploa grows at the base of leaves and stems just above the soil on many plants and trees. It has been reported to cause keratitis and subcutaneous infection [209-211].
Torula
Torula forms dark brown to black velvety colonies [212,213]. It grows on soils, dead wood, leaves, food, hay, textiles, and is found in the air and frequently detected, in small amounts, in indoor air and sometimes outdoors [214-218]. Indoors, Torula grows on cellulose-based materials. Torula causes type I allergies and may cause hay fever and asthma. Torula produces several bioactive secondary metabolites [219-221].
Triadelphia
Triadelphia is found on rotting wood or other plant materials, often submerged in water except for a few species known to be opportunistic human pathogens isolated from clinical samples [222-224]. Triadelphia grows slowly forming velvety colonies with white tufts, starting as uncolored and later becoming greenish grey to dark brown/grey, and finally to brown/black with whitish margins and abundant sporulation; colonies grow best around 30°C. Infections occur mostly in immunocompromised individuals including those with diabetes, or those on chemotherapy and may involve lungs and brain [223].
Trichoderma
Trichoderma grows fast at 25–30°C, some species grow well at 45°C to initially transparent to white colonies which turn to compact or loose clusters of green, yellow, or white in color. Trichoderma is frequently found in soil, decaying dead trees, pine needles, paper, and inside buildings; it often grows on other fungi. Spores of Trichoderma are spread through air. Trichoderma is an opportunistic pathogen that causes allergies, sinusitis, brain abscess, liver infection, stomatitis, hypersensitive pneumonitis, skin infections and disseminated infections, mostly in immunocompromised and organ transplant recipients [225,226]. Infections caused by Trichoderma are rare, however increasing. Trichoderma is associated with hyalohyphomycosis and nosocomial infections traced to contaminated solutions used in hospitals. Several species of Trichoderma produce mycotoxins like trilongins, trichothecenes, and gliotoxin [227,228]. Trilongins block potassium and sodium ion channels and can affect the heart, lungs, and nervous system [227]. Gliotoxin affects the immune system and inhibits phagocytosis and acts as an immunosuppressor [228]. For details about trichothecenes, gliotoxin, readers are directed to “Description of the Mycotoxins…” section below.
Trichothecium
Trichothecium is widely distributed and found on decaying vegetation, foodstuffs, and in soil. It forms powdery colonies, initially white and later turns pale pink to peach in color [229]. Several secondary metabolites including trichothecene (first isolated and named after this mold) are produced by Trichothecium [229]. For details about trichothecenes, readers are directed to “Description of the Mycotoxins…” section below.
Unidentifiable spores
Unidentifiable spores are considered allergenic.
Wallemia
Wallemia is found in soil, on fruits, dry foods, dairy products, textiles, and hay; it also grows on materials with high sugar and salt content like sugary foods and salted meats [230-232]. It grows on materials with low water activity [131]. Wallemia is commonly detected in dust collected from inside buildings [131]. Wallemia is allergenic and known to cause rare infections both in healthy and immunocompromised individuals [230,233].
Yeast
Yeast is found worldwide in varied natural habitats. It is present on the skin and in the GI tracts, where yeast may act as parasites or have symbiotic relationship with the host. Colonies of yeast grow rapidly, they may appear smooth and glabrous, pasty, moist, or dry and most are white to cream in color, but some may be tan, pinkish, or orange in color. The most common fungal infections in humans are yeast infections. Yeast infections range from localized cutaneous or mucocutaneous lesions, to fungemia or systemic mycoses. Some yeasts are also allergenic and multiple exposure may lead to hypersensitivity. Additionally, yeasts may be allergenic to susceptible individuals at sufficient levels.
Zygomycetes
Zygomycetes is a fast growing mold, commonly found in soil or on decaying plants or animal material. Zygomycetes often overgrow and/or inhibits the growth of other molds growing nearby. Spores of Zygomycetes are transmitted by wind and infection occurs through inhalation, damaged skin, and/or ingestion. Species of Zygomycetes (e.g., Rhizopus, Mucor) cause infections and disease, called zygomycosis [234], generally in immunocompromised individuals [235-237]. Zygomycosis rarely occurs in normal individuals. Risk factors for zygomycosis are diabetes mellitus, neutropenia, sustained immunosuppressive therapy, chronic prednisone use, iron chelation therapy, broad-spectrum antibiotic use, severe malnutrition, and breach in the integrity of primary cutaneous barrier such as trauma, surgical wounds, needle sticks, or burns. The most common are rhinocerebral, pulmonary, GI, cutaneous, and disseminated zygomycosis as well as allergies [235-237]. Some of the species of Zygomycetes cause angioinvasive disease that often leads to thrombosis, infarction of involved tissues, and tissue destruction; diseases are mediated by several proteases, lipases, and mycotoxins [147].
Commonly Detected Bacteria in Collected Samples
From suitable places inside buildings, suspected ideal for bacterial growth, samples are collected and placed into sterile containers and sent to microbiology laboratory for the identification and enumeration of culturable bacteria (i.e., colony forming units or CFU/mL). Level of endotoxins produced by the bacteria is also determined and reported. As the focus of this paper is mold and mycotoxins, we are only presenting a list of bacteria and endotoxins in (Table 3) for completeness. These are detected inside of even one out of over 800 buildings sampled by the Mold Case Consulting in the last four years without any further discussion. For details, see [24].
|
Commonly Detected Bacterial Species in Samples Collected from Inside the Buildings and Their Pathogenicity |
|
||||
|
Species |
Path |
Species |
Path |
Species |
Path |
|
Achromobacter sp. |
Y |
Dermacoccus sp. |
Y |
Proteus mirabilis |
Y |
|
Acidovorax sp. |
Y |
Elizabethkingia miricola |
Y |
Providencia retigeri |
Y |
|
Acinetobacter sp. |
Y |
Enterobacter sp. |
Y |
Pseudoescherichia vulneris |
Y |
|
A. calcoaceticus |
Y |
Enterococcus casseliflavus |
Y |
Pseudomonas sp. |
Y |
|
A. johnsonii |
Y |
E. faecalis |
Y |
P. maltophilia |
Y |
|
A. junii |
Y |
Escherichia coli |
Y |
P. aeruginosa |
Y |
|
A. Iwoffii |
Y |
E. hermannii |
Y |
P. fluorescens |
Y |
|
A. radioresistens |
Y |
Ewingella americana |
Y |
P. luteola |
Y |
|
A. schindleri |
Y |
Exiguobacterium acetylicum |
Y |
P. mendocina |
Y |
|
A. ursingii |
Y |
Flavobacterium mizutati |
Y |
P. mosselii |
Y |
|
Aerococcus viridians |
Y |
Gluconacetobacter liquefaciens |
Y |
P. oleovorans |
Y |
|
Aeromonas sp. |
Y |
Gram negative rod |
Y |
P. oryzihabitans |
Y |
|
Alcaligenes faecalis |
Y |
Gram positive rod |
Y |
P. putida |
Y |
|
Alicyclobacillus sp. |
N |
Herbaspirillum huttiens |
Y |
P. rhodesiae |
N |
|
Arthrobacter sp. |
Y |
Hydrogenophaga taeniospiralis |
N |
P. stutzeri |
Y |
|
Bacillus sp. |
Y |
Janibacter melonis |
Y |
Pseudoxanthomonas mexicana |
Y |
|
B. cereus |
Y |
Klebsiella sp. |
Y |
Psychrobacter sp. |
Y |
|
B. circulans |
Y |
K. oxytoca |
Y |
P. faecalis |
Y |
|
B. flexus |
NK |
K. pneumoniae |
Y |
P. phenylpyruvicus |
Y |
|
B. fusiformis |
Y |
Kocuria sp. |
Y |
Ralstonia pickettii |
Y |
|
B. megaterium |
Y |
Lactobacillus sp. |
Y |
Raoultella ornithinolytica |
Y |
|
B. pumilus |
Y |
Lactococcus lactis |
Y |
R. terrigena |
Y |
|
B. simplex |
Y |
Leclercia adecarboxylata |
Y |
Rhizobium radiobacter |
Y |
|
B. subtilis |
Y |
Leifsonia aquatica |
Y |
R. rhizogenes |
N |
|
Bergeyella zoohelcum |
Y |
Lelliottia amnigena |
Y |
Rhodobacter sphaeroides |
N |
|
Brachybacterium nesterenkovii |
Y |
Lysinibacillus fusiformis |
Y |
Rhodococcus erythropolis |
Y |
|
Brevibacillus parabrevis |
Y |
L. sphaericus |
N |
Roseomonas sp. |
Y |
|
Brevibacterium casei |
Y |
Macrococcus caseolyticus |
Y |
Rothia mucilaginosa |
Y |
|
B. iodimum |
Y |
Methylobacterium radiotolerans |
Y |
Serratia marcescens |
Y |
|
Brevundimonas dimimuta |
Y |
Microbacterium sp. |
Y |
Shewanella putrefaciens |
Y |
|
B. vesicularis |
Y |
M. arborescens |
Y |
Siccibacter turicensis |
Y |
|
Burkholderia sp. |
Y |
M. aurum |
Y |
Solibacillus silvestris |
N |
|
B. cenocepacia |
Y |
M. hominis |
Y |
Sphingobacterium sp. |
Y |
|
B. gladioli |
Y |
M. oxydans |
Y |
S. multivorum |
Y |
|
Buttinxella agrestis |
Y |
M. paraoxydans |
Y |
S. spiritivorum |
Y |
|
Cellulomonas sp. |
Y |
M. resistens |
Y |
Sphingobium sp. |
Y |
|
Cellulosimicrobium cellulans |
Y |
M. terrae |
Y |
Sphingomonas sp. |
Y |
|
Chitinophaga arvensicola |
Y |
Micrococcus luteus |
Y |
S. paucimobilis |
Y |
|
Chryseobacterium gleum |
Y |
M. lylae |
Y |
Sphingopyxis sp. |
N |
|
C. balustinmum |
Y |
Moraxella osloensis |
Y |
Staphylococcus sp. |
Y |
|
C. indologenes |
Y |
Morganella morganii |
Y |
S. epidermidis |
Y |
|
Citrobacter sp. |
Y |
Mycobacterium smegmatis |
N |
S. heamolyticus |
Y |
|
C. amalonaticus |
Y |
Nesterenkonia halobia |
Y |
S. pasteuri |
Y |
|
C. braakii |
Y |
Ochrobactrum anthropi |
Y |
S. saprophyticus |
Y |
|
C. freundii |
Y |
O. intermedium |
Y |
S. simulans |
Y |
|
C. koseri |
Y |
Oerskovia sp. |
Y |
S. warneri |
Y |
|
Coliform bacteria |
Y |
Okibacterium fritillariae |
NK |
S. xylosus |
Y |
|
Corynebacterium variabile |
Y |
Paenibacillus sp. |
Y |
Stenotrophomonas maltophilia |
Y |
|
Cupriavidus pauculus |
Y |
Pandoraea promenusa |
Y |
S. rhizophila |
N |
|
Curtobacterium flaccumfaciens |
Y |
Pantoea agglomerans |
Y |
Y Streptococcus pneumoniae |
Y |
|
Delftia acidovorans |
Y |
Paracoccus yeeii |
Y |
Virgibacillus pantothenticus |
Y |
|
Dermabacter hominis |
Y |
Phyllobacterium rubiacearum |
Y |
Xanthomonas sp. |
Y |
|
Path, pathogenicity, Y, yes; N, no; NK, not known. |
|||||
Analysis of Urine for Mycotoxins Produced by Many Molds
Urine (rarely blood, only when warranted) samples are collected from the inhabitant(s) of the buildings in question and analyzed for 11 mycotoxins produced by at least 5 genera of molds (Table 4). These are considered primary molds and mycotoxins of concern for human health. For details of the methods, see [24].
|
Molds & Their Mycotoxins in Urine* |
|
|
AspergiIlus Aflatoxin-M1 Gliotoxin Chaetomi globosin A Cliaetoglobosin A Fusarium Enniatin B Zearalenone |
Multiple Mold SÞecies** Citrinin (Dihydrocitrinone DHC) Penicillium Sterigmatocystin Mycophenolic Acid Stachybotrys Roridin E Venucarin A |
|
*Sometimes also analyzed in blood. ** Mostly by Aspergillus, Penicillium, and Monascus sp. |
|
Mycotoxins consist of several hundred identified toxic compounds that are naturally produced by certain molds [23]; only those which are commonly detected in occupants with potential toxicity are mentioned here. According to WHO [23], mycotoxins can cause a variety of adverse health effects ranging from acute poisoning to long-term effects such as immune dysfunction and cancer, posing a serious health threat to both humans and animals [238,239]. Based on the adverse health effects, aflatoxin, fumonisins, trichothecenes, OTA, zearalenones, and patulin are recognized as the most important mycotoxins [240]. The International Agency for Research on Cancer (IARC) has classified several mycotoxins (e.g., aflatoxin B1, aflatoxin B2, aflatoxin G1, and aflatoxin G2) as Group 1 (known) human carcinogen and several (OTA, fumonisin B1, and fumonisin B2, aflatoxin M1) as Group 2B (possibly) human carcinogen [241,242]. The most frequently detected mycotoxins were OTA, CTN, and MPA followed by gliotoxin, and aflatoxin M1 in samples collected from over 2000 occupants from across the United States who lived in over 800 suspected mold-infested buildings.
Individuals hypersensitive to mycotoxin are at higher risk of developing toxicities against aforementioned agents. Symptoms of mycotoxin poisoning depend on the type of mycotoxin involved, dose, frequency, and duration of exposure as well as gender, health, and age of the exposed individual. Exposure to mycotoxins can also increase the vulnerability to microbial diseases [25,243,244]. Mycotoxins have been reported to impair barrier function of epithelial cells, including cells that make blood brain barrier, resulting in inflammatory changes and neurological effects in healthy individuals and exacerbation of many inflammatory conditions, like pneumonia, chronic fatigue [1,16,25,245-248].
Mycotoxins are easily absorbed following inhalation, dermal, and oral routes and reported to cause innate immune activation, neural, cognitive, and emotional dysfunction [21,249]. There is now mounting evidence, both from animal and human (epidemiological) studies, that exposure to molds and mycotoxins in indoor settings can cause adverse health effects [250].
Description of the Mycotoxins Found in Urine (rarely blood is also analyzed)
Aflatoxin
Aflatoxins are among the most poisonous mycotoxins that are produced by certain species of Aspergillus, mainly A. flavus, A. parasiticus and A. nomius [23,251,252]. Out of over groups of 20 known aflatoxins, B1 (most potent), B2, G1, and G2 are the four major ones for toxicity [253]. Aflatoxin M1 is the hydroxylated metabolite of B1 formed during fermentation by A. parasiticus and produced during in vivo metabolism and excreted via urine (major elimination route) and milk (minor elimination route); they have also been detected in human breast milk, infant formula, cow’s milk, and dairy products [254-258].
Aflatoxins cause hepatotoxicity, immunotoxicity, developmental toxicity, and are mutagens, thus are carcinogens. According to the European Food Safety Authority (EFSA), even exposure of as low as 1 ng/kg/day can increase the risk of developing liver cancer [259]. Liver toxicity of aflatoxin is considered a crucial issue; aflatoxicosis, characterized by liver damage, with acute symptoms of edema, hepatitis, hemorrhagic necrosis of liver and profound lethargy, while chronic effects include immune suppression, growth retardation, and cancer [260-268]. Ingestion of as little as 2 mg/day of aflatoxin for a month can lead to acute hepatitis and death [260,263,270].
Immunotoxicity of aflatoxins in humans is characterized by downregulation of interleukin-4 (IL-4) and upregulation of tumor necrosis factor-alpha (TNFα) secretion; Aflatoxin B1 is a known suppresser of immunity by decreasing protective effects of vaccines [271-273]. Aflatoxins can also enter developing fetus in humans by crossing placenta and have been detected in cord blood [274-278]. Increased preterm birth and late-term miscarriages have been reported from maternal exposure to aflatoxins [279]. Aflatoxin B1 and M1 are classified as Group 1 and Group 2B carcinogens, respectively by the IARC [78,79,280]. Carcinogenicity of aflatoxin B1 is partly due to its ability to cause DNA damage and mutation [281-283]; they have also been reported to cross blood brain barrier causing damage to mitochondrial DNA of brain cells [284,285].
The most common route of entry of aflatoxin into the human body is ingestion followed by inhalation. Once absorbed, aflatoxins are metabolized by microsomal mixed-function oxidase, cytochrome P450 3A4 and 1A2, mostly in the liver, to form reactive epoxide intermediates which are responsible for DNA mutation and cellular dysregulation, following depletion of glutathione, through binding reactive metabolites to proteins, RNA, and DNA [79,82,286,287]. The absorbed aflatoxins are relatively rapidly excreted mainly through bile. In urine, aflatoxin B1 is excreted as aflatoxin M1. Elimination t½ of aflatoxin M1 in humans is ~8 h [288]; elimination t½ of aflatoxin-albumin adduct from blood in humans has been reported to be 30-60 days [267].
Chaetoglobosin A
Chaetoglobosin A is produced by molds (e.g., Chaetomium, Penicillium), primarily of the genus Chaetomium [289,290]; for details of secondary metabolites produced by Chaetomium, see section on Chaetomium above. Chaetoglobosin A belongs to cytochalasans, a highly diversified group of fungal secondary metabolites, which display a broad range of bioactive properties. Cytochalasans have been shown to act as phytoalexins, hamper cholesterol biosynthesis, act as an immunosuppressor at high doses, interfere with glucose transport by human erythrocyte membranes, inhibit secretion of thyroid hormones, inhibit postmitotic cytoplasmic cleavage of HeLa cells, inhibit cell movement, inhibit ciliary beating in chicken tracheal organ culture [96,103,291]. Cytochalasans also facilitate fungal virulence (https://metacyc.org/META/NEW-IMAGE?type=PATHWAY&object=PWY-7612). Chaetoglobosin A has been reported to be highly acutely toxic to rats when administered subcutaneously killing all of them at the lowest dose of 2 mg/kg tested; LD50 in mice was ~7 mg/kg (male) and ~18 mg/kg (female) with 5 mg/kg dose causing visceral congestion, necrosis of the thymus and spleen tissues and degeneration of spermatocytes in testes [103]. Oral doses were far less toxic (>400 mg/kg), likely due to low oral absorption and/or first-pass metabolism [103]. A 2-week dosing of 30 ppm chaetoglobosin A to mice in diet (~6 mg/kg/day) caused liver injuries, bone marrow aplasia, and atrophy of lymphatic tissue [109]. Reproductive and developmental toxicities (increased resorptions, decreased fetal body weight, and fetal survivability) have been reported in mice dosed with either ~2 or ~6 mg/kg/day chaetoglobosin A from gestational days 0-18 [109]. A slight increase in mutation frequency was observed in a mouse mammary cancer cell line [292].
Citrinin
Mycotoxin citrinin (CTN) is produced by species of many molds including Penicillium, Aspergillus and Monascus [25,293]. CTN has some antibiotic properties against gram-positive bacteria, but it has high nephrotoxicity and therefore, never used as a drug. Although, the major target organ for CTN toxicity is kidney, it is also hepatotoxic, embryocidal, fetotoxic, immunotoxic; cause toxicity to bone marrow and modulate immune system [294-303]. Kidney damage by CTN is characterized by enlarged kidney, hydropic degeneration, loss of brush border, and pyknotic nuclei in the proximal tubules [304]. CTN inhibits key enzymes in cholesterol biosynthesis, reducing concentration of serum testosterone and causes hypocholesterolemia [305]. Swelling of the kidneys and acute tubular necrosis was observed in animals dosed with acutely toxic doses (LD50 oral and subcutaneous = 50 and 35 mg/kg) of CTN [303,304,306-309]. The TDI of CTN is set to 0.2 μg/kg by the European Food Safety Authority and Deutsche Forschungsgemeinschaft [310-312].
Following absorption, CTN is extensively metabolized to dihydrocitrinone (DHC) and excreted in urine as the main metabolite, along with parent CTN [313-314]. DHC is less toxic than CTN and the presence of DHC in urine or blood is used as a biomarker of exposure to CTN [315,316]. In human volunteers, cumulative (CTN+DHC) urinary excretion over 24 h has been reported to between 33 and 71% with urinary elimination t½ of ~7 h for CTN and ~9 h for DHC; plasma elimination t½ of CTN is ~9 h [314].
Enniatin B
Enniatins (ENNs) are produced by several Fusarium species, 29 of them are known [317]; the most important ENNs is ENN B based on incidence and observance. ENNs inhibit acyl-CoA: cholesterol acyl transferase activity resulting in oxidative stress [318,319]. ENNs are cytotoxic through the disruption of normal physiological concentrations of Ca2+, Na+, K+ across membranes by disrupting ionic selectivity, which is debilitating for mitochondrial membranes causing uncoupling of oxidative phosphorylation [320,321]. The non-functioning of mitochondria leads to cell cycle disruption and apoptotic cell death [319,322-329].
ENN B alters cellular energy metabolism and reduces cell proliferation, increases apoptosis, and necrotic cell death; alteration in energy metabolism is by effecting mitochondrial membrane permeability transition and hence its function [330]. ENN B inhibits multidrug resistance associated protein-1 (ABCG2) and P-glycoprotein (ABCB1) efflux pumps [331-333]. Cytotoxicity is observed at low micromolar concentrations in animal cell lines (i.e., mouse macrophages, porcine kidney cells, Spodoptera frugiperda cell line, [SF-9 cells]), and reduce motility of boar spermatozoa [334]. ENN B is an endocrine disruptive chemical, produces adrenal toxicity [335]; toxicity of ENN B has been reported to enhance in the presence of other ENNs or other mycotoxins [329]. Once absorbed, ENN B is detected in all tissues and in blood with the highest concentrations in adipose tissue and liver indicating its bioaccumulation in lipophilic organs [336]. Elimination t½ of ENN B has been reported to be ~5 h in mice [337] and ~1.6 h in pigs [338].
Gliotoxin
Gliotoxin is produced by several fungal species belonging to genus Aspergillus (e.g., A. flavus, A. fumigatus, A. niger, A. terreus), Eurotium (e.g., E. chevalieri, E. Rubrum), Neosartorya (e.g., N. pseudofischeri), Trichoderma (e.g., T. virens), and some species of Penicillium, Acremonium and Alternaria; spores of A. fumigatus is the most clinically relevant source of gliotoxin [339-344]. Gliotoxin is an epipolythiodioxopiperazine (ETP) derivative that exerts profound immunosuppressive effects by inhibiting cellular functions of B, and T lymphocytes, macrophages, and apoptosis of immune cells [345-348]. The presence of a disulfide bridge in ETP makes gliotoxin to inactivate proteins at high concentrations by covalently binding with thiol groups of proteins and generating reactive oxygen species by redox cycling [349,350]. At relatively low concentrations (IC50 of 50–100 nM), gliotoxin selectively inhibits activation of nuclear factor-kappa B (NF-κB), preventing induction of intercellular adhesion molecule 1 (ICAM-1) demonstrated using ICAM-1 promoter-reporter luciferase gene and determing the reporter activity by tumor necrosis factor-alpha (TNFα), interleukin -1 (IL-1), and phorbol myristate acetate (PMA), all of them are NF-κB activators [351].
Gliotoxin suppresses phagocytosis by interfering with phosphatidylinositol 3,4,5-trisphosphate production which impairs the ability of macrophages to recognize and destroy invading pathogens [352]. Exposure to gliotoxin is hypothesized to result in colonization and virulence of A. fumigatus [348,353-355]. In mice, administration of gliotoxin caused immunosuppression resulting in the establishment of invasive aspergillosis with A. fumigatus; in humans, gliotoxin is known to slow ciliary action and damage epithelium of the respiratory tract [348,353-355]. Gliotoxin can lead to invasive aspergillosis, caused by the opportunistic mold A. fumigatus, that typically reside in the pulmonary system, the ears, the eyes, or the nails; gliotoxin is detected in serum of patients with invasive aspergillus [356]. Aspergillosis is a devastating disease for immunocompromised individuals (e.g., organ transplant recipients, those with AIDS, cancer, receiving bone marrow transplant, patients undergoing chemotherapy) caused by gliotoxin frequently resulted in renal failure with mortality rate of ~90% [349-351,357-360]. A. fumigatus is also frequently detected in sputum of patients with chronic respiratory diseases like cystic fibrosis [361,362].
Mycophenolic acid
Mycophenolic acid (MPA) is produced by many species of Penicillium, it is a potent immunosuppressant often used to prevent rejection in renal transplant patients [363,364]. MPA is a selective and non-competitive inhibitor of the inosine monophosphate dehydrogenases (IMPDH), an enzyme involved in de novo biosynthesis of guanosine nucleotide, the only pathway of purines synthesis in B and T lymphocytes [365]. Inhibition of IMPDH blocks cell proliferation by blocking DNA and RNA biosynthesis [364,366]. Inhibition of proliferation of both B and T-cells suppresses lymphocytes that identify mold toxins and increases risk of opportunistic infections [367-369]. Following oral administration, MPA is rapidly absorbed from the small intestine reaching maximum blood concentration in 60 to 90 min. with an average oral bioavailability of ~94% in healthy human volunteers [370]. MPA is rapidly metabolized to an inactive glucuronide conjugate by isoforms of the UDP-glucuronosyltransferases in the liver, kidney, and intestine [371,372]. At least three minor metabolites of MPA have also been identified in humans [373].
Plasma elimination t½ of MPA in healthy volunteers is 17.9 h after oral administration (https://go.drugbank.com/drugs/DB01024). Between 8 and 12 h after oral administration, an average of 37% of people display a secondary peak of MPA in plasma, representing absorption of the intestinal bacterial deglucuronidated metabolites of MPA through enterohepatic circulation accounting for up to 40-60% of the total circulating dose. Metabolites of MPA is predominantly eliminated in urine (~93% of the dose), fecal elimination accounts for ~6% of the dose [374; https://go.drugbank.com/drugs/DB01024].
Human leukocyte antigen (HLA) genes are a family of genes on the human chromosome 6 responsible for making a group of cell-surface proteins, i.e., HLA complex, which are essential for removing either infected cells or producing antibodies in response to invading/foreign antigens [375]. HLA genes have many alleles which play key role in presenting endogenous and exogenous peptides to T-cells for fine-tuning of the adaptive immune response; mutations at the HLA gene alleles result in slow response to eliminate MPA from the body [376-378]. People with genetic predisposition at the HLA genes have shown to eliminate MPA extremely slowly from their body (~213-fold slower with the t½ of ~160 days instead of ~0.75 day in individuals without genetic predisposition at the HLA genes) [24].
Ochratoxin A
Ochratoxins are produced by species of Eurotium, Aspergillus, Fusarium and Penicillium. There are three generally recognized ochratoxins, designated A, B and C. Ochratoxin A (OTA) is the most toxic, followed by OTB and OTC. Kidney is the primary target organ of OTA toxicity through lysis of tubular cells [379]. OTA is nephrotoxic to every animal species tested to date and is most likely toxic to humans; elimination of OTA is the slowest in humans than any other species examined [http://www.ictm.com/Reports/ereport_Vol3No3.pdf; 380]. Endemic Balkan nephropathy, a progressive chronic nephritis in people living in areas bordering Danube River, is speculated to be caused by ochratoxins contaminated food as evidenced by the presence of ochratoxins in serum of families with endemic Balkan nephropathy and urinary tract tumors than in unaffected families [381-384]. In addition to being a nephrotoxin, OTA is also hepatotoxic, immune suppressant, potent teratogen, mutagen, and carcinogen [385,386]. OAT has been placed under cancer category 2B, possible human carcinogen, by the IARC [386].
Mode of toxicity of OTA is not completely understood and appears to be quite complex. Inhibition of energy production (e.g., mitochondrial ATPs), inhibition of the synthesis of proteins (e.g., enzymes that synthesize phenylalanine-tRNA, phenylalanyl-tRNA synthetase), stimulation of lipid peroxidation, induction of oxidative stress, DNA adducts formation, apoptosis, cellular necrosis, and cell cycle arrest are possible reasons of OTA’s toxicity [25,74,80,369,387-396].
Following absorption, OTA is distributed at a high concentration in the kidney, the major target organ [397]; OTA has also been reported to cross placenta and found twice as high in fetal than maternal serum in swine and humans [398]. OTA remains highly bound to plasma proteins (99.9% of the circulating OTA remains protein bound with highest binding affinity to human serum albumin), oral bioavailability is between 40 and 60% in animals and ~93% in humans [396,399-401]. Based on lipophilicity and high blood partition of OTA and lungs being highly perfused organ, high absorption of OTA is also expected from the lungs following inhalation exposure. OTA is poorly metabolized and slowly excreted with a plasma t½ of ~6 days in rats, 19-21 days in monkeys, and ~36 days in humans; elimination occurs in the form of parent OTA and following hydrolysis of the peptide bond, presumably by carboxypeptidases produced by the intestinal microflora [288,394,401-404].
Based on the lowest observed adverse effect level (LOAEL) of 8 μg/kg/day in pigs that caused renal malfunction in a dose-response study [405], regulatory agencies have set TDI of OTA between 3 and ~17 ng/kg/day, 4 ng/kg/day intake is considered with negligible cancer risk [406-413].
Roridin E
Roridin E is a trichothecene produced by various species of Fusarium, Myrothecium and Stachybotrys. Roridin E can cause respiratory and olfactory toxicity as many other trichothecenes, it may also disrupt DNA, RNA synthesis, and inhibits protein biosynthesis by preventing peptidyl transferase activity and are known carcinogen [60,61]. Elimination t½ of roridin E is estimated using quantitative structure activity relationship (QSAR) modeling to be ~8 h in healthy humans (https://www.mycocentral.eu/mycotoxins/719). Disruption of DNA, RNA, and protein biosynthesis impact every cell in the body, cells with the highest rate of mitosis are the most susceptible targets of trichothecene. Even low levels of exposure to trichothecenes can result in immune suppression, neurological issues, endocrine disruption, cardiovascular issues, and GI distress [195,197]. For details about trichothecenes, readers are directed to “trichothecenes” section below.
Sterigmatocystin
Sterigmatocystin is produced by several species of Aspergillus, Bipolaris, Botryotrichum, Humicola and Penicillium with Aspergillus being the main producer of sterigmatocystin [414]. Acute toxicity of sterigmatocystin fall under U.S. EPA category II (i.e., oral LD50 ≤500 mg/kg), LD50 following intraperitoneal dosing to rats and monkeys is 60-85 mg/kg and 32 mg/kg, respectively [415]. Sterigmatocystin has been found to affect immune function [416,417]. Sterigmatocystin has been reported to covalently bind to DNA and forms DNA adducts; sterigmatocystin-DNA adducts have been detected in blood and urine of patients with liver and stomach cancer and with liver cirrhosis [414,418-421]. Sterigmatocystin is mutagenic, teratogenic, and carcinogenic (lung and liver cancer) in experimental animals at doses ranging from 5 ng/kg (subcutaneous) to 3-30 mg/kg (oral) [422-426]. Sterigmatocystin has been reported to generate liver and lung tumors following a single subcutaneous dose of 5 ng/kg to newborn mice and confirmed as a putative causal factor for lung adenocarcinoma in mice [424,425]. Sterigmatocystin has been classified as Group 2B human carcinogen by the IARC [427].
Trichothecenes
Trichothecenes are not measured directly as they are a family of more than 200 mycotoxins, several of the commonly detected mold species indoors produce one or more of trichothecenes (for details, see “Description of Commonly Detected Molds…”, above), therefore, we consider it will be helpful for readers to provide information about the trichothecenes as a group here in addition to the mycotoxins analyzed in urine and/or blood. Trichothecenes are produced by some species of Acremonium, Cephalosporium, Cylindrocarpon, Fusarium, Mycothecium, Phomopsis, Spicellum, Stachybotrys, Trichoderma, Trichothecium, and Verticimonosporium [61,62,136,137,227,229,342, 428-430].
Each trichothecene has a common 12,13-epoxitrichothec-9-ene structure (Figure 1), the epoxy group is highly reactive site of trichothecenes allowing them to cause oxidative damage due to the generation of free radicals [431,432]. Based on the substitution pattern of R, H, OH, O, Acyl groups on 12,13-epoxitrichothec-9-ene, trichothecene are classified into Types A, B, C, and D [433,434]. For Type A trichothecenes, substitution at C-8 is either a hydroxyl group (e.g., neosolaniol), an ester (e.g., T-2 toxin), or no oxygen substitution (e.g., trichodermin, 4,15-diacetoxyscirpenol, and harzianum A). For Type B trichothecenes, substitution at C-8 is a keto (carbonyl) group (e.g., nivalenol, deoxynivalenol, and trichothecin). Type B trichothecenes produced by Fusarium typically have hydroxyl group at C-7; however, this is absent in trichothecenes produced by other genera. Trichothecenes in Type C have an epoxide between C-7/C-8 (e.g., crotocin). Trichothecenes in Type D have an additional ring connecting to C-4 and C-15 positions of the 12,13-epoxitrichothec-9-ene (e.g., roridin A, verrucarin A, satratoxin H) [435]. This classification, however, misses some other structural features like all trichothecenes (Types A and B) produced by Fusarium contain a hydroxyl or an acetyl group at C-3 position and trichothecenes (Types A, B, C and D) produced by Trichoderma, Trichothecium, Myrothecium or Stachybotrys lack oxygen at C-3 position [436-438].
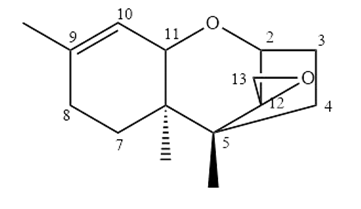
Figure 1. Core structure of 12,13-epoxitrichothec-9-ene to which substitutions of R, H, OH, O, Acyl groups occur producing Types A, B, C, or D trichothecene. Source: Wikimedia Commons, Khayes11 2018, https://commons.wikimedia.org/wiki/File:Tricothecene_Classifications.jpg
{kind=link}
Trichothecenes exert multiorgan effects, e.g., anorexia, loss of weight, growth retardation, immunodeficiency (through decreasing lymphocyte production in hematopoietic organs), cardiovascular alterations, nervous system disorders, decreased reproduction, bone marrow damage, skin toxicity, hemostatic derangements, and alimentary toxic aleukia (mycotoxin-induced conditions like nausea, vomiting, diarrhea, leukopenia, hemorrhaging, skin inflammation, and sometimes death) [60,62,195,197,439-442]. Following dermal or oral exposure, trichothecenes can cause irritation, burning and itching, rash or blisters, and bleeding from skin or intestinal mucosa. Exposure to eyes can cause burning, tearing, pain, conjunctivitis, and blurred vision [441]. Trichothecenes are immunostimulatory at low doses and immunosuppressive at high doses [60,428,441]. Individuals with chronic exposure to the mycotoxins report dermatitis, cough, rhinitis, nose bleeds, burning sensation in the mouth and nasal passage, cold and flu, headache, general malaise, fever, chronic fatigue, irregular menstrual cycle, and premature ovarian failure. Unlike many other mycotoxins, metabolic activation is not needed for trichothecenes to exert their toxicity; they directly react with cellular components through their highly reactive epoxide moiety. Trichothecenes are potent inhibitors of DNA, RNA, and protein syntheses, and mitosis; some of them are also known carcinogen [60,61,244].
Trichothecenes are cytotoxic which is due to their ability to inhibit protein synthesis by binding to ribosomes interfering with the active site of peptidyl transferase at the 3'-end of large 28S ribosomal RNA and inhibit initiation, elongation or termination of protein synthesis causing polyribosome disaggregation. Cells with the highest rate of mitosis, including GI mucosal cells (enterocytes), lymphoid tissues, and bone marrow, are the most susceptible to this effect. Binding to ribosomes also activates signaling downstream resulting in immune response and apoptosis; apoptosis can also be induced through the generation of reactive oxygen species. Additionally, trichothecenes can alter membrane structure resulting in increased lipid peroxidation and inhibition of electron transport in mitochondria [60,441,443-445].
Trichothecenes are easily absorbed following inhalation, dermal, and oral routes of exposure due to their lipophilicity. They are metabolized mainly by cytochrome P-450s and carboxylesterase in liver; other tissues (e.g., kidney, spleen, and intestine) also show some metabolic activity. Trichothecenes are biotransformed into less-toxic metabolites following hydrolysis, hydroxylation, de-epoxidation, and glucuronidation and excreted in urine and feces [440,441].
Verrucarin A
Verrucarin A is a trichothecene produced by Fusarium and Aspergillus. As other trichothecenes, verrucarin is neurotoxic, immunotoxic, cytotoxic, potent protein synthesis inhibitor. Verrucarin A is partially absorbed in dogs following oral administration and excreted with an elimination t½ of about 2 h [446]. Verrucarin is considered among some of the most toxic trichothecenes and more toxic than simple trichothecenes [439,442]. For details about trichothecenes, readers are directed to “trichothecenes” section above.
Zearalenone
Zearalenone is produced by Fusarium molds. Zearalenone is an endocrine disruptor, it is similar in chemical structure to estrogen and therefore, binds with estrogen receptors affecting reproductive organs [447,448]. It also affects the male reproductive system [449]. Zearalenone is also an immunotoxicant and hepatotoxicant [450]. Zearalenone exposure decreases fertility, precocious puberty, change weight of thyroid, adrenal, and pituitary glands, alter progesterone and estradiol levels in serum, cause fibrosis and hyperplasia in the uterus, breast cancer, endometrial carcinoma, and liver damages which may lead to liver cancer [244]. One study found higher levels of zearalenone in urine and serum of autistic children than their healthy siblings [451]. Zearalenone has relatively low acute toxicity with LD50 >2000 mg/kg (EFSA 2011b). EFSA set TDI for zearalenone to 0.25 μg/kg [452-454].
Zearalenone is extensively absorbed and metabolized by oral, dermal, and inhalation routes. Reduction of zearalenone results in formation of α-zearalenol, which is more estrogenic, and β-zearalenol, which is less estrogenic than zearalenone. Efficient glucuronidation of zearalenone in the small intestine and liver significantly reduces the amounts of unconjugated (i.e., receptor-active) parent compound that can reach the circulation. Cytochrome P-450-mediated oxidation produces catechol metabolites that are subject to redox cycling to reactive quinones [288]. Zearalenone is eliminated with an elimination t½ of ~86 h in pigs and <24 h in humans with high oral bioavailability [454,455].
Analysis of Feces for Commensal and Dysbiotic Bacteria and Yeast
Fecal samples are collected from the occupant(s) of the buildings in question and analyzed for bacteria (expected, commensal, and dysbiotic) and yeast (normal and dysbiotic) by culturing in appropriate growth media or via optical microscopy. As the focus of this paper is mold and mycotoxins, we are only presenting a list of commensals and dysbiotic bacteria in (Table 5) for reference only. These are detected in even one out of over 2000 occupants lived in over 800 buildings sampled by the Mold Case Consulting in the last four years without any further discussion. For details of the methods, see [24]. Dysbiosis is an alteration in gut microbiome that increases intestinal permeability increasing the transfer of bacterial endotoxins via portal vein into liver [456]. Endotoxins in liver, activate liver resident macrophages (i.e., Kupffer cells) and promote release of proinflammatory cytokines (e.g., TNFα, IL-1, and IL-6 leading to a cascade of immune responses and inflammation [457-459].
|
Commonly Detected Commensal/Dysbiotic Bacteria in Fecal Samples of Occupant(s) |
||
|
Species |
Species |
Species |
|
Acinetobacter junii |
Kocuria rhizophila |
Staphylococcus aureus |
|
Achromobacter ruhlandii |
K. salsicia |
S. borealis |
|
A. xylosoxidans |
Lactococcus lactis |
S. epidermidis |
|
Bacillus licheniformis |
Lelliottia amnigena |
S. haemolyticus |
|
B. pumilus |
Leuconostoc lactis |
S. lugdunensis |
|
Brevibacterium sp. |
Microbacterium sp. |
S. nepalensis |
|
Citrobacter amalonaticus |
M. maritypicum |
S. pasteuri |
|
C. freundii complex |
Morganella morganii |
S. simulans |
|
Corynebacterium amycolatum |
Pediococcus acidilactici |
Streptococcus agalactiae |
|
C. argentoratense |
P. pentosaceus |
S. anginosus |
|
C. aurimucosum |
Proteus mirabilis |
S. canis |
|
C. falsenii |
P. vulgaris group |
S. constellatus |
|
C. tuberculostearicum |
Providencia alcalifaciens |
S. dysgalactiae |
|
Enterobacter cloacae complex |
P. rettgeri |
S. equinus |
|
Hafnia alvei |
Pseudoglutamicibacter albus |
S. gallolyticus |
|
Klebsiella (Enterobacter) aerogenes |
Pseudomonas aeruginosa |
S. gordonii |
|
Klebsiella/Raoultella complex |
P. chlororaphis group |
S. lutetiensis |
|
K. oxytoca |
P. koreensis |
S. mitis/oralis group |
|
K. pneumoniae |
Rothia (Kocuria) kristinae |
S. mutans |
|
K. variicola |
R. dentocariosa |
S. parasanguinis |
|
Kluyvera cryocrescens |
R. mucilaginosa |
S. salivarius/vestibularis group |
|
K. georgiana |
--- |
--- |
Role of Gut Dysbiosis in Mycotoxin-Related Adverse Health Effects
Gut microbes are good sources of secondary metabolites, such as short chain fatty acids (SCFAs) and lipopolysaccharides, however, in the event of alteration in gut microbiota, gut dysbiosis occurs. In a healthy state, gut microbiota help maintain the basic functions, whereas dysbiosis alters metabolism that can lead to diseases like metabolic syndrome, cardiovascular, GI, neurodegenerative diseases, and cancer [460,461]. Additionally, gut dysbiosis increases the intestinal permeability of bacterial liposaccharides (LPS). Infections with several species of toxic bacteria or occurrence of microbiota dysbiosis, secondary to mycotoxin exposure, likely contribute to several chronic human diseases such as diabetes, colorectal cancer, and degenerative neurological diseases (e.g., Alzheimer’s and Parkinsons’s diseases) [462-464]. Pathogenesis of Alzheimer’s disease (AD) is linked to strong inflammatory responses leading to higher amyloid beta (Aβ) formation [465,466]. The brains of AD patients contain 5–10 times more bacterial LPS than healthy brains [467]. A high cholesterol diet may cause increased sequestration of mycotoxins on the surface of cholesterol leading to increased absorption of various mycotoxins [468]. Additionally, binding of mycotoxins to lipoproteins in human and animal plasma is linked with induction of hypercholesterolemia [469]. Hypercholesterolemia, non-alcoholic fatty liver disease (NAFLD) from metabolic syndrome, diabetes, and inflammation also modifies blood brain barrier (BBB), increasing permeability of mycotoxins across BBB into brain [470]. Higher penetration of mycotoxins to central nervous system due to LPS-induced inflammation and increased blood brain barrier permeability also exacerbate neurological effects of mycotoxins. Additionally, enhanced absorption of lipoprotein-sequestered mycotoxins from intestine will lead to their increased bioavailability to target organs [462,464,469-472].
Globally, inhalation as well as ingestion of mycotoxin, bacterial infections, and gut dysbiosis resulting in increased systemic LPS levels are of major health concern. In developing countries, exposure to mycotoxins and LPS is primarily from ingestion of contaminated food. In developed countries, inhalation exposure from inhabiting mold-infested energy efficient buildings is of more concern, which is predicted to be similar to exposure from diet in developing countries, than exposure through food which is normally significantly less due to strict regulations in developed countries [462,464]. Mycotoxins and LPS once absorbed, either from ingesting from intestine, with high lipids-containing diets, or from inhalation when inhabiting mold-infested building, find their way to target organs. Gut dysbiosis results in systemically increased inflammatory metabolites and cytokines which increase BBB permeability and results in increased transport of immune cells and mediators of neuroinflammation into the brain [470]. Mold exposure to individuals with gut dysbiosis may lead to increased delivery of mycotoxins to the brain from increased BBB permeability. Additionally, enhanced absorption of mycotoxins sequestered in lipids can cause other adverse health effects mentioned above. Therefore, excessive bacterial growth indoors and fat rich diet may be of major concern for mycotoxin exposure, either by ingestion or inhalalation, warranting a closer investigation of LPS and mycotoxin nexus in mycotoxin-exposed individuals.
Risk Assessment of Molds and Mycotoxins
Risk assessment is a process of integrating hazard identification with dose-response and exposure assessment (https://www.epa.gov/risk/conducting-human-health-risk-assessment). The first step in the risk assessment is the identification of hazard, i.e., whether exposure to something of concern can increase the incidence of (specific) adverse health effects and effects, if seen only in experimental animals, are likely to occur in humans. Hazard identification also considers pharmacokinetics, pharmacodynamics, mode-of-action in experimental animals, and relevance to humans. For example, ∝2u-globulin (a male rat-specific protein) related kidney toxicity and cancer in male rats has no concordance with humans and mice are much more resistant to aflatoxin B1-induced liver cancer than rats [473,474]. Based on the information presented here, many molds and mycotoxins commonly detected in samples collected from the suspected mold-infested buildings and residents are identified to cause adverse health effects including some causing cancer to animals and humans (see above for details).
The second step of the risk assessment is the determination of the dose-response (or exposure response) relationship, i.e., degree of adverse health effects at different exposure (dose), normally in experimental animals. Terminologies frequently used in assessing dose-response relationships include: 1) no-observed adverse effect level (NOAEL), the highest exposure level (dose) at which no statistical or biological significant increase in the frequency and/or severity of adverse effects is observed in exposed than non-exposed (control) populations; 2) lowest-observed-adverse-effect level (LOAEL) when some adverse effect(s) is/are observed at the lowest dose tested; 3) benchmark dose (BMD), determined by mathematical modeling, as an alternative to NOAEL.
The LOAEL, NOAEL, or statistical lower confidence limit of BMD that is used as the point of departure for extrapolation to lower doses. The NOAEL (preferred), LOAEL (when NOAEL is not achieved), or lower confidence limit of BMD is used to calculate maximum acceptable dose of a toxic substance, also called reference dose (RfD) or reference concentration (RfC) for inhalation exposure, or acceptable/tolerable daily intake (ADI/TDI), by applying uncertainty factors (UFs). The UFs are generally applied in the order-of-magnitude to account for the variability and uncertainty from differences between test animals and humans (generally 10-fold) and variability within the human population (generally another 10-fold). When LOAEL, instead of NOAEL, is used, another 10-fold UF is used; use of lower or higher UFs depend upon the quality of the generated toxicological, toxicokinetic, and toxicodynamic data in experimental animals as well as human relevance of the effects in animals. For most of the mycotoxins determined in urine samples collected from the residents of the suspected mold-infested buildings and presented in (Table 4), dose-response data already exist and TDI developed (Table 6). For additional information readers are directed to Borchers et al. [475] publication.
|
Mycotoxin |
TDI (μg/kg/day) |
|
AflatoxinB1 (Ml)a,b |
0.001 |
|
Citrinin |
0.2 |
|
Fumonisins (all) |
2 |
|
Fumonisins (Bl/B2) |
1 |
|
Ochratoxin AC |
0.0012-0.014 |
|
Trichothecenes (Type A)d |
0.06e |
|
Trichothecenes (Type B) |
1f, 0.7g |
|
Zearalenone |
0.07-025 |
|
References used to compile this table [142,143,259,310,311,411,453,454,475,478-480].
aAflatoxin M1 is the hydroxylated metabolite of aflatoxin B1. bJECFA calculated intake of even 1 ng/kg/day will cause one extra cancer case in 105 individuals. cProvisional maximum TDI. dFor T-2 toxin. eTemporary TDI. fFor deoxynivalenol. gFor nivalenol. |
|
Unfortunately, extremely limited dose-response relationship data are available for molds, even in experimental animals. There are only a few animal studies where animals were dosed with known number of spores and adverse health effects determined. For example, Flemming et al. [476] conducted a study in rats to determine NOAEL of S. chartarum. They dosed rats with 30, 300, and 3000 S. chartarum spores/g bodyweight via intratracheal instillations and determined inflammatory biomarkers in the lung lavage. The NOAEL of the study was < 30 S. chartarum spores/g. Using this NOAEL, one can calculate TDI by dividing NOAEL in animals with UF. A UF of 10 is used to account for the possible differences in responsiveness between animals and humans, another UF of 10 is used to account for variation in susceptibility in human population. The UF of 100 is usually appropriate for many chemicals; however, for chemicals with less complete data, e.g., use of short-term study, as the case for Flemming et al. [476] study, an additional UF of 10 is required (leading to a UF of 1000) (https://www.epa.gov/iris/reference-dose-rfd-description-and-use-health-risk-assessments). Based on this risk assessment, TDI of S. chartarum in humans is <30 spores/kg bodyweight.
The third step in risk assessment is to determine the extent of exposure which entails measuring or estimating magnitude, frequency, and duration of exposure and sometimes estimating future exposures from certain environments, e.g., molds, bacteria, and related biotoxins when living in a mold-infested building. For the assessment of exposure to molds and biotoxins in indoors settings, levels of molds, bacteria, endotoxins are determined in air, dust and other samples collected from suspected mold-infested buildings, see (Tables 1-5) for details. Currently there are no regulations or standards for molds indoors including no threshold limit values for airborne mold or mold spore concentrations (https://www.epa.gov/mold/mold-testing-or-sampling#regs; https://www.osha.gov/mold/standards). Frequency and duration of exposure are estimated based on the duration of residence and normal time spent daily inside the building. For mycotoxins in urine and blood (rarely conducted) establishing systemic exposure, pharmacokinetic information is used to further adjust the actual systemic dose. This is especially helpful when samples are collected weeks or months after moving out from the mold-infested to non-mold-infested buildings to estimate the systemic exposure at the time of residing in the building in question [24].
As part of the fourth step in the risk assessment all the information gathered in the first three steps is summarized and integrated to synthesize overall conclusion about risk. Therefore, in the absence of any regulatory guidelines, several approaches can be used to determine if exposure has crossed the threshold of the adverse health effects. One approach that many mold-testing companies advocate is setting arbitrary number of spores in the air to classify the level as normal (<500 spores/m3) or high (>500 spores/m3). However, we consider a more scientific approach using the fact that levels of molds and spores indoors are mostly lower or equal to that found outdoor [5]. This approach compares the levels of spores indoors with that of the outdoors to make conclusions about overall risk based on the severity of adverse health effects rendered by the mold(s) and related biotoxin(s) in question [4,477]. For mycotoxins, on the other hand, systemic exposures are used to calculate risk based on the hazard (i.e., toxicity) and dose-response information as shown above and in (Table 6) along with other scientific approaches when such data are not available.
Conclusions
Out of an estimated 1.5–5.0 million fungal species [481,482], only several hundred can cause diseases in humans, primarily in immunocompromised and critically ill individuals, with only a very few can affect healthy individuals. The number of at-risk populations is unfortunately increasing globally over time due to the rise in immunocompromising diseases like diabetes along with genetic predisposition and environmental factors resulting in increased exposure to fungi and related health complications [24,480-482]. Among the environmental factors, there is growing evidence of a positive relationship between climate change and increased mold growth, sporulation, and allergies [41,43,485-487]. Recent data corroborate with the fact that a rise in fungal infections in humans has been observed with the rise in global temperature, precipitation, flooding, population, and urbanization [52,485,488,489].
As mentioned above, biotoxins (i.e., hyphal fragments, spores, and mycotoxins) cause a variety of allergies in people living or working in mold-infested buildings [2,8,10-16,19,20,22]. In addition to allergies, exposure to mycotoxins can cause many systemic toxicities to organs, e.g., respiratory and nervous systems, liver, kidney, and developing fetus; several of them are known (Group 1) or possibly (Group 2B) carcinogens [1,18,21,23,25]. Exposure to mycotoxins can also make individuals vulnerable to microbial diseases [25]. These adverse health effects may even be more pronounced in sensitive, e.g., immunocompromised and/or genetically predisposed to slow elimination, like HLA gene alleles, individuals [1,18,21,23,24,195].
Fungal (including mold) infections are among the most difficult diseases to manage, and invasive fungal infections cause significant morbidity and mortality [490-492]. High complexity in managing fungal infections is mostly due to nonspecific clinical presentations leading to poor diagnosis, lack of an array of antifungal agents, toxicity of the available antifungal medicines, and need of a prolong therapy [490-492]. It is estimated that globally, fungal infections occur to at least 13 million people and cause more than 1.5 million deaths every year [491]. In 2018, in the USA alone, approximately 666,235 fungal infections were diagnosed out of 35.5 million inpatients costing $6.7 billion; additionally, 6.6 million fungal infections were diagnosed in outpatients [491]. Approximately 76% of fungal infections were from Aspergillus, Pneumocystis, and Candida [491].
Assessing exposure to biotoxins, and bacteria/endotoxins, especially in indoor settings is challenging with the currently employed approaches. These approaches (e.g., airborne spores in breathing zone or internalized molds in feces; mycotoxins in urine and/or blood) only give a snapshot of exposure to biotoxins without providing trends of the long-term exposure or exposure from different environments. While results of these tests can confirm exposure, they do not provide information about when or where the exposure occurred. Source(s) of exposure is/are established by determining the proportion of time occupant(s) spend(s) at the building in question and at other building(s) (e.g., at work) and level of molds in other building(s). The timeline and extent of exposure to mycotoxins is determined by using kinetic information of mycotoxin(s) in question and any preexisting condition(s) of occupant(s) that may influence absorption, distribution, metabolism, and excretion (ADME) of mycotoxin(s), e.g., genetic predisposition. Elimination of OTA and MPA slows by ~10- and ~213-fold, respectively, in individuals with specific genotype of HLA/DR gene [24]. Some physicians claim to treat mold toxicity through the process of “detoxification” by dosing activated charcoal orally, in most cases, long after the cessation of exposure. They claim that activated charcoal mobilizes mycotoxins from different organs, where they may be sequestered, and bring them to the GI tract, where they bind with the orally dosed activated charcoal. Activated charcoal is commonly used in emergency to treat certain kinds of poisoning as it absorbs poisons present in the GI tract, mostly in stomach, and prevents their absorption into the body. There is no research that backs the claim that activated charcoal actively extract mycotoxins from the body; elimination of mycotoxins from the body is governed by ADME.
A rise in buildings with mold infestation is expected with rise in both temperature and humidity from the climate change, consequently, an increase in the number of patients with severe mold related diseases is also expected, thus warranting better health management. To address indoor mold-related illness, there is an urgent need to streamline the process of testing suspected mold-infested buildings by standardizing collection, analysis, and reporting of the results for the consistency and comparison of results across the testing laboratories. Additionally, the use of better markers of mold-related illness in humans are needed along with generation of animal and human (e.g., epidemiological studies) data. Quality animal studies are needed, at least for molds responsible for severe adverse health effects, to develop RfDs/RfCs, ADI/TDI for both mold components (e.g., spores, hyphal fragments) and mycotoxins, especially following inhalation exposure. A careful examination of factors that may influence the severity of illness, like dysbiosis of gut microbiota, endotoxin, other chemicals, and nutrition, is needed for better understanding of mold- and mycotoxin-related adverse health effects in humans. While data for the relevant route(s) of exposure are being generated, we can use risk values set for ingestion presented in this paper along with other available information like 0.5-15 μg/kg for aflatoxins in nuts, grains, dried figs, and milk and 50 μg/kg for patulin in apple juice [23] after incorporating differences in ADME between oral and inhalation routes of exposure. For this paper, we have used data of samples collected from over 800 suspected mold-infested buildings and over 2000 residents from the whole United States with the objective of compiling findings for use by the researchers and those working in this area.
Acknowledgements
Authors acknowledge David Merchwart of Bio Genesis Industries for using data generated by the Mold Test Company.
References
2. U.S. EPA (United States Environmental Protection Agency). A Brief Guide to Mold, Moisture and Your Home. 2023. https://www.epa.gov/mold/brief-guide-mold-moisture-and-your-home (accessed November 18, 2024).
3. Straus DC. Molds, mycotoxins, and sick building syndrome. Toxicol Ind Health. 2009 Oct-Nov;25(9-10):617-35.
4. Codina R, Fox RW, Lockey RF, DeMarco P, Bagg A. Typical levels of airborne fungal spores in houses without obvious moisture problems during a rainy season in Florida, USA. J Investig Allergol Clin Immunol. 2008;18(3):156-62.
5. Palaty C. Mould Assessment in Indoor Environments-Review of Guidelines and Evidence. Metaphase Health Research Consulting Inc, National Collaborating Centre for Environmental Health, Canada. 2010. https://ncceh.ca/sites/default/files/Mould_Assessment_May_2010.pdf (accessed November 18, 2024).
6. Institute of Medicine (US) Committee on Damp Indoor Spaces and Health. Damp Indoor Spaces and Health. Washington (DC): National Academies Press (US); 2004.
7. Croft WA, Jarvis BB, Yatawara CS. Airborne outbreak of trichothecene toxicosis. Atmospheric Environment (1967). 1986 Jan 1;20(3):549-52.
8. Creasia DA, Thurman JD, Wannemacher RW Jr, Bunner DL. Acute inhalation toxicity of T-2 mycotoxin in the rat and guinea pig. Fundam Appl Toxicol. 1990 Jan;14(1):54-9.
9. Dearborn DG, Yike I, Sorenson WG, Miller MJ, Etzel RA. Overview of investigations into pulmonary hemorrhage among infants in Cleveland, Ohio. Environ Health Perspect. 1999 Jun;107 Suppl 3(Suppl 3):495-9.
10. Johanning E, Landsbergis P, Gareis M, Yang CS, Olmsted E. Clinical experience and results of a Sentinel Health Investigation related to indoor fungal exposure. Environ Health Perspect. 1999 Jun;107 Suppl 3(Suppl 3):489-94.
11. Robbins CA, Swenson LJ, Nealley ML, Gots RE, Kelman BJ. Health effects of mycotoxins in indoor air: a critical review. Appl Occup Environ Hyg. 2000 Oct;15(10):773-84.
12. Górny RL, Reponen T, Willeke K, Schmechel D, Robine E, Boissier M, et al. Fungal fragments as indoor air biocontaminants. Appl Environ Microbiol. 2002 Jul;68(7):3522-31.
13. Górny RL. Filamentous microorganisms and their fragments in indoor air--a review. Ann Agric Environ Med. 2004;11(2):185-97.
14. Hooper DG, Bolton VE, Guilford FT, Straus DC. Mycotoxin detection in human samples from patients exposed to environmental molds. Int J Mol Sci. 2009 Apr 1;10(4):1465-75.
15. WHO (Word Health Organization). Guidelines for indoor air quality: Dampness and mould. Geneva, WHO. 2009. https://apps.who.int/iris/handle/10665/164348 (accessed November 18, 2024).
16. Brewer JH, Thrasher JD, Straus DC, Madison RA, Hooper D. Detection of mycotoxins in patients with chronic fatigue syndrome. Toxins (Basel). 2013 Apr 11;5(4):605-17.
17. Mueller A, Schlink U, Wichmann G, Bauer M, Graebsch C, Schüürmann G, et al. Individual and combined effects of mycotoxins from typical indoor moulds. Toxicol In Vitro. 2013 Sep;27(6):1970-8.
18. Köhler JR, Casadevall A, Perfect J. The spectrum of fungi that infects humans. Cold Spring Harb Perspect Med. 2014 Nov 3;5(1):a019273.
19. Baxi SN, Portnoy JM, Larenas-Linnemann D, Phipatanakul W; Environmental Allergens Workgroup. Exposure and Health Effects of Fungi on Humans. J Allergy Clin Immunol Pract. 2016 May-Jun;4(3):396-404.
20. Thrasher JD, Prokop C, Roberts C, Hooper D. A family with ME/CFS following exposure to molds, mycotoxins and bacteria in a water-damaged home: a case report. Int J. 2016;4:15.
21. Harding CF, Pytte CL, Page KG, Ryberg KJ, Normand E, Remigio GJ, et al. Mold inhalation causes innate immune activation, neural, cognitive and emotional dysfunction. Brain Behav Immun. 2020 Jul;87:218-28.
22. Jakšić D, Sertić M, Kifer D, Kocsubè S, Mornar Turk A, Nigović B, et al. Fungi and their secondary metabolites in water-damaged indoors after a major flood event in eastern Croatia. Indoor Air. 2021 May;31(3):730-44.
23. WHO (World Health Organization). Mycotoxins. WHO publications. 2023. https://www.who.int/news-room/fact-sheets/detail/mycotoxins (accessed November 18, 2024).
24. Saghir SA, Ansari RA. HLA gene variations and mycotoxin toxicity: Four case reports. Mycotoxin Res. 2024 Feb;40(1):159-73.
25. Bennett JW, Klich M. Mycotoxins. Clin Microbiol Rev. 2003 Jul;16(3):497-516.
26. Bornehag CG, Sundell J, Sigsgaard T. Dampness in buildings and health (DBH): Report from an ongoing epidemiological investigation on the association between indoor environmental factors and health effects among children in Sweden. Indoor Air. 2004;14 Suppl 7:59-66.
27. Gunnbjörnsdóttir MI, Franklin KA, Norbäck D, Björnsson E, Gislason D, Lindberg E, et al. Prevalence and incidence of respiratory symptoms in relation to indoor dampness: the RHINE study. Thorax. 2006 Mar;61(3):221-5.
28. Howden-Chapman P, Matheson A, Crane J, Viggers H, Cunningham M, Blakely T, et al. Effect of insulating existing houses on health inequality: cluster randomised study in the community. BMJ. 2007 Mar 3;334(7591):460.
29. Bloom E, Nyman E, Must A, Pehrson C, Larsson L. Molds and mycotoxins in indoor environments--a survey in water-damaged buildings. J Occup Environ Hyg. 2009 Nov;6(11):671-8.
30. Haverinen-Shaughnessy U. Prevalence of dampness and mold in European housing stock. J Expo Sci Environ Epidemiol. 2012 Sep;22(5):461-7.
31. Sun Y, Sundell J. On associations between housing characteristics, dampness and asthma and allergies among children in Northeast Texas. Indoor and Built Environment. 2013 Aug;22(4):678-84.
32. Weinmayr G, Gehring U, Genuneit J, Büchele G, Kleiner A, Siebers R, et al. Dampness and moulds in relation to respiratory and allergic symptoms in children: results from Phase Two of the International Study of Asthma and Allergies in Childhood (ISAAC Phase Two). Clin Exp Allergy. 2013 Jul;43(7):762-74.
33. Liu W, Huang C, Hu Y, Zou Z, Shen L, Sundell J. Associations of building characteristics and lifestyle behaviors with home dampness-related exposures in Shanghai dwellings. Building and Environment. 2015 Jun 1;88:106-15.
34. Cai J, Liu W, Hu Y, Zou Z, Shen L, Huang C. Associations between home dampness-related exposures and childhood eczema among 13,335 preschool children in Shanghai, China: A cross-sectional study. Environ Res. 2016 Apr;146:18-26.
35. Norbäck D, Zock JP, Plana E, Heinrich J, Tischer C, Jacobsen Bertelsen R, et al. Building dampness and mold in European homes in relation to climate, building characteristics and socio-economic status: The European Community Respiratory Health Survey ECRHS II. Indoor Air. 2017 Sep;27(5):921-32.
36. Cai J, Li B, Yu W, Wang H, Du C, Zhang Y, et al. Household dampness-related exposures in relation to childhood asthma and rhinitis in China: A multicentre observational study. Environ Int. 2019 May;126:735-46.
37. Ingham T, Keall M, Jones B, Aldridge DRT, Dowell AC, Davies C, et al. Damp mouldy housing and early childhood hospital admissions for acute respiratory infection: a case control study. Thorax. 2019 Sep;74(9):849-57.
38. NZG (New Zealand Government) (2019). One in five homes damp. https://www.stats.govt.nz/news/one-in-five-homes-damp (accessed November 18, 2024).
39. Howard A, Mansour A, Warren-Myers G, Jensen C, Bentley R. Housing typologies and asthma: a scoping review. BMC Public Health. 2023 Sep 11;23(1):1766.
40. LBNL (Lawrence Berkeley National Laboratory). Prevalence of Building Dampness. 2024. https://iaqscience.lbl.gov/prevalence-building-dampness (accessed November 18, 2024).
41. Beggs PJ, Bambrick HJ. Is the global rise of asthma an early impact of anthropogenic climate change? Environ Health Perspect. 2005 Aug;113(8):915-9.
42. Antova T, Pattenden S, Brunekreef B, Heinrich J, Rudnai P, Forastiere F, et al. Exposure to indoor mould and children's respiratory health in the PATY study. J Epidemiol Community Health. 2008 Aug;62(8):708-14.
43. Shea KM, Truckner RT, Weber RW, Peden DB. Climate change and allergic disease. J Allergy Clin Immunol. 2008 Sep;122(3):443-53; quiz 454-5.
44. Keall M, Baker MG, Howden-Chapman P, Cunningham M, Ormandy D. Assessing housing quality and its impact on health, safety and sustainability. J Epidemiol Community Health. 2010 Sep;64(9):765-71.
45. Vardoulakis S, Dimitroulopoulou C, Thornes J, Lai KM, Taylor J, Myers I, et al. Impact of climate change on the domestic indoor environment and associated health risks in the UK. Environ Int. 2015 Dec;85:299-313.
46. Fisk WJ. Review of some effects of climate change on indoor environmental quality and health and associated no-regrets mitigation measures. Building and Environment. 2015 Apr 1;86:70-80.
47. Dewsbury M, Law T, Potgieter J, Fitz-Gerald D, Mccomish B, Chandler T, Soudan A. Scoping study of condensation in residential buildings. Australian Build Codes Board. 2016. p. 1-98. https://www.abcb.gov.au/sites/default/files/resources/2020//Scoping_Study_of_Condensation_in_Residential_Buildings_Appendices.pdf, (accessed November 18, 2024).
48. Major JL, Boese GW. Cross Section of Legislative Approaches to Reducing Indoor Dampness and Mold. J Public Health Manag Pract. 2017 Jul/Aug;23(4):388-95.
49. Telfar-Barnard L, Bennett J, Howden-Chapman P, Jacobs DE, Ormandy D, Cutler-Welsh M, et al. Measuring the effect of housing quality interventions: the case of the New Zealand “rental warrant of fitness”. International Journal of Environmental Research and Public Health. 2017 Nov;14(11):1352.
50. Sharpe RA, Taylor T, Fleming LE, Morrissey K, Morris G, Wigglesworth R. Making the Case for "Whole System" Approaches: Integrating Public Health and Housing. Int J Environ Res Public Health. 2018 Oct 24;15(11):2345.
51. Baker E, Lester L, Beer A, Bentley R. An Australian geography of unhealthy housing. Geogr Res. 2019 Feb;57(1):40-51.
52. Dantas KC, Mauad T, de André CDS, Bierrenbach AL, Saldiva PHN. A single-centre, retrospective study of the incidence of invasive fungal infections during 85 years of autopsy service in Brazil. Sci Rep. 2021 Feb 17;11(1):3943.
53. U.S. EPA (United States Environmental Protection Agency). The Environmental Relative Moldiness Index (ERMI). 2021. https://www.epa.gov/system/files/documents/2021-09/updated-fact-sheet.ermi-_9.9.21.final_new-template_508-compliant_0.pdf (accessed November 18, 2024).
54. Das S, Saha R, Dar SA, Ramachandran VG. Acremonium species: a review of the etiological agents of emerging hyalohyphomycosis. Mycopathologia. 2010 Dec;170(6):361-75.
55. Fincher RM, Fisher JF, Lovell RD, Newman CL, Espinel-Ingroff A, Shadomy HJ. Infection due to the fungus Acremonium (cephalosporium). Medicine (Baltimore). 1991 Nov;70(6):398-409.
56. Fridkin SK, Kremer FB, Bland LA, Padhye A, McNeil MM, Jarvis WR. Acremonium kiliense endophthalmitis that occurred after cataract extraction in an ambulatory surgical center and was traced to an environmental reservoir. Clin Infect Dis. 1996 Feb;22(2):222-7.
57. Patterson R, Fink JN, Miles WB, Basich JE, Schleuter DB, Tinkelman DG, et al. Hypersensitivity lung disease presumptively due to Cephalosporium in homes contaminated by sewage flooding or by humidifier water. J Allergy Clin Immunol. 1981 Aug;68(2):128-32.
58. Suda T, Sato A, Ida M, Gemma H, Hayakawa H, Chida K. Hypersensitivity pneumonitis associated with home ultrasonic humidifiers. Chest. 1995 Mar;107(3):711-7.
59. Fakharian A, Dorudinia A, Alavi Darazam I, Mansouri D, Masjedi MR. Acremonium Pneumonia: Case Report and Literature Review. Tanaffos. 2015;14(2):156-60.
60. Rocha O, Ansari K, Doohan FM. Effects of trichothecene mycotoxins on eukaryotic cells: a review. Food Addit Contam. 2005 Apr;22(4):369-78.
61. Bunyapaiboonsri T, Yoiprommarat S, Lapanun S, Balram U, Chanthaket R, Klaysuban A, Suetrong S. Trichothecenes from the fungus Acremonium crotocinigenum BCC 20012. Phytochem Lett. 2016 Dec 1;18:39-43.
62. Huang D, Cui L, Dai M, Wang X, Wu Q, Hussain HI, et al. Mitochondrion: A new molecular target and potential treatment strategies against trichothecenes. Trends in Food Science & Technology. 2019 Jun 1;88:33-45.
63. Fonseca-Guerra IR, Beltrán Pineda ME, Benavides Rozo ME. Characterization of Alternaria alternata and Alternaria scrophulariae Brown Spot in Colombian quinoa (Chenopodium quinoa). J Fungi (Basel). 2023 Sep 20;9(9):947.
64. Abdel-Gawad KM. Aspergillus fumigatus and Aspergillosis. Am J Biomed Sci & Res. 2021;14:002043.
65. Mokobi F. Alternaria alternata - an overview. In: Aryal S, Editor. Micobe Notes. 2021. https://microbenotes.com/alternaria-alternata/ (accessed November 18, 2024).
66. Hernandez-Ramirez G, Barber D, Tome-Amat J, Garrido-Arandia M, Diaz-Perales A. Alternaria as an Inducer of Allergic Sensitization. J Fungi (Basel). 2021 Oct 7;7(10):838.
67. Pastor FJ, Guarro J. Alternaria infections: laboratory diagnosis and relevant clinical features. Clin Microbiol Infect. 2008 Aug;14(8):734-46.
68. Dall’Asta C, Cirlini M, Falavigna M. Mycotoxins from Alternaria: Toxicological Implication. Adv Mol Toxicol. 2014;8:107-21.
69. EFSA Panel on Contaminants in the Food Chain (CONTAM). Scientific opinion on the risks for animal and public health related to the presence of Alternaria toxins in feed and food. EFSA Journal. 2011 Oct;9(10):2407.
70. López P, Venema D, de Rijk T, de Kok A, Scholten JM, Mol HG, et al. Occurrence of Alternaria toxins in food products in The Netherlands. Food Control. 2016 Feb 1;60:196-204.
71. Wei DL, Chang SC, Lin SC, Doong ML, Jong SC. Production of 3-nitropropionic acid by Arthrinium species. Current Microbiology. 1994 Jan;28:1-5.
72. He F, Zhang S, Qian F, Zhang C. Delayed dystonia with striatal CT lucencies induced by a mycotoxin (3-nitropropionic acid). Neurology. 1995 Dec;45(12):2178-83.
73. Birkelund T, Johansen RF, Illum DG, Dyrskog SE, Østergaard JA, Falconer TM, et al. Fatal 3-Nitropropionic Acid Poisoning after Consuming Coconut Water. Emerg Infect Dis. 2021 Jan;27(1):278-80.
74. Pfohl-Leszkowicz A, Manderville RA. Ochratoxin A: An overview on toxicity and carcinogenicity in animals and humans. Mol Nutr Food Res. 2007 Jan;51(1):61-99.
75. Moretti A, Susca A, Mulé G, Logrieco AF, Proctor RH. Molecular biodiversity of mycotoxigenic fungi that threaten food safety. Int J Food Microbiol. 2013 Oct 1;167(1):57-66.
76. Amare MG, Keller NP. Molecular mechanisms of Aspergillus flavus secondary metabolism and development. Fungal Genet Biol. 2014 May;66:11-8.
77. Xie L, Chen M, Ying Y. Development of Methods for Determination of Aflatoxins. Crit Rev Food Sci Nutr. 2016 Dec 9;56(16):2642-64.
78. Kumar P, Mahato DK, Kamle M, Mohanta TK, Kang SG. Aflatoxins: A Global Concern for Food Safety, Human Health and Their Management. Front Microbiol. 2017 Jan 17;7:2170.
79. Marchese S, Polo A, Ariano A, Velotto S, Costantini S, Severino L. Aflatoxin B1 and M1: Biological Properties and Their Involvement in Cancer Development. Toxins (Basel). 2018 May 24;10(6):214.
80. Tao Y, Xie S, Xu F, Liu A, Wang Y, Chen D, et al. Ochratoxin A: Toxicity, oxidative stress and metabolism. Food Chem Toxicol. 2018 Feb;112:320-31.
81. WHO (Word Health Organization). Mycotoxins. 2018. https://www.who.int/news-room/fact-sheets/detail/mycotoxins (accessed November 18, 2024).
82. Aguilar F, Hussain SP, Cerutti P. Aflatoxin B1 induces the transversion of G-->T in codon 249 of the p53 tumor suppressor gene in human hepatocytes. Proc Natl Acad Sci U S A. 1993 Sep 15;90(18):8586-90.
83. Taylor PE, Esch R, Flagan RC, House J, Tran L, Glovsky MM. Identification and possible disease mechanisms of an under-recognized fungus, Aureobasidium pullulans. International Archives of Allergy and Immunology. 2005 Dec 1;139(1):45-52.
84. Chowdhary A, Kathuria S, Agarwal K, Meis JF. Recognizing filamentous basidiomycetes as agents of human disease: A review. Med Mycol. 2014 Nov;52(8):782-97.
85. Park BJ, Wannemuehler KA, Marston BJ, Govender N, Pappas PG, Chiller TM. Estimation of the current global burden of cryptococcal meningitis among persons living with HIV/AIDS. AIDS. 2009 Feb 20;23(4):525-30.
86. Manamgoda DS, Rossman AY, Castlebury LA, Crous PW, Madrid H, Chukeatirote E, et al. The genus Bipolaris. Stud Mycol. 2014 Sep;79:221-88.
87. Jurgensen CW, Madsen A. Exposure to the airborne mould Botrytis and its health effects. Ann Agric Environ Med. 2009;16(2):183-96.
88. Soni KK, Turkane D, Jamaluddin J, Verma RK. Cephaliophora-a new seed rot fungal pathogen of teak from India. Indian J Trop Biodiv. 2009;17(1):95-6.
89. Zhao GuiHua ZG, Li DW. First report of Cephaliophora tropica on NL351 poplar in China. J W China Forest Sci. 2012;41:46-52.
90. Srivastava S, Kumar R, GUPTA GN, SINGH VP, SINHA A. First report of Cephaliophora irregularis as-sociated with the deterioration of Jatropha curcas L. seeds. J. Mycopathol. Res.. 2014;52(1):153-4.
91. Zhao L, Yang P, Zhao Z, Xia Y. First report of Cephaliophora tropica causing leaf spot on tomato (Solanum lycopersicum cv. Picus) in USA. Crop Protection. 2023 Oct 1;172:106324.
92. Hansen K, Perry BA, Dranginis AW, Pfister DH. A phylogeny of the highly diverse cup-fungus family Pyronemataceae (Pezizomycetes, Ascomycota) clarifies relationships and evolution of selected life history traits. Mol Phylogenet Evol. 2013 May;67(2):311-35.
93. Thaxter R. Contributions from the cryptogamic laboratory of Harvard University. LIV. New or peculier North American Hyphomycetes. III. Botanical Gazette XXXV. 1903. 153-59.
94. Mathews MS, Kuriakose T. Keratitis due to Cephaliophora irregularis Thaxter. J Med Vet Mycol. 1995 Sep-Oct;33(5):359-60.
95. Emmons CW, Lie-Kian-Joe, Eng NI, Pohan A, Kertopati S, Van der Meulen A. Basidiobolus and Cercospora from human infections. Mycologia. 1957 Jan 1;49(1):1-10.
96. Pieckova E. In vitro toxicity of indoor Chaetomium Kunze ex Fr. Ann Agric Environ Med. 2003;10(1):9-14.
97. Zhang Q, Li HQ, Zong SC, Gao JM, Zhang AL. Chemical and bioactive diversities of the genus Chaetomium secondary metabolites. Mini Rev Med Chem. 2012 Feb;12(2):127-48.
98. Stiller MJ, Rosenthal S, Summerbell RC, Pollack J, Chan A. Onychomycosis of the toenails caused by Chaetomium globosum. J Am Acad Dermatol. 1992 May;26(5 Pt 1):775-6.
99. Shi D, Lu G, Mei H, de Hoog GS, Zheng H, Liang G, et al. Onychomycosis due to Chaetomium globosum with yellowish black discoloration and periungual inflammation. Med Mycol Case Rep. 2016 Sep 14;13:12-6.
100. Niedoszytko M, Chełmińska M, Jassem E, Czestochowska E. Association between sensitization to Aureobasidium pullulans (Pullularia sp) and severity of asthma. Ann Allergy Asthma Immunol. 2007 Feb;98(2):153-6.
101. Vesper S, McKinstry C, Ashley P, Haugland R, Yeatts K, Bradham K, et al. Quantitative PCR analysis of molds in the dust from homes of asthmatic children in North Carolina. J Environ Monit. 2007 Aug;9(8):826-30.
102. Barron MA, Sutton DA, Veve R, Guarro J, Rinaldi M, Thompson E, et al. Invasive mycotic infections caused by Chaetomium perlucidum, a new agent of cerebral phaeohyphomycosis. J Clin Microbiol. 2003 Nov;41(11):5302-7.
103. Ohtsubo K, Saito M, Sekita S, Yoshihira K, Natori S. Acute toxic effects of chaetoglobosin A, a new cytochalasan compound produced by Chaetomium globosum, on mice and rats. Jpn J Exp Med. 1978 Apr;48(2):105-10.
104. Sekita S, Yoshihira K, Natori S, Udagawa S, Muroi T, Sugiyama Y, et al. Mycotoxin production by Chaetomium spp. and related fungi. Can J Microbiol. 1981 Aug;27(8):766-72.
105. Christensen CM, Nelson GH, Mirocha CJ, Bates F, Dorworth CE. Toxicity to rats of corn invaded by Chaetomium globosum. Appl Microbiol. 1966 Sep;14(5):774-7.
106. Gupta J, Pathak B, Sethi N, Vora VC. Histopathology of Mycotoxicosis produced in Swiss albino mice by metabolites of some fungal isolates. Appl Environ Microbiol. 1981 Mar;41(3):752-7.
107. Burge HA. Fungus allergens. Clin Rev Allergy. 1985 Jul;3(3):319-29.
108. McMullin DR, Sumarah MW, Miller JD. Chaetoglobosins and azaphilones produced by Canadian strains of Chaetomium globosum isolated from the indoor environment. Mycotoxin Res. 2013 Feb;29(1):47-54.
109. Ito Y, Ohtsubo K. Teratogenicity of oral chaetochromin, a polyphenolic mycotoxin produced by Chaetomium spp., to mice embryo. Bull Environ Contam Toxicol. 1987 Aug;39(2):299-303.
110. Theodore FH, Littman ML, Almeda E. Endophthalmitis following cataract extraction: Due to Neurospora Sitophila, a so-called nonpathogenic fungus. American Journal of Ophthalmology. 1962 Jan 1;53(1):35-9.
111. Bensch K, Braun U, Groenewald JZ, Crous PW. The genus Cladosporium. Stud Mycol. 2012 Jun 15;72(1):1-401.
112. Lumpkins ED Sr, Corbit SL, Tiedeman GM. Airborne fungi survey. 1. Culture-plate survey of the home environment. Ann Allergy. 1973 Aug;31(8):361-70.
113. Fradkin A, Tarlo SM, Tobin RS, Tucic-Porretta M, Malloch D. Species identification of airborne molds and its significance for the detection of indoor pollution. JAPCA. 1987 Jan;37(1):51-3.
114. Piecková E, Jesenská Z. Microscopic fungi in dwellings and their health implications in humans. Ann Agric Environ Med. 1999;6(1):1-11.
115. Kauffman HF, Tomee JF, van der Werf TS, de Monchy JG, Koëter GK. Review of fungus-induced asthmatic reactions. Am J Respir Crit Care Med. 1995 Jun;151(6):2109-15; discussion 2116.
116. Wijayawardene NN, Mckenzie EH, Chukeatirote E, Wang Y, Hyde KD. Coelomycetes. Cryptogamie, Mycologie. 2012 Sep;33(3):215-44.
117. Sutton BC. The Coelomycetes, Fungi Imperfecti with Pycnidia. Acervuli and Stromata. 1980:470-2.
118. Sutton DA. Coelomycetous fungi in human disease. A review: Clinical entities, pathogenesis, identification and therapy. Rev Iberoam Micol. 1999 Dec;16(4):171-9.
119. Stchigel AM, Sutton DA. Coelomycete fungi in the clinical lab. Current Fungal Infection Reports. 2013 Sep;7:171-91.
120. Qi Y, Xie Y, Zhang X, Pu J, Zhang H, Huang S, et al. Molecular and pathogenic variation identified among isolates of Corynespora cassiicola. Mol Biotechnol. 2009 Feb;41(2):145-51.
121. Sumabat LG, Kemerait RC Jr, Brewer MT. Phylogenetic Diversity and Host Specialization of Corynespora cassiicola Responsible for Emerging Target Spot Disease of Cotton and Other Crops in the Southeastern United States. Phytopathology. 2018 Jul;108(7):892-901.
122. Zou JJ, Li J, Ma SS, Li PF, Zhou DH. Subcutaneous phaeohyphomycosis caused by plant pathogenic Corynespora cassiicola: A case report. Chin J Traumatol. 2022 Nov;25(6):400-3.
123. Huang HK, Liu CE, Liou JH, Hsiue HC, Hsiao CH, Hsueh PR. Subcutaneous infection caused by Corynespora cassiicola, a plant pathogen. Journal of Infection. 2010 Feb 1;60(2):188-90.
124. Lv GX, Ge YP, Shen YN, Li M, Zhang X, Chen H, et al. Phaeohyphomycosis caused by a plant pathogen, Corynespora cassiicola. Med Mycol. 2011 Aug;49(6):657-61.
125. Yan XX, Yu CP, Fu XA, Bao FF, Du DH, Wang C, et al. CARD9 mutation linked to Corynespora cassiicola infection in a Chinese patient. Br J Dermatol. 2016 Jan;174(1):176-9.
126. Bengyella L, Iftikhar S, Nawaz K, Fonmboh DJ, Yekwa EL, Jones RC, et al. Biotechnological application of endophytic filamentous bipolaris and curvularia: a review on bioeconomy impact. World J Microbiol Biotechnol. 2019 Apr 22;35(5):69.
127. MacMillan RH 3rd, Cooper PH, Body BA, Mills AS. Allergic fungal sinusitis due to Curvularia lunata. Hum Pathol. 1987 Sep;18(9):960-4.
128. Ebright JR, Chandrasekar PH, Marks S, Fairfax MR, Aneziokoro A, McGinnis MR. Invasive sinusitis and cerebritis due to Curvularia clavata in an immunocompetent adult. Clin Infect Dis. 1999 Mar;28(3):687-9.
129. Wilhelmus KR, Jones DB. Curvularia keratitis. Trans Am Ophthalmol Soc. 2001;99:111-30.
130. Gupta R, Singh BP, Sridhara S, Gaur SN, Kumar R, Chaudhary VK, et al. Allergenic cross-reactivity of Curvularia lunata with other airborne fungal species. Allergy. 2002 Jul;57(7):636-40.
131. Flannigan B, Samson RA, Miller JD. Microorganisms in home and indoor work environments: diversity, health impacts, investigation and control. Boca Raton: CRC Press; 2011.
132. Elkhateeb WA, Daba GM. Epicoccum species as potent factories for the production of compounds of industrial, medical, and biological control applications. Biomedical Journal of Scientific and Technical Research. 2019;14(3):10616-20.
133. Oshikata C, Watanabe M, Saito A, Ishida M, Kobayashi S, Konuma R, et al. Allergic bronchopulmonary mycosis due to exposure to Eurotium herbariorum after the Great East Japan Earthquake. Prehospital and Disaster Medicine. 2017 Dec;32(6):688-90.
134. Haverinen U, Husman T, Toivola M, Suonketo J, Pentti M, Lindberg R, et al. An approach to management of critical indoor air problems in school buildings. Environ Health Perspect. 1999 Jun;107 Suppl 3(Suppl 3):509-14.
135. IARC Working Group on the Evaluation of Carcinogenic Risks to Humans, International Agency for Research on Cancer, World Health Organization. Some traditional herbal medicines, some mycotoxins, naphthalene and styrene. World Health Organization; 2002.
136. Escrivá L, Font G, Manyes L. In vivo toxicity studies of fusarium mycotoxins in the last decade: a review. Food Chem Toxicol. 2015 Apr;78:185-206.
137. Guerre P. Fusariotoxins in Avian Species: Toxicokinetics, Metabolism and Persistence in Tissues. Toxins (Basel). 2015 Jun 23;7(6):2289-305.
138. Summerell BA, Leslie JF. Fifty years of Fusarium: how could nine species have ever been enough?. Fungal Diversity. 2011 Sep;50:135-44.
139. Shephard GS, Thiel PG, Sydenham EW. Initial studies on the toxicokinetics of fumonisin B1 in rats. Food Chem Toxicol. 1992 Apr;30(4):277-9.
140. Martinez-Larranaga MR, Anadon A, Diaz MJ, Fernandez-Cruz ML, Martinez MA, Frejo MT, et al. Toxicokinetics and oral bioavailability of fumonisin B1. Vet Hum Toxicol. 1999 Dec;41(6):357-62.
141. Mostrom M. Mycotoxins: Classification. In: Caballero B, Finglas PM, Toldrá F, Editors. Encyclopedia of Food and Health. London: Academic Press; 2016. p. 29-34.
142. JECFA (Joint FAO/WHO Expert Committee on Food Additives). Evaluation of certain contaminants in food: Eighty-third report of the JECFA. WHO Technical Report Series 1002, World Health Organization. 2017. https://iris.who.int/handle/10665/254893 (accessed November 18, 2024).
143. EFSA Panel on Contaminants in the Food Chain (CONTAM), Knutsen HK, Barregård L, Bignami M, Brüschweiler B, Ceccatelli S, et al. Appropriateness to set a group health‐based guidance value for fumonisins and their modified forms. EFSA Journal. 2018 Feb;16(2):e05172.
144. Quan C, Spellberg B. Mucormycosis, pseudallescheriasis, and other uncommon mold infections. Proc Am Thorac Soc. 2010 May;7(3):210-5.
145. Cheng VC, Chan JF, Ngan AH, To KK, Leung SY, Tsoi HW, et al. Outbreak of intestinal infection due to Rhizopus microsporus. J Clin Microbiol. 2009 Sep;47(9):2834-43.
146. Ibrahim AS, Spellberg B, Avanessian V, Fu Y, Edwards JE Jr. Rhizopus oryzae adheres to, is phagocytosed by, and damages endothelial cells in vitro. Infect Immun. 2005 Feb;73(2):778-83.
147. Ribes JA, Vanover-Sams CL, Baker DJ. Zygomycetes in human disease. Clin Microbiol Rev. 2000 Apr;13(2):236-301.
148. Ananya TS, Kindo AJ, Subramanian A, Suresh K. " Nigrospora Sphaerica" Causing Corneal Ulcer in an Immunocompetent Woman: A Case Report. Int J Case Rep Images. 2014 Oct 1;5(10):675-9.
149. Motswaledi HM, Pillay RT. An unusual deep fungal infection with Nigrospora sphaerica in HIV positive patient. Int J Dermatol. 2019 Mar;58(3):333-5.
150. Takayama T, Inoda S, Watanabe A, Kawashima H. Nigrospora oryzae causing human corneal keratitis: A case report. Am J Ophthalmol Case Rep. 2024 Apr 14;34:102062.
151. Blomqvist K, Salonen A. Oidiodendron cerealis isolated from neurodermitis nuchae. Dermatologica. 1969;139(2):158-60.
152. Piecková E, Samson RA. Heat resistance of Paecilomyces variotii in sauce and juice. Journal of Industrial Microbiology and Biotechnology. 2000 Apr 1;24(4):227-30.
153. Dismukes WE, Pappas PG, Sobel JD. Clinical mycology. New York: Oxford University Press; 2003. p 263.
154. Nucci M, Anaissie EJ. Hyalohyphomycosis. In: Anaissie EJ, Pfaller MA. Clinical mycology. London: Elsevier; 2009. p. 309-27.
155. Rosales CMF, Cayetano MG, Saghir SA. Airborne Particles. In: Farland B, Klaunig J, Paustenbach D, Editors. Patty’s Toxicology. 7th ed. London: Wiley; 2024. p. 7168.
156. Selvin SS, Korah SM, Michael JS, Raj PM, Jacob P. Series of five cases of Papulaspora equi keratomycosis. Cornea. 2014 Jun;33(6):640-3.
157. AAAAI (American Academy of Allergy Asthma & Immunology) (2024). https://www.aaaai.org/conditions-treatments/allergies/mold-allergy (accessed November 18, 2024)
158. de Hoog GS, Guarro J, Gene J, Figueras MJ. Atlas of Clinical Fungi, 2nd ed. Utrecht, The Netherlands: Centraalbureau voor Schimmelcultures. 2000.
159. Fog Nielsen K. Mycotoxin production by indoor molds. Fungal Genet Biol. 2003 Jul;39(2):103-17.
160. Ismaiel AA, Papenbrock J. Mycotoxins: producing fungi and mechanisms of phytotoxicity. Agriculture. 2015 Sep;5(3):492-537.
161. Jackson SA, Dobson AD. Yeasts and molds: Penicillium camemberti. Ref Module Food Sci. 2016; p. 1-4.
162. Otero C, Arredondo C, Echeverría-Vega A, Gordillo-Fuenzalida F. Penicillium spp. mycotoxins found in food and feed and their health effects. World Mycotoxin Journal. 2020 Jul 1;13(3):323-43.
163. Monden Y, Yamamoto S, Yamakawa R, Sunada A, Asari S, Makimura K, et al. First case of fungal keratitis caused by Pestalotiopsis clavispora. Clin Ophthalmol. 2013;7:2261-4.
164. Lennartsson PR, Taherzadeh MJ, Edebo L. Rhizopus. In: Batt CA, Tortorello ML, Editors. Encyclopedia of Food Microbiology. Oxford: Academic Press; 2014. p. 284-90.
165. Markovskaja S, Kačergius A. Morphological and molecular characterisation of Periconia pseudobyssoides sp. nov. and closely related P. byssoides. Mycological Progress. 2014 May;13:291-302.
166. Chuaseeharonnachai C, Somrithipol S, Boonyuen N. Periconia notabilis sp. nov. and a new record and notes on the genus in Thailand. Mycotaxon. 2016 Oct 18;131(3):491-502.
167. Rojas TI, Aira MJ. Fungal biodiversity in indoor environments in Havana, Cuba. Aerobiologia. 2012 Sep;28:367-74.
168. Patil BY, Chavre BW. Survey of indoor airspora in Kallam tehsil of Osmanabad District, Maharashtra, India. Indian Journal of Pure and Applied Biology, 27 (1). 2012:65-9.
169. Gunasekaran R, Janakiraman D, Rajapandian SGK, Appavu SP, Namperumalsamy Venkatesh P, Prajna L. Periconia species - An unusual fungal pathogen causing mycotic keratitis. Indian J Med Microbiol. 2021 Jan;39(1):36-40.
170. Li JY, Sidhu RS, Ford EJ, Long DM, Hess WM, Strobel GA. The induction of taxol production in the endophytic fungus—Periconia sp from Torreya grandifolia. Journal of Industrial Microbiology and Biotechnology. 1998 May 1;20(5):259-64.
171. Teles HL, Sordi R, Silva GH, Castro-Gamboa I, da Silva Bolzani V, Pfenning LH, et al. Aromatic compounds produced by Periconia atropurpurea, an endophytic fungus associated with Xylopia aromatica. Phytochemistry. 2006 Dec 1;67(24):2686-90.
172. Bhilabutra W, Techowisan T, Peberdy JF, Lumyong S. Antimicrobial activity of bioactive compounds from Periconia siamensis CMUGE015. Res J Microbiol. 2007;2(10):749-55.
173. Verma VC, Lobkovsky E, Gange AC, Singh SK, Prakash S. Piperine production by endophytic fungus Periconia sp. isolated from Piper longum L. The Journal of Antibiotics. 2011 Jun;64(6):427-31.
174. Wu YH, Xiao GK, Chen GD, Wang CX, Hu D, Lian YY, et al. Pericocins A-D, New Bioactive Compounds from Periconia sp. Nat Prod Commun. 2015 Dec;10(12):2127-30.
175. De Lima TE, Bezerra JL, Cavalcanti MA. Phaeotrichoconis crotalariae, endophytic on Vitis labrusca in Brazil. Mycotaxon. 2012 Sep 28;120(1):291-4.
176. Shukla PK, Jain M, Lal B, Agrawal PK, Srivastava OP. Mycotic keratitis caused by Phaeotrichoconis crotalariae. New report. Mycoses. 1989 May;32(5):230-2.
177. Fernández M, Pérez V, Fuertes M, Benavides J, Espinosa J, Menéndez J, et al. Pathological Study of Facial Eczema (Pithomycotoxicosis) in Sheep. Animals (Basel). 2021 Apr 9;11(4):1070.
178. da Cunha KC, Sutton DA, Gené J, Cano J, Capilla J, Madrid H, et al. Pithomyces species (Montagnulaceae) from clinical specimens: identification and antifungal susceptibility profiles. Med Mycol. 2014 Oct;52(7):748-57.
179. Kidd S, Halliday C, Alexiou H, Ellis D. Descriptions of medical fungi 3rd edition. Newstyle Printing, Australia. 2016.
180. Shah H, Honeybul S, Tang S, Arthur I, McLaren S, Boan P. Mould meningitis associated with intravenous drug use. Med Mycol Case Rep. 2018 Jan 10;20:18-20.
181. Walsh TJ, Hayden RT, Larone DH. Larone's medically important fungi: A guide to identification. 6th ed. London: John Wiley & Sons; 2018.
182. Barron GL, Cain RF, Gilman JC. The genus Microascus. Can J Botany. 1961 Nov 1;39(7):1609-31.
183. Issakainen J, Heikkilä H, Vainio E, Koukila-Kähkölä P, Castren M, Liimatainen O, et al. Occurrence of Scopulariopsis and Scedosporium in nails and keratinous skin. A 5-year retrospective multi-center study. Med Mycol. 2007 May;45(3):201-9.
184. Moore D, Robson GD, Trinci AP. 21st century guidebook to fungi. 2nd ed. Cambridge University Press; 2011. p. 610.
185. Neglia JP, Hurd DD, Ferrieri P, Snover DC. Invasive Scopulariopsis in the immunocompromised host. Am J Med. 1987 Dec;83(6):1163-6.
186. Sandoval-Denis M, Sutton DA, Fothergill AW, Cano-Lira J, Gené J, Decock CA, et al. Scopulariopsis, a poorly known opportunistic fungus: spectrum of species in clinical samples and in vitro responses to antifungal drugs. J Clin Microbiol. 2013 Dec;51(12):3937-43.
187. Cullen WR. The toxicity of trimethylarsine: an urban myth. J Environ Monit. 2005 Jan;7(1):11-5.
188. Vánky K. Smut fungi (Basidiomycota p.p., Ascomycota p.p.) of the world. novelties, selected examples, trends. Acta Microbiol Immunol Hung. 2008 Jun;55(2):91-109.
189. Piepenbring M. Diversity, ecology, and systematics of smut fungi. Tropical Biology and Conservation Management-VI: Phytopathology and Entomology. 2009 May 11:140.
190. Wittich FW, Stakman EC. Case of respiratory allergy due to inhalation of grain smuts. Journal of Allergy. 1937 Jan 1;8(2):189-93.
191. Wittich FW. Further observations on allergy to smuts. Journal-Lancet. 1939;59:382.
192. González Glez Minero FJ, Candau P, González Glez Romano ML, Romero F. A study of the aeromycoflora of Cádiz: relationship to anthropogenic activity. J Investig Allergol Clin Immunol. 1992 Jul-Aug;2(4):211-5.
193. Yoshida K, Suga M, Yamasaki H, Nakamura K, Sato T, Kakishima M, et al. Hypersensitivity pneumonitis induced by a smut fungus Ustilago esculenta. Thorax. 1996 Jun;51(6):650-1; discussion 656-7.
194. Constable PD, Hinchcliff KW, Done SH, Gruenberg W. Diseases of the Liver. In: Veterinary Medicine. 11th ed. London: Elsevier Health Sciences; 2017. p. 622-56.
195. Croft WA, Jarvis BB, Yatawara CS. Airborne outbreak of trichothecene toxicosis. Atmospheric Environment (1967). 1986 Jan 1;20(3):549-52.
196. Hodgson MJ, Morey P, Leung WY, Morrow L, Miller D, Jarvis BB, et al. Building-associated pulmonary disease from exposure to Stachybotrys chartarum and Aspergillus versicolor. J Occup Environ Med. 1998 Mar;40(3):241-9.
197. Pestka JJ, Yike I, Dearborn DG, Ward MD, Harkema JR. Stachybotrys chartarum, trichothecene mycotoxins, and damp building-related illness: new insights into a public health enigma. Toxicol Sci. 2008 Jul;104(1):4-26.
198. Miller JD, Rand TG, Jarvis BB. Stachybotrys chartarum: cause of human disease or media darling? Med Mycol. 2003 Aug;41(4):271-91.
199. Nikulin M, Reijula K, Jarvis BB, Hintikka EL. Experimental lung mycotoxicosis in mice induced by Stachybotrys atra. Int J Exp Pathol. 1996 Oct;77(5):213-8.
200. Nikulin M, Reijula K, Jarvis BB, Veijalainen P, Hintikka EL. Effects of intranasal exposure to spores of Stachybotrys atra in mice. Fundam Appl Toxicol. 1997 Feb;35(2):182-8.
201. Lichtenstein JH, Molina RM, Donaghey TC, Amuzie CJ, Pestka JJ, Coull BA, et al. Pulmonary responses to Stachybotrys chartarum and its toxins: mouse strain affects clearance and macrophage cytotoxicity. Toxicol Sci. 2010 Jul;116(1):113-21.
202. Elidemir O, Colasurdo GN, Rossmann SN, Fan LL. Isolation of Stachybotrys from the lung of a child with pulmonary hemosiderosis. Pediatrics. 1999 Oct;104(4 Pt 1):964-6.
203. Flappan SM, Portnoy J, Jones P, Barnes C. Infant pulmonary hemorrhage in a suburban home with water damage and mold (Stachybotrys atra). Environmental Health Perspectives. 1999 Nov;107(11):927-30.
204. Gutiérrez-Rodríguez A, Postigo I, Guisantes JA, Suñén E, Martínez J. Identification of allergens homologous to Alt a 1 from Stemphylium botryosum and Ulocladium botrytis. Med Mycol. 2011 Nov;49(8):892-6.
205. Rodríguez-Gutiérrez G, Carrillo-Casas EM, Arenas R, García-Méndez JO, Toussaint S, Moreno-Morales ME, et al. Mucormycosis in a Non-Hodgkin Lymphoma Patient Caused by Syncephalastrum racemosum: Case Report and Review of Literature. Mycopathologia. 2015 Aug;180(1-2):89-93.
206. Irshad M, Nasir N, Hashmi UH, Farooqi J, Mahmood SF. Invasive pulmonary infection by Syncephalastrum species: Two case reports and review of literature. IDCases. 2020 Jul 25;21:e00913.
207. Kamalam A, Thambiah AS. Cutaneous infection by Syncephalastrum. Sabouraudia. 1980 Mar;18(1):19-20.
208. Mathuram AJ, Mohanraj P, Mathews MS. Rhino-orbital-cerebral infection by Syncephalastrum racemosusm. J Assoc Physicians India. 2013 May;61(5):339-40.
209. Newmark E, Polack FM. Tetraploa keratomycosis. Am J Ophthalmol. 1970 Dec;70(6):1013-5.
210. Liesegang TJ, Forster RK. Spectrum of microbial keratitis in South Florida. Am J Ophthalmol. 1980 Jul;90(1):38-47.
211. Markham WD, Key RD, Padhye AA, Ajello L. Phaeohyphomycotic cyst caused by Tetraploa aristata. J Med Vet Mycol. 1990;28(2):147-50.
212. Hyde KD, Dong Y, Phookamsak R, Jeewon R, Bhat DJ, Jones EG, et al. Fungal diversity notes 1151–1276: taxonomic and phylogenetic contributions on genera and species of fungal taxa. Fungal Diversity. 2020 Jan;100:5-277.
213. Crous PW, Carris LM, Giraldo A, Groenewald JZ, Hawksworth DL, Hernández-Restrepo M, et al. The Genera of Fungi - fixing the application of the type species of generic names - G 2: Allantophomopsis, Latorua, Macrodiplodiopsis, Macrohilum, Milospium, Protostegia, Pyricularia, Robillarda, Rotula, Septoriella, Torula, and Wojnowicia. IMA Fungus. 2015 Jun;6(1):163-98.
214. Grinn-Gofroń A, Bosiacka B. Effects of meteorological factors on the composition of selected fungal spores in the air. Aerobiologia (Bologna). 2015;31(1):63-72.
215. Çolakoğlu G. Indoor and outdoor mycoflora in the different districts of the city of Istanbul (Turkey). Indoor Built Environ. 2004 Apr;13(2):91-100.
216. Wu D, Zhang Y, Qin W, Zhao C, Li J, Hou Y, et al. Seasonal structural characteristics of indoor airborne fungi in library rooms by culturing and high-throughput sequencing. Building and Environment. 2021 Dec 1;206:108368.
217. Karmakar B, SenGupta K, Kaur A, Roy A, Gupta Bhattacharya S. Fungal bio-aerosol in multiple micro-environments from eastern India: source, distribution, and health hazards. SN Applied Sciences. 2020;2:1-14.
218. García-Mozo H, López-Orozco R, Canalejo C, Oteros J. Indoor biological particles in a train: comparative analysis with outdoor atmosphere. Aerobiologia. 2020 Sep;36(3):481-92.
219. Wang L, Dong JY, Song HC, Shen KZ, Wang LM, Sun R, et al. Screening and isolation of antibacterial activities of the fermentative extracts of freshwater fungi from Yunnan Province, China. Annals of Microbiology. 2008 Dec;58:579-84.
220. Geng WL, Wang XY, Kurtan T, Mandi A, Tang H, Schulz B, et al. Herbarone, a rearranged heptaketide derivative from the sea hare associated fungus Torula herbarum. Journal of Natural Products. 2012 Oct 26;75(10):1828-32.
221. Osman ME, El-Beih AA, Khatab OK, Moghannem SA, Abdullah NH. Production of herbarin and dehydroherbarin by endophytic Chaetosphaeronema sp.(KY321184) isolated from Nepeta septemcrenata and evaluation of their bioactivities. South African Journal of Botany. 2018 Jul 1;117:174-83.
222. Al-Hedaithy SS. First report of human infection due to the fungus Triadelphia pulvinata. J Clin Microbiol. 2001 Sep;39(9):3386-9.
223. Edathodu J, Al-Abdely HM, Althawadi S, Wickes BL, Thompson EH, Wiederhold NP, et al. Invasive fungal infection due to Triadelphia pulvinata in a patient with acute myeloid leukemia. J Clin Microbiol. 2013 Oct;51(10):3426-9.
224. Crous PW, Wingfield MJ, Guarro J, Hernández-Restrepo M, Sutton DA, Acharya K, et al. (2015b). Fungal Planet description sheets: 320–370. Persoonia. 2015;34:167-266.
225. Ram RM, Singh HB. Trichoderma spp.: An opportunistic pathogen. Biotech Today: An International Journal of Biological Sciences. 2018;8(2):16-24.
226. Liu D. Molecular detection of human fungal pathogens. 1st ed. Boca Raton: CRC Press; 2011. p. 932.
227. Hübner CA, Jentsch TJ. Ion channel diseases. Hum Mol Genet. 2002 Oct 1;11(20):2435-45.
228. Brian PW. Production of gliotoxin by Trichoderma viride. Nature. 1944 Nov 25;154(3917):667-8.
229. Sharma A, Gautam S, Mishra BB. Trichothecium. In: Batt CA, Tortorello ML, Editors. Encyclopedia of Food Microbiology. 2nd ed. Oxford: Academic Press; 2014. p. 647-52.
230. Zajc J, Gunde-Cimerman N. The Genus Wallemia-From Contamination of Food to Health Threat. Microorganisms. 2018 May 21;6(2):46.
231. Zajc J, Kogej T, Galinski EA, Ramos J, Gunde-Cimerman N. Osmoadaptation strategy of the most halophilic fungus, Wallemia ichthyophaga, growing optimally at salinities above 15% NaCl. Appl Environ Microbiol. 2014 Jan;80(1):247-56.
232. Pitt JI. Hocking AD. Fungi and Food Spoilage. New York: Springer; 2009. p. 350-3.
233. Guarro J, Gugnani HC, Sood N, Batra R, Mayayo E, Gené J, et al. Subcutaneous phaeohyphomycosis caused by Wallemia sebi in an immunocompetent host. J Clin Microbiol. 2008 Mar;46(3):1129-31.
234. Richardson M. The ecology of the Zygomycetes and its impact on environmental exposure. Clin Microbiol Infect. 2009 Oct;15 Suppl 5:2-9.
235. Vallabhaneni S, Mody RK. Gastrointestinal mucormycosis in neonates: A review. Current Fungal Infection Reports. 2015 Dec;9:269-74.
236. Song Y, Qiao J, Giovanni G, Liu G, Yang H, Wu J, et al. Mucormycosis in renal transplant recipients: review of 174 reported cases. BMC Infect Dis. 2017 Apr 18;17(1):283.
237. Francis JR, Villanueva P, Bryant P, Blyth CC. Mucormycosis in Children: Review and Recommendations for Management. J Pediatric Infect Dis Soc. 2018 May 15;7(2):159-164.
238. Marin DE, Pistol GC, Gras MA, Palade ML, Taranu I. Comparative effect of ochratoxin A on inflammation and oxidative stress parameters in gut and kidney of piglets. Regul Toxicol Pharmacol. 2017 Oct;89:224-31.
239. Wood LF, Wood MP, Fisher BS, Jaspan HB, Sodora DL. T Cell Activation in South African HIV-Exposed Infants Correlates with Ochratoxin A Exposure. Front Immunol. 2017 Dec 22;8:1857.
240. Yang J, Li J, Jiang Y, Duan X, Qu H, Yang B, et al. Natural occurrence, analysis, and prevention of mycotoxins in fruits and their processed products. Crit Rev Food Sci Nutr. 2014;54(1):64-83.
241. Ostry V, Malir F, Toman J, Grosse Y. Mycotoxins as human carcinogens-the IARC Monographs classification. Mycotoxin Res. 2017 Feb;33(1):65-73.
242. Claeys L, Romano C, De Ruyck K, Wilson H, Fervers B, Korenjak M, et al. Mycotoxin exposure and human cancer risk: A systematic review of epidemiological studies. Compr Rev Food Sci Food Saf. 2020 Jul;19(4):1449-64.
243. Turner NW, Bramhmbhatt H, Szabo-Vezse M, Poma A, Coker R, Piletsky SA. Analytical methods for determination of mycotoxins: An update (2009-2014). Anal Chim Acta. 2015 Dec 11;901:12-33.
244. Abrunhosa L, Morales H, Soares C, Calado T, Vila-Chã AS, Pereira M, et al. A Review of Mycotoxins in Food and Feed Products in Portugal and Estimation of Probable Daily Intakes. Crit Rev Food Sci Nutr. 2016;56(2):249-65.
245. French PW, Ludowyke RI, Guillemin GJ. Fungal-contaminated grass and well water and sporadic amyotrophic lateral sclerosis. Neural Regen Res. 2019 Sep;14(9):1490-3.
246. Gao Y, Meng L, Liu H, Wang J, Zheng N. The Compromised Intestinal Barrier Induced by Mycotoxins. Toxins (Basel). 2020 Sep 28;12(10):619.
247. Gonkowski S, Gajęcka M, Makowska K. Mycotoxins and the enteric nervous system. Toxins. 2020 Jul 19;12(7):461.
248. Kraft S, Buchenauer L, Polte T. Mold, Mycotoxins and a Dysregulated Immune System: A Combination of Concern? Int J Mol Sci. 2021 Nov 12;22(22):12269.
249. Kercsmar CM, Dearborn DG, Schluchter M, Xue L, Kirchner HL, Sobolewski J, et al. Reduction in asthma morbidity in children as a result of home remediation aimed at moisture sources. Environ Health Perspect. 2006 Oct;114(10):1574-80.
250. Duarte SC, Pena A, Lino CM. Human ochratoxin a biomarkers--from exposure to effect. Crit Rev Toxicol. 2011 Mar;41(3):187-212.
251. Rustom IY. Aflatoxin in food and feed: occurrence, legislation and inactivation by physical methods. Food Chemistry. 1997 May 1;59(1):57-67.
252. Reiter E, Zentek J, Razzazi E. Review on sample preparation strategies and methods used for the analysis of aflatoxins in food and feed. Mol Nutr Food Res. 2009 Apr;53(4):508-24.
253. Inan F, Pala M, Doymaz I. Use of ozone in detoxification of aflatoxin B1 in red pepper. Journal of Stored Products Research. 2007 Jan 1;43(4):425-9.
254. Somogyi A, Beck H. Nurturing and breast-feeding: exposure to chemicals in breast milk. Environ Health Perspect. 1993 Jul;101 Suppl 2(Suppl 2):45-52.
255. Giray B, Girgin G, Engin AB, Aydın S, Sahin G. Aflatoxin levels in wheat samples consumed in some regions of Turkey. Food Control. 2007 Jan 1;18(1):23-9.
256. Hussain I, Anwar J. A study on contamination of aflatoxin M1 in raw milk in the Punjab province of Pakistan. Food Control. 2008 Apr 1;19(4):393-5.
257. Kamkar A, Yazdankhah S, Nafchi AM, Nejad AS. Aflatoxin M1 in raw cow and buffalo milk in Shush city of Iran. Food Addit Contam Part B Surveill. 2014;7(1):21-4.
258. Dhakal A, Hashmi MF, Sbar E. Aflatoxin Toxicity. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024.
259. European Food Safety Authority (EFSA). Opinion of the scientific panel on contaminants in the food chain [CONTAM] related to the potential increase of consumer health risk by a possible increase of the existing maximum levels for aflatoxins in almonds, hazelnuts and pistachios and derived products. EFSA Journal. 2007 Mar;5(3):446.
260. Krishnamachari KA, Bhat RV, Nagarajan V, Tilak TB. Investigations into an outbreak of hepatitis in parts of western India. Indian J Med Res. 1975 Jul;63(7):1036-49.
261. Ngindu A, Johnson BK, Kenya PR, Ngira JA, Ocheng DM, Nandwa H, et al. Outbreak of acute hepatitis caused by aflatoxin poisoning in Kenya. Lancet. 1982 Jun 12;1(8285):1346-8.
262. IARC (International Agency for Research on Cancer). IARC - Summaries & Evaluations: Aflatoxins (Group 1). Vol 82. 2002b; pp 171. Lyon. https://inchem.org/documents/iarc/vol82/82-04.html (accessed November 18, 2024).
263. CDC (Centers for Disease Control and Prevention). Outbreak of Aflatoxin Poisoning - Eastern and Central Provinces, Kenya, January-July 2004. 2004. https://www.cdc.gov/mmwr/preview/mmwrhtml/mm5334a4.htm (accessed November 18, 2024).
264. Azziz-Baumgartner E, Lindblade K, Gieseker K, Rogers HS, Kieszak S, Njapau H, et al. Case-control study of an acute aflatoxicosis outbreak, Kenya, 2004. Environ Health Perspect. 2005 Dec;113(12):1779-83.
265. Iqbal SZ, Mustafa HG, Asi MR, Jinap S. Variation in vitamin E level and aflatoxins contamination in different rice varieties. Journal of Cereal Science. 2014 Sep 1;60(2):352-5.
266. Gong Y, Hounsa A, Egal S, Turner PC, Sutcliffe AE, Hall AJ, et al. Postweaning exposure to aflatoxin results in impaired child growth: a longitudinal study in Benin, West Africa. Environmental Health Perspectives. 2004 Sep;112(13):1334-8.
267. Williams JH, Phillips TD, Jolly PE, Stiles JK, Jolly CM, Aggarwal D. Human aflatoxicosis in developing countries: a review of toxicology, exposure, potential health consequences, and interventions. Am J Clin Nutr. 2004 Nov;80(5):1106-22.
268. Cotty PJ, Jaime-Garcia R. Influences of climate on aflatoxin producing fungi and aflatoxin contamination. Int J Food Microbiol. 2007 Oct 20;119(1-2):109-15.
269. Krishnamachari KA, Bhat RV, Nagarajan V, Tilak TB. Hepatitis due to aflatoxicosis. An outbreak in Western India. Lancet. 1975 May 10;1(7915):1061-3.
270. Patten RC. Aflatoxins and disease. Am J Trop Med Hyg. 1981 Mar;30(2):422-5.
271. Hendrickse RG. Problems of future measles vaccination in developing countries. Trans R Soc Trop Med Hyg. 1975;69(1):31-5.
272. Venturini MC, Perfumo CJ, Risso MA, Gomez CM, Piscopo MV, Sala de Miguel M, et al. Effect of aflatoxin B1 on resistance induced by Bordetella bronchiseptica vaccine in rabbits. Vet Microbiol. 1990 Nov;25(2-3):209-16.
273. Meissonnier GM, Marin DE, Galtier P, Bertin G, Taranu I, Oswald IP. Modulation of the immune response by a group of fungal food contaminant, the aflatoxins. Nutrit Immun. 2006;2006:147-66.
274. Lamplugh SM, Hendrickse RG, Apeagyei F, Mwanmut DD. Aflatoxins in breast milk, neonatal cord blood, and serum of pregnant women. Br Med J (Clin Res Ed). 1988 Apr 2;296(6627):968.
275. De Vries HR, Maxwell SM, Hendrickse RG. Foetal and neonatal exposure to aflatoxins. Acta Paediatr Scand. 1989 May;78(3):373-8.
276. Hsieh LL, Hsieh TT. Detection of aflatoxin B1-DNA adducts in human placenta and cord blood. Cancer Res. 1993 Mar 15;53(6):1278-80.
277. Groopman JD, Egner PA, Schulze KJ, Wu LS, Merrill R, Mehra S, et al. Aflatoxin exposure during the first 1000 days of life in rural South Asia assessed by aflatoxin B₁-lysine albumin biomarkers. Food Chem Toxicol. 2014 Dec;74:184-9.
278. Smith LE, Prendergast AJ, Turner PC, Humphrey JH, Stoltzfus RJ. Aflatoxin exposure during pregnancy, maternal anemia, and adverse birth outcomes. The American Journal of Tropical Medicine and Hygiene. 2017 Apr 4;96(4):770.
279. Kyei NNA, Boakye D, Gabrysch S. Maternal mycotoxin exposure and adverse pregnancy outcomes: a systematic review. Mycotoxin Res. 2020 May;36(2):243-55.
280. Sarma UP, Bhetaria PJ, Devi P, Varma A. Aflatoxins: Implications on Health. Indian J Clin Biochem. 2017 Jun;32(2):124-33.
281. Kensler TW, Qian GS, Chen JG, Groopman JD. Translational strategies for cancer prevention in liver. Nat Rev Cancer. 2003 May;3(5):321-9.
282. Smela ME, Currier SS, Bailey EA, Essigmann JM. The chemistry and biology of aflatoxin B1: from mutational spectrometry to carcinogenesis. Carcinogenesis. 2001 Apr 1;22(4):535-45.
283. Wild CP, Turner PC. The toxicology of aflatoxins as a basis for public health decisions. Mutagenesis. 2002 Nov;17(6):471-81.
284. Verma RJ. Aflatoxin cause DNA damage. International Journal of Human Genetics. 2004 Dec 1;4(4):231-6.
285. Qureshi H, Hamid SS, Ali SS, Anwar J, Siddiqui AA, Khan NA. Cytotoxic effects of aflatoxin B1 on human brain microvascular endothelial cells of the blood-brain barrier. Med Mycol. 2015 May;53(4):409-16.
286. Gallagher EP, Kunze KL, Stapleton PL, Eaton DL. The kinetics of aflatoxin B1 oxidation by human cDNA-expressed and human liver microsomal cytochromes P450 1A2 and 3A4. Toxicol Appl Pharmacol. 1996 Dec;141(2):595-606.
287. Jolly PE, Inusah S, Lu B, Ellis WO, Nyarko A, Phillips TD, et al. Association between high aflatoxin B1 levels and high viral load in HIV-positive people. World Mycotoxin J. 2013;6(3):255-61.
288. Armendáriz CR, Fernández ÁJG, Gironés MCLR, de la Torre AH. Mycotoxins. In: Wexler P, Editors. Encyclopedia of Toxicology. 3rd ed. Oxford: Academic Press; 2014. p. 424-7.
289. Cox RJ, Simpson TJ. Fungal Type I Polyketides. In: Liu HW, Mander L, Editors. Comprehensive Natural Products II. London: Elsevier Health Sciences; 2010. pp. 347-83.
290. Huang T, W
291. Hua C, Yang Y, Sun L, Dou H, Tan R, Hou Y. Chaetoglobosin F, a small molecule compound, possesses immunomodulatory properties on bone marrow-derived dendritic cells via TLR9 signaling pathway. Immunobiology. 2013 Mar;218(3):292-302.
292. Umeda M, Tsutsui T, Saito M. Mutagenicity and inducibility of DNA single-strand breaks and chromosome aberrations by various mycotoxins. Gan. 1977 Oct;68(5):619-25.
293. Geisen R, Schmidt-Heydt M, Touhami N, Himmelsbach A. New aspects of ochratoxin A and citrinin biosynthesis in Penicillium. Current Opinion in Food Science. 2018 Oct 1;23:23-31.
294. Carlton WW, Sansing G, Szczech GM, Tuite J. Citrinin mycotoxicosis in beagle dogs. Food Cosmet Toxicol. 1974 Aug;12(4):479-90.
295. Hood RD, Hayes AW, Scammell JG. Effects of prenatal administration of citrinin and viriditoxin to mice. Food Cosmet Toxicol. 1976 Jun;14(3):175-8.
296. Reiss J. Mycotoxins in foodstuffs. X. Production of citrinin by Penicillium chrysogenum in bread. Food Cosmet Toxicol. 1977 Aug;15(4):303-7.
297. Gupta M, Sasmal D, Bandyopadhyay S, Bagchi G, Chatterjee T, Dey S. Hematological changes produced in mice by ochratoxin A and citrinin. Toxicology. 1983 Jan;26(1):55-62.
298. Mayura K, Parker R, Berndt WO, Phillips TD. Effect of simultaneous prenatal exposure to ochratoxin A and citrinin in the rat. J Toxicol Environ Health. 1984;13(4-6):553-61.
299. Da Lozzo EJ, Oliveira MB, Carnieri EG. Citrinin-induced mitochondrial permeability transition. J Biochem Mol Toxicol. 1998;12(5):291-7.
300. Xu BJ, Jia XQ, Gu LJ, Sung CK. Review on the qualitative and quantitative analysis of the mycotoxin citrinin. Food Control. 2006 Apr 1;17(4):271-85.
301. Yu FY, Liao YC, Chang CH, Liu BH. Citrinin induces apoptosis in HL-60 cells via activation of the mitochondrial pathway. Toxicol Lett. 2006 Feb 20;161(2):143-51.
302. Qingqing H, Linbo Y, Yunqian G, Shuqiang L. Toxic effects of citrinin on the male reproductive system in mice. Exp Toxicol Pathol. 2012 Jul;64(5):465-9.
303. Zargar S, Wani TA. Food Toxicity of Mycotoxin Citrinin and Molecular Mechanisms of Its Potential Toxicity Effects through the Implicated Targets Predicted by Computer-Aided Multidimensional Data Analysis. Life (Basel). 2023 Mar 26;13(4):880.
304. Friis P, Hasselager E, Krogh P. Isolation of citrinin and oxalic acid from Penicillium viridicatum Westling and their nephrotoxicity in rats and pigs. Acta Pathol Microbiol Scand. 1969;77(3):559-60.
305. Endo A, Kuroda M. Citrinin, an inhibitor of cholesterol synthesis. J Antibiot (Tokyo). 1976 Aug;29(8):841-3.
306. Ambrose AM, DeEds F. Some toxicological and pharmacological properties of citrinin. J Pharmacol Exp Ther. 1946 Oct;88(2):173-86.
307. Sakai F. An experimental study on the toxic effect, especially on the kidney of “yellowed rice” polluted by Penicillium citrinum Thom, as well as of citrinin, a pigment isolated from the mould. Folia Pharmacol Jpn. 1955;51:431-2.
308. Krogh P, Hasselager E, Friis P. Studies on fungal nephrotoxicity. 2. Isolation of two nephrotoxic compounds from Penicillium viridicatum Westling: citrinin and oxalic acid. Acta Pathol Microbiol Scand B Microbiol Immunol. 1970;78(4):401-13.
309. Reddy RV, Mayura K, Hayes AW, Berndt WO. Embryocidal, teratogenic and fetotoxic effects of citrinin in rats. Toxicology. 1982;25(2-3):151-60.
310. EFSA Panel on Contaminants in the Food Chain (CONTAM). Scientific Opinion on the risks for public and animal health related to the presence of citrinin in food and feed. EFSA Journal. 2012 Mar;10(3):2605.
311. DFG (Deutsche Forschungsgemeinschaft) Permanent Senate Commission on Food Safety. Toxicological Evaluation of Red Mould Rice: An Update. Deutsche Forschungsgemeinschaft. 2013. https://www.dfg.de/resource/blob/171286/af99a6ebade380eced5e1a07a9c35573/131206-sklm-red-mould-rice-update-data.pdf (accessed November 18, 2024).
312. López Sáncheza P, de Nijsa M, Spanjerb M, Pietric A, Bertuzzic T, Starski A, et al. Generation of occurrence data on citrinin in food. EFSA Supporting Publications. 2017 Feb;14(2):1177E.
313. Dunn BB, Stack ME, Park DL, Joshi A, Friedman L, King RL. Isolation and identification of dihydrocitrinone, a urinary metabolite of citrinin in rats. J Toxicol Environ Health. 1983 Aug-Sep;12(2-3):283-9.
314. Degen GH, Ali N, Gundert-Remy U. Preliminary data on citrinin kinetics in humans and their use to estimate citrinin exposure based on biomarkers. Toxicol Lett. 2018 Jan 5;282:43-8.
315. Föllmann W, Behm C, Degen GH. Toxicity of the mycotoxin citrinin and its metabolite dihydrocitrinone and of mixtures of citrinin and ochratoxin A in vitro. Arch Toxicol. 2014 May;88(5):1097-107.
316. Faisal Z, Vörös V, Lemli B, Derdák D, Kunsági-Máté S, Bálint M, et al. Interaction of the mycotoxin metabolite dihydrocitrinone with serum albumin. Mycotoxin Res. 2019 May;35(2):129-39.
317. Sy-Cordero AA, Pearce CJ, Oberlies NH. Revisiting the enniatins: a review of their isolation, biosynthesis, structure determination and biological activities. The Journal of Antibiotics. 2012 Nov;65(11):541-9.
318. Tomoda H, Huang XH, Cao J, Nishida H, Nagao R, Okuda S, et al. Inhibition of acyl-CoA: cholesterol acyltransferase activity by cyclodepsipeptide antibiotics. J Antibiot (Tokyo). 1992 Oct;45(10):1626-32.
319. Prosperini A, Juan-García A, Font G, Ruiz MJ. Reactive oxygen species involvement in apoptosis and mitochondrial damage in Caco-2 cells induced by enniatins A, A₁, B and B₁. Toxicol Lett. 2013 Sep 12;222(1):36-44.
320. Tonshin AA, Teplova VV, Andersson MA, Salkinoja-Salonen MS. The Fusarium mycotoxins enniatins and beauvericin cause mitochondrial dysfunction by affecting the mitochondrial volume regulation, oxidative phosphorylation and ion homeostasis. Toxicology. 2010 Sep 30;276(1):49-57.
321. Manyes L, Escrivá L, Serrano AB, Rodríguez-Carrasco Y, Tolosa J, Meca G, et al. A preliminary study in Wistar rats with enniatin A contaminated feed. Toxicol Mech Methods. 2014 Mar;24(3):179-90.
322. Dornetshuber R, Heffeter P, Kamyar MR, Peterbauer T, Berger W, Lemmens-Gruber R. Enniatin exerts p53-dependent cytostatic and p53-independent cytotoxic activities against human cancer cells. Chem Res Toxicol. 2007 Mar;20(3):465-73.
323. Wätjen W, Debbab A, Hohlfeld A, Chovolou Y, Kampkötter A, Edrada RA, et al. Enniatins A1, B and B1 from an endophytic strain of Fusarium tricinctum induce apoptotic cell death in H4IIE hepatoma cells accompanied by inhibition of ERK phosphorylation. Mol Nutr Food Res. 2009 Apr;53(4):431-40.
324. Gammelsrud A, Solhaug A, Dendelé B, Sandberg WJ, Ivanova L, Kocbach Bølling A, et al. Enniatin B-induced cell death and inflammatory responses in RAW 267.4 murine macrophages. Toxicol Appl Pharmacol. 2012 May 15;261(1):74-87.
325. Ivanova L, Skjerve E, Eriksen GS, Uhlig S. Cytotoxicity of enniatins A, A1, B, B1, B2 and B3 from Fusarium avenaceum. Toxicon. 2006 Jun 15;47(8):868-76.
326. Ivanova L, Egge-Jacobsen WM, Solhaug A, Thoen E, Fæste CK. Lysosomes as a possible target of enniatin B-induced toxicity in Caco-2 cells. Chem Res Toxicol. 2012 Aug 20;25(8):1662-74.
327. Behm C, Degen GH, Föllmann W. The Fusarium toxin enniatin B exerts no genotoxic activity, but pronounced cytotoxicity in vitro. Mol Nutr Food Res. 2009 Apr;53(4):423-30.
328. Juan-García A, Manyes L, Ruiz MJ, Font G. Involvement of enniatins-induced cytotoxicity in human HepG2 cells. Toxicol Lett. 2013 Apr 12;218(2):166-73.
329. Prosperini A, Berrada H, Ruiz MJ, Caloni F, Coccini T, Spicer LJ, et al. A Review of the Mycotoxin Enniatin B. Front Public Health. 2017 Nov 16;5:304.
330. Jonsson M, Jestoi M, Anthoni M, Welling A, Loivamaa I, Hallikainen V, et al. Fusarium mycotoxin enniatin B: Cytotoxic effects and changes in gene expression profile. Toxicol In Vitro. 2016 Aug;34:309-20.
331. Ruiz MJ, Franzova P, Juan-García A, Font G. Toxicological interactions between the mycotoxins beauvericin, deoxynivalenol and T-2 toxin in CHO-K1 cells in vitro. Toxicon. 2011 Sep 15;58(4):315-26.
332. Prosperini A, Meca G, Font G, Ruiz MJ. Study of the cytotoxic activity of beauvericin and fusaproliferin and bioavailability in vitro on Caco-2 cells. Food Chem Toxicol. 2012 Jul;50(7):2356-61.
333. Juan C, Manyes L, Font G, Juan-García A. Evaluation of immunologic effect of Enniatin A and quantitative determination in feces, urine and serum on treated Wistar rats. Toxicon. 2014 Sep;87:45-53.
334. Altomare C, Logrieco AF, Gallo A. Mycotoxins and mycotoxigenic fungi: Risk and management. A challenge for future global food safety and security. In: Zaragoza O, Casadevall A, Editors. Encyclopedia of Mycology, Vol 1. Netherlands: Elsevier; 2021. p. 64-93.
335. Kalayou S, Ndossi D, Frizzell C, Groseth PK, Connolly L, Sørlie M, et al. An investigation of the endocrine disrupting potential of enniatin B using in vitro bioassays. Toxicol Lett. 2015 Mar 4;233(2):84-94.
336. Rodríguez-Carrasco Y, Heilos D, Richter L, Süssmuth RD, Heffeter P, Sulyok M, et al. Mouse tissue distribution and persistence of the food-born fusariotoxins Enniatin B and Beauvericin. Toxicol Lett. 2016 Apr 15;247:35-44.
337. Ojiro R, Okano H, Ozawa S, Yamagata H, Zou X, Tang Q, et al. Pharmacokinetics and 28-day repeated-dose toxicity of enniatin B after oral administration in mice. Food Chem Toxicol. 2023 Jul;177:113814.
338. Devreese M, Broekaert N, De Mil T, Fraeyman S, De Backer P, Croubels S. Pilot toxicokinetic study and absolute oral bioavailability of the Fusarium mycotoxin enniatin B1 in pigs. Food Chem Toxicol. 2014 Jan;63:161-5.
339. Kwon-Chung KJ, Sugui JA. What do we know about the role of gliotoxin in the pathobiology of Aspergillus fumigatus? Med Mycol. 2009;47 Suppl 1(Suppl 1):S97-103.
340. Scharf DH, Heinekamp T, Remme N, Hortschansky P, Brakhage AA, Hertweck C. Biosynthesis and function of gliotoxin in Aspergillus fumigatus. Appl Microbiol Biotechnol. 2012 Jan;93(2):467-72.
341. Scharf DH, Brakhage AA, Mukherjee PK. Gliotoxin--bane or boon? Environ Microbiol. 2016 Apr;18(4):1096-109.
342. Mitchell NJ, Marroquín-Cardona AG, Romoser A, Phillips TD, Hayes AW. Mycotoxins. Ref Module Biomed Sci. 2014 https://doi.org/10.1016/B978-0-12-801238-3.00135-5 (accessed November 18, 2024).
343. Siddiquee S. Recent advancements on the role and analysis of volatile compounds (VOCs) from Trichoderma. In: Gupta VK, Schmoll M, Herrera-Estrella A, Upadhyay RS, Druzhinina I, Tuohy MG, Editors. Biotechnology and biology of Trichoderma. London: Elsevier; 2014. p. 139-175.
344. Pratt-Hyatt M. Mycotoxin Exposure: Assessment and Treatment. In: Pizzorno JE, Murray MT, Editors. Textbook of Natural Medicine. 5th ed. London: Churchill Livingstone; 2020. p. 1026-34.
345. Waring P, Eichner RD, Müllbacher A. The chemistry and biology of the immunomodulating agent gliotoxin and related epipolythiodioxopiperazines. Med Res Rev. 1988 Oct-Dec;8(4):499-524.
346. Waring P, Eichner RD, Müllbacher A, Sjaarda A. Gliotoxin induces apoptosis in macrophages unrelated to its antiphagocytic properties. J Biol Chem. 1988 Dec 5;263(34):18493-9.
347. Taylor A. The toxicology of sporidesmins and other epipolythiadioxopiperazines. Microbial Toxins. 1971;7:337-76.
348. Sutton P, Newcombe NR, Waring P, Müllbacher A. In vivo immunosuppressive activity of gliotoxin, a metabolite produced by human pathogenic fungi. Infect Immun. 1994 Apr;62(4):1192-8.
349. Waring P, Beaver J. Gliotoxin and related epipolythiodioxopiperazines. Gen Pharmacol. 1996 Dec;27(8):1311-6.
350. Gardiner DM, Waring P, Howlett BJ. The epipolythiodioxopiperazine (ETP) class of fungal toxins: distribution, mode of action, functions and biosynthesis. Microbiology. 2005 Apr;151(4):1021-32.
351. Pahl HL, Krauss B, Schulze-Osthoff K, Decker T, Traenckner EM, Vogt M, et al. The immunosuppressive fungal metabolite gliotoxin specifically inhibits transcription factor NF-kappaB. The Journal of Experimental Medicine. 1996 Apr 1;183(4):1829-40.
352. Schlam D, Canton J, Carreño M, Kopinski H, Freeman SA, Grinstein S, et al. Gliotoxin Suppresses Macrophage Immune Function by Subverting Phosphatidylinositol 3,4,5-Trisphosphate Homeostasis. mBio. 2016 Apr 5;7(2):e02242.
353. Amitani R, Murayama T, Nawada R, Lee WJ, Niimi A, Suzuki K, et al. Aspergillus culture filtrates and sputum sols from patients with pulmonary aspergillosis cause damage to human respiratory ciliated epithelium in vitro. Eur Respir J. 1995 Oct;8(10):1681-7.
354. Amitani R, Taylor G, Elezis EN, Llewellyn-Jones C, Mitchell J, Kuze F,et al. Purification and characterization of factors produced by Aspergillus fumigatus which affect human ciliated respiratory epithelium. Infect Immun. 1995 Sep;63(9):3266-71.
355. Amitani R, Kawanami R. Interaction of Aspergillus with human respiratory mucosa: a study with organ culture model. Med Mycol. 2009;47 Suppl 1:S127-31.
356. Dagenais TR, Keller NP. Pathogenesis of Aspergillus fumigatus in Invasive Aspergillosis. Clin Microbiol Rev. 2009 Jul;22(3):447-65.
357. Denning DW. Invasive aspergillosis. Clin Infect Dis. 1998 Apr;26(4):781-803; quiz 804-5.
358. Reeves EP, Messina CG, Doyle S, Kavanagh K. Correlation between gliotoxin production and virulence of Aspergillus fumigatus in Galleria mellonella. Mycopathologia. 2004 Jul;158(1):73-9.
359. Ben-Ami R, Lewis RE, Leventakos K, Kontoyiannis DP. Aspergillus fumigatus inhibits angiogenesis through the production of gliotoxin and other secondary metabolites. Blood. 2009 Dec 17;114(26):5393-9.
360. Lin SJ, Schranz J, Teutsch SM. Aspergillosis case-fatality rate: systematic review of the literature. Clin Infect Dis. 2001 Feb 1;32(3):358-66.
361. Bakare N, Rickerts V, Bargon J, Just-Nübling G. Prevalence of Aspergillus fumigatus and other fungal species in the sputum of adult patients with cystic fibrosis. Mycoses. 2003 Feb;46(1-2):19-23.
362. Hauser AR, Jain M, Bar-Meir M, McColley SA. Clinical significance of microbial infection and adaptation in cystic fibrosis. Clin Microbiol Rev. 2011 Jan;24(1):29-70.
363. Holt CD. Overview of Immunosuppressive Therapy in Solid Organ Transplantation. Anesthesiol Clin. 2017 Sep;35(3):365-80.
364. Takahashi K, Go P, Stone CH, Safwan M, Putchakayala KG, Kane WJ, et al. Mycophenolate Mofetil and Pulmonary Fibrosis After Kidney Transplantation: A Case Report. Am J Case Rep. 2017 Apr 14;18:399-404.
365. Xu ZN, Yang ST. Production of mycophenolic acid by Penicillium brevicompactum immobilized in a rotating fibrous-bed bioreactor. Enzyme and Microbial Technology. 2007 Mar 5;40(4):623-8.
366. Jonsson CA, Carlsten H. Mycophenolic acid inhibits inosine 5'-monophosphate dehydrogenase and suppresses immunoglobulin and cytokine production of B cells. Int Immunopharmacol. 2003 Jan;3(1):31-7.
367. El-Banna AA, Pitt JI, Leistner L. Production of mycotoxins by Penicillium species. Systematic and Applied Microbiology. 1987 Nov 1;10(1):42-6.
368. Overy DP, Frisvad JC. Mycotoxin production and postharvest storage rot of ginger (Zingiber officinale) by Penicillium brevicompactum. Journal of Food Protection. 2005 Mar 1;68(3):607-9.
369. WHO (World Health Organization). Evaluation of certain contaminants in food: Eighty-third report of the Joint FAO/WHO Expert Committee on Food Additives. WHO technical report series no. 1002. WHO and the Food and Agriculture Organization of the United Nations (FAO), Geniva. 2017. https://www.who.int/publications/i/item/9789241210027 (accessed November 18, 2024).
370. Bullingham R, Monroe S, Nicholls A, Hale M. Pharmacokinetics and bioavailability of mycophenolate mofetil in healthy subjects after single-dose oral and intravenous administration. J Clin Pharmacol. 1996 Apr;36(4):315-24.
371. Bernard O, Guillemette C. The main role of UGT1A9 in the hepatic metabolism of mycophenolic acid and the effects of naturally occurring variants. Drug Metab Dispos. 2004 Aug;32(8):775-8.
372. Picard N, Ratanasavanh D, Prémaud A, Le Meur Y, Marquet P. Identification of the UDP-glucuronosyltransferase isoforms involved in mycophenolic acid phase II metabolism. Drug Metab Dispos. 2005 Jan;33(1):139-46.
373. Staatz CE, Tett SE. Clinical pharmacokinetics and pharmacodynamics of mycophenolate in solid organ transplant recipients. Clin Pharmacokinet. 2007;46(1):13-58.
374. GASTON RS, AGARWAL G, MORRIS PJ. 15 Azathioprine and. Kidney Transplantation-Principles and Practice E-Book. 2019 Aug 31:212.
375. Choo SY. The HLA system: genetics, immunology, clinical testing, and clinical implications. Yonsei Med J. 2007 Feb 28;48(1):11-23.
376. Gehlot P, Holoshitz J. HLA and Autoimmunity. In: Ratcliffe MJH, Editor. Encyclopedia of Immunobiology. London: Academic Press; 2016. p. 297-303.
377. Nakamura T, Shirouzu T, Nakata K, Yoshimura N, Ushigome H. The Role of Major Histocompatibility Complex in Organ Transplantation- Donor Specific Anti-Major Histocompatibility Complex Antibodies Analysis Goes to the Next Stage. Int J Mol Sci. 2019 Sep 13;20(18):4544.
378. Tumer G, Simpson B, Roberts TK. Genetics, Human Major Histocompatibility Complex (MHC). In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024.
379. Hanada K, Yewdell JW, Yang JC. Immune recognition of a human renal cancer antigen through post-translational protein splicing. Nature. 2004 Jan 15;427(6971):252-6.
380. Creppy EE. Human ochratoxicosis. J Toxicol Toxin Rev. 1999 Jan 1;18(3-4):277-93.
381. Hult K, Pleština R, Habazin-Novak V, Radić B, Čeović S. Ochratoxin A in human blood and Balkan endemic nephropathy. Archives of Toxicology. 1982 Dec;51:313-21.
382. Castegnaro M, Bartsch H, Chernozemsky I. Endemic nephropathy and urinary tract tumors in the Balkans. Cancer Res. 1987;47:3606-9.
383. Krogh P. Ochratoxin in Foods. In: Krogh P, Editor. Mycotoxins in Food. London: Academic Press; 1987. p. 97-110.
384. Schwartz GG. Hypothesis: does ochratoxin A cause testicular cancer? Cancer Causes Control. 2002 Feb;13(1):91-100.
385. Kuiper-Goodman T, Scott PM. Risk assessment of the mycotoxin ochratoxin A. Biomed Environ Sci. 1989 Sep;2(3):179-248.
386. Beardall JM, Miller JD. Disease in humans with mycotoxins as possible causes. In: Miller JD, Trenholm HL, Editors. Mycotoxins in grains: Compounds other than aflatoxin. St. Paul, Minn: Eagan Press; 1994. p. 487-539.
387. Bunge I, Heller K, Roschenthaler R. Isolation and purification of ochratoxin A. Z Lebensm Unters Forsch. 1979;168:457-8.
388. Meisner H, Meisner P. Ochratoxin A, an in vivo inhibitor of renal phosphoenolpyruvate carboxykinase. Arch Biochem Biophys. 1981 Apr 15;208(1):146-53.
389. Rahimtula AD, Béréziat JC, Bussacchini-Griot V, Bartsch H. Lipid peroxidation as a possible cause of ochratoxin A toxicity. Biochem Pharmacol. 1988 Dec 1;37(23):4469-77.
390. Dirheimer G, Creppy EE. Mechanism of action of ochratoxin A. IARC Sci Publ. 1991;(115):171-86.
391. Marquardt RR, Frohlich AA. A review of recent advances in understanding ochratoxicosis. J Anim Sci. 1992 Dec;70(12):3968-88.
392. Pfohl-Leszkowicz A, Grosse Y, Castegnaro M, Nicolov IG, Chernozemsky IN, Bartsch H, et al. Ochratoxin A-related DNA adducts in urinary tract tumours of Bulgarian subjects. IARC Sci Publ. 1993;(124):141-8.
393. Hassen W, Abid S, Achour A, Creppy E, Bacha H. Ochratoxin A and beta2-microglobulinuria in healthy individuals and in chronic interstitial nephropathy patients in the centre of Tunisia: a hot spot of Ochratoxin A exposure. Toxicology. 2004 Jul 1;199(2-3):185-93.
394. Ringot D, Chango A, Schneider YJ, Larondelle Y. Toxicokinetics and toxicodynamics of ochratoxin A, an update. Chem Biol Interact. 2006 Jan 5;159(1):18-46.
395. Gil-Serna J, Vázquez C, González-Jaén MT, Patiño B. Mycotoxins: toxicology. In: Batt CA, Tortorello ML, Editors. Encyclopedia of Food Microbiology. 2nd ed. London: Academic Press; 2014. p. 887-92.
396. Kőszegi T, Poór M. Ochratoxin A: Molecular Interactions, Mechanisms of Toxicity and Prevention at the Molecular Level. Toxins (Basel). 2016 Apr 15;8(4):111.
397. Soto JB, Ruiz MJ, Manyes L, Juan-García A. Blood, breast milk and urine: potential biomarkers of exposure and estimated daily intake of ochratoxin A: a review. Food Addit Contam Part A Chem Anal Control Expo Risk Assess. 2016;33(2):313-28.
398. Minervini F, Giannoccaro A, Nicassio M, Panzarini G, Lacalandra GM. First evidence of placental transfer of ochratoxin A in horses. Toxins (Basel). 2013 Jan 11;5(1):84-92.
399. Galtier P, Alvinerie M, Charpenteau JL. The pharmacokinetic profiles of ochratoxin A in pigs, rabbits and chickens. Food Cosmet Toxicol. 1981 Dec;19(6):735-8.
400. Hagelberg S, Hult K, Fuchs R. Toxicokinetics of ochratoxin A in several species and its plasma-binding properties. J Appl Toxicol. 1989 Apr;9(2):91-6.
401. Studer-Rohr I, Schlatter J, Dietrich DR. Kinetic parameters and intraindividual fluctuations of ochratoxin A plasma levels in humans. Arch Toxicol. 2000 Nov;74(9):499-510.
402. Stander MA, Nieuwoudt TW, Steyn PS, Shephard GS, Creppy EE, Sewram V. Toxicokinetics of ochratoxin A in vervet monkeys (Cercopithecus aethiops). Arch Toxicol. 2001 Jul;75(5):262-9.
403. Zepnik H, Völkel W, Dekant W. Toxicokinetics of the mycotoxin ochratoxin A in F 344 rats after oral administration. Toxicol Appl Pharmacol. 2003 Oct 1;192(1):36-44.
404. Dietrich DR, Heussner AH, O'Brien E. Ochratoxin A: comparative pharmacokinetics and toxicological implications (experimental and domestic animals and humans). Food Addit Contam. 2005;22 Suppl 1:45-52.
405. Elling F. Ochratoxin A-induced mycotoxic porcine nephropathy: alterations in enzyme activity in tubular cells. Acta Pathol Microbiol Scand A. 1979 Jul;87A(4):237-43.
406. Jelinek CF, Pohland AE, Wood GE. Worldwide occurrence of mycotoxins in foods and feeds--an update. J Assoc Off Anal Chem. 1989 Mar-Apr;72(2):223-30.
407. Olsen M, Thorup I, Knudsen I, Larsen JJ, Hald B, Olsen J. Health evaluation of ochratoxin A in food products. Nordic Working Group on Food Toxicology and Risk Evaluation. Nordic Council of Ministers, Report No 545. Copenhagen, Denmark.(1991)
408. Van Egmond HP. Worldwide regulations for ochratoxin A. IARC Scientific Publications. 1991 Jan 1(115):331-6.
409. Sweeney MJ, White S, Dobson AD. Mycotoxins in agriculture and food safety. Irish Journal of Agricultural and Food Research. 2000 Jan 1:235-44.
410. European Food Safety Authority (EFSA). Opinion of the Scientific Panel on contaminants in the food chain [CONTAM] related to ochratoxin A in food. EFSA Journal. 2006 Jun;4(6):365.
411. van Egmond HP, Schothorst RC, Jonker MA. Regulations relating to mycotoxins in food: perspectives in a global and European context. Anal Bioanal Chem. 2007 Sep;389(1):147-57.
412. WHO (Word Health Organization). Evaluation of certain food additives and contaminants: Sixty-eighth report of the Joint FAO/WHO Expert Committee on Food Additives. WHO Technical Report Series. 2007. 947. https://www.who.int/publications/i/item/9789241209472 (accessed November 18, 2024).
413. Kuiper-Goodman T, Hilts C, Billiard SM, Kiparissis Y, Richard ID, Hayward S. Health risk assessment of ochratoxin A for all age-sex strata in a market economy. Food Addit Contam Part A Chem Anal Control Expo Risk Assess. 2010 Feb;27(2):212-40.
414. Zingales V, Fernández-Franzón M, Ruiz MJ. Sterigmatocystin: Occurrence, toxicity and molecular mechanisms of action - A review. Food Chem Toxicol. 2020 Dec;146:111802
415. Purchase IF, van der Watt JJ. Acute toxicity of sterigmatocystin to rats. Food Cosmet Toxicol. 1969 Mar;7(2):135-9.
416. Liu Y, Xing X, Wang J, Xing L, Su Y, Yao Z, et al. Sterigmatocystin alters the number of FoxP3+ regulatory T cells and plasmacytoid dendritic cells in BALB/c mice. Food Chem Toxicol. 2012 Jun;50(6):1920-6.
417. Zhang Y, Yao ZG, Wang J, Xing LX, Xia Y, Zhang XH. Effects of sterigmatocystin on TNF-α, IL-6 and IL-12 expression in murine peripheral blood mononuclear cells and peritoneal macrophages in vivo. Mol Med Rep. 2012 May;5(5):1318-22.
418. Lou J, Tian H, Meng Z, Gou Z. Detection of sterigmatocystin in food/feed samples from area with various liver/stomach cancer incidences by enzyme-linked immuneabsorbent assay. Wei Sheng Yan Jiu/Journal Hyg. Res. 1995;2:28-31.
419. Tian H, Lou J, Du C. [Determination of sterigmatocystin in cancerous tissues, blood and urine in patients with liver and stomach cancer]. Zhonghua Yu Fang Yi Xue Za Zhi. 1995 Sep;29(5):276-8.
420. Zhang X, Wang F, Wang J, Yan X, Huang X, Xie T, et al. [Experimental lung carcinoma induced by fungi and mycotoxins--a review]. Beijing Da Xue Xue Bao Yi Xue Ban. 2003 Feb 18;35(1):4-6.
421. Cao X, Li X, Li J, Niu Y, Shi L, Fang Z, et al. Quantitative determination of carcinogenic mycotoxins in human and animal biological matrices and animal-derived foods using multi-mycotoxin and analyte-specific high performance liquid chromatography-tandem mass spectrometric methods. J Chromatogr B Analyt Technol Biomed Life Sci. 2018 Jan 15;1073:191-200.
422. Purchase IF, Van Der Watt JJ. Carcinogenicity of sterigmatocystin. Food Cosmet Toxicol. 1970 Jun;8(3):289-95.
423. Purchase IF, Van der Watt JJ. Carcinogenicity of sterigmatocystin to rat skin. Toxicol Appl Pharmacol. 1973 Oct;26(2):274-81.
424. Fujii K, Kurata H, Odashima S, Hatsuda Y. Tumor induction by a single subcutaneous injection of sterigmatocystin in newborn mice. Cancer Res. 1976 May;36(5):1615-8.
425. Huang XH, Zhang XH, Li YH, Wang JL, Yan X, Xing LX, et al. [Carcinogenic effects of sterigmatocystin and deoxynivalenol in NIH mice]. Zhonghua Zhong Liu Za Zhi. 2004 Dec;26(12):705-8.
426. Kusunoki M, Misumi J, Shimada T, Aoki K, Matsuo N, Sumiyoshi H, et al. Long-term administration of the fungus toxin, sterigmatocystin, induces intestinal metaplasia and increases the proliferative activity of PCNA, p53, and MDM2 in the gastric mucosa of aged Mongolian gerbils. Environ Health Prev Med. 2011 Jul;16(4):224-31.
427. International Agency for Research on Cancer. Overall Evaluations of Carcinogenicity: an Updating of IARC Monographs (vols 1-42). IARC monographs on the evaluation of carcinogenic risks to humans. 1987.
428. Cole RA, Jarvis BB, Schweikert MA. Handbook of Secondary Metabolites. New York: Academic Press; 2003. p. 199-560.
429. Fujimoto H. Yeasts and Molds | Mycotoxins: Classification, Occurrence and Determination. In: Fuquay JW, Editors. Encyclopedia of Dairy Sciences. 2nd ed. New York: Academic Press; 2011. p. 792-800.
430. Wu Q, Huang L, Liu Z, Yao M, Wang Y, Dai M, et al. A comparison of hepatic in vitro metabolism of T-2 toxin in rats, pigs, chickens, and carp. Xenobiotica. 2011 Oct;41(10):863-73.
431. Suneja SK, Wagle DS, Ram GC. Effect of oral administration of T-2 toxin on glutathione shuttle enzymes, microsomal reductases and lipid peroxidation in rat liver. Toxicon. 1989;27(9):995-1001.
432. Riley RT, Norred WP. Mechanisms of mycotoxicity. In: Howard DH, Miller JD, Editors. Human and Animal Relationships. Berlin, Heidelberg: Springer Berlin Heidelberg; 1996. p. 193-211.
433. Ueno Y. Mode of action of trichothecenes. Ann Nutr Aliment. 1977;31(4-6):885-900.
434. Ueno Y. Toxicological features of T-2 toxin and related trichothecenes. Fundam Appl Toxicol. 1984 Apr;4(2 Pt 2):S124-32.
435. McCormick SP, Stanley AM, Stover NA, Alexander NJ. Trichothecenes: from simple to complex mycotoxins. Toxins (Basel). 2011 Jul;3(7):802-14.
436. Altomare C, Logrieco A, Bottalico A, Mulé G, Moretti A, Evidente A. Production of type A trichothecenes and enniatin B by Fusarium sambucinum Fuckel sensu lato. Mycopathologia. 1995;129(3):177-81.
437. Garvey GS, McCormick SP, Rayment I. Structural and functional characterization of the TRI101 trichothecene 3-O-acetyltransferase from Fusarium sporotrichioides and Fusarium graminearum: kinetic insights to combating Fusarium head blight. Journal of Biological Chemistry. 2008 Jan 18;283(3):1660-9.
438. Gottschalk C, Barthel J, Engelhardt G, Bauer J, Meyer K. Simultaneous determination of type A, B and D trichothecenes and their occurrence in cereals and cereal products. Food Additives and Contaminants. 2009 Sep 1;26(9):1273-89.
439. Pestka JJ, Forsell JH. Inhibition of human lymphocyte transformation by the macrocyclic trichothecenes roridin A and verrucarin A. Toxicol Lett. 1988 Jun;41(3):215-22.
440. WHO (World Health Organization). Selected mycotoxins: Ochratoxins, trichothecenes, ergot - Environmental Health Criteria 105. United Nations Environment Programme, International Programme on Chemical Safety, WHO, Geneva. 1990. https://wedocs.unep.org/20.500.11822/29486 (accessed November 18, 2024).
441. Wannemacher RW, Wiener SL, Sidell FR, Takafuji ET, Franz DR. Trichothecene mycotoxins. Medical aspects of chemical and biological warfare. 1997;6:655-76.
442. Islam Z, Shinozuka J, Harkema JR, Pestka JJ. Purification and comparative neurotoxicity of the trichothecenes satratoxin G and roridin L2 from Stachybotrys chartarum. J Toxicol Environ Health A. 2009;72(20):1242-51.
443. Bae HK, Pestka JJ. Deoxynivalenol induces p38 interaction with the ribosome in monocytes and macrophages. Toxicol Sci. 2008 Sep;105(1):59-66.
444. Nusuetrong P, Pengsuparp T, Meksuriyen D, Tanitsu M, Kikuchi H, Mizugaki M, et al. Satratoxin H generates reactive oxygen species and lipid peroxides in PC12 cells. Biol Pharm Bull. 2008 Jun;31(6):1115-20.
445. Pestka JJ. Mechanisms of deoxynivalenol-induced gene expression and apoptosis. Food Addit Contam Part A Chem Anal Control Expo Risk Assess. 2008 Sep;25(9):1128-40.
446. Barel S, Yagen B, Bialer M. Pharmacokinetics of the trichothecene mycotoxin verrucarol in dogs. J Pharm Sci. 1990 Jun;79(6):548-51.
447. Gromadzka K, Waskiewicz A, Chelkowski J, Golinski P. Zearalenone and its metabolites: occurrence, detection, toxicity and guidelines. World Mycotoxin Journal. 2008 May 1;1(2):209-20.
448. Ropejko K, Twarużek M. Zearalenone and Its Metabolites-General Overview, Occurrence, and Toxicity. Toxins (Basel). 2021 Jan 6;13(1):35.
449. Tassis PD, Tsakmakidis IA, Nagl V, Reisinger N, Tzika E, Gruber-Dorninger C, et al. Individual and Combined In Vitro Effects of Deoxynivalenol and Zearalenone on Boar Semen. Toxins (Basel). 2020 Aug 1;12(8):495.
450. Zinedine A, Soriano JM, Moltó JC, Mañes J. Review on the toxicity, occurrence, metabolism, detoxification, regulations and intake of zearalenone: an oestrogenic mycotoxin. Food Chem Toxicol. 2007 Jan;45(1):1-18.
451. De Santis B, Raggi ME, Moretti G, Facchiano F, Mezzelani A, Villa L, et al. Study on the Association among Mycotoxins and other Variables in Children with Autism. Toxins (Basel). 2017 Jun 29;9(7):203.
452. EFSA Panel on Contaminants in the Food Chain. Scientific Opinion on the risks for public health related to the presence of zearalenone in food. EFSA Journal. 2011 Jun;9(6):2197.
453. Kovalsky Paris MP, Schweiger W, Hametner C, Stückler R, Muehlbauer GJ, Varga E, et al. Zearalenone-16-O-glucoside: a new masked mycotoxin. J Agric Food Chem. 2014 Feb 5;62(5):1181-9.
454. Mally A, Solfrizzo M, Degen GH. Biomonitoring of the mycotoxin Zearalenone: current state-of-the art and application to human exposure assessment. Arch Toxicol. 2016 Jun;90(6):1281-92.
455. Rai A, Das M, Tripathi A. Occurrence and toxicity of a fusarium mycotoxin, zearalenone. Crit Rev Food Sci Nutr. 2020;60(16):2710-29.
456. Fianchi F, Liguori A, Gasbarrini A, Grieco A, Miele L. Nonalcoholic Fatty Liver Disease (NAFLD) as Model of Gut-Liver Axis Interaction: From Pathophysiology to Potential Target of Treatment for Personalized Therapy. Int J Mol Sci. 2021 Jun 17;22(12):6485.
457. Szabo G, Romics L Jr, Frendl G. Liver in sepsis and systemic inflammatory response syndrome. Clin Liver Dis. 2002 Nov;6(4):1045-66.
458. Wynn TA, Barron L. Macrophages: master regulators of inflammation and fibrosis. Semin Liver Dis. 2010 Aug;30(3):245-57.
459. Kanel GC. Part II - Liver Biopsy Evaluation: Morphology with Differential Diagnoses. In: Kanel GC, Editors. Atlas of Liver Pathology. 4th ed. Netherlands: Elsevier; 2024. p. 515-60.
460. Fung F, Clark RF. Health effects of mycotoxins: a toxicological overview. J Toxicol Clin Toxicol. 2004;42(2):217-34.
461. Liu J, Tan Y, Cheng H, Zhang D, Feng W, Peng C. Functions of Gut Microbiota Metabolites, Current Status and Future Perspectives. Aging Dis. 2022 Jul 11;13(4):1106-26.
462. Martins IJ. Overnutrition Determines LPS Regulation of Mycotoxin Induced Neurotoxicity in Neurodegenerative Diseases. Int J Mol Sci. 2015 Dec 10;16(12):29554-73.
463. Guerre P. Mycotoxin and Gut Microbiota Interactions. Toxins (Basel). 2020 Dec 4;12(12):769.
464. Sharma A, Martins IJ. The role of Microbiota in the Pathogenesis of Alzheimer’s Disease. Acta Scientific Nutritional Health. 2023 Jul;7(7).
465. Pritchard AB, Crean S, Olsen I, Singhrao SK. Periodontitis, Microbiomes and their Role in Alzheimer's Disease. Front Aging Neurosci. 2017 Oct 24;9:336.
466. Giau VV, Wu SY, Jamerlan A, An SSA, Kim SY, Hulme J. Gut Microbiota and Their Neuroinflammatory Implications in Alzheimer's Disease. Nutrients. 2018 Nov 14;10(11):1765.
467. Emery DC, Shoemark DK, Batstone TE, Waterfall CM, Coghill JA, Cerajewska TL, et al. 16S rRNA Next Generation Sequencing Analysis Shows Bacteria in Alzheimer's Post-Mortem Brain. Front Aging Neurosci. 2017 Jun 20;9:195.
468. Daniel W. Modified Nanoparticles for Lipophilic Toxin Sequestration. Published on The Small Business Innovation Research (SBIR) and Small Business Technology Transfer (STTR) programs website. 2011. (https://legacy.www.sbir.gov/about) (accessed on November 18, 2024).
469. Martins I. Bacterial lipopolysaccharides and neuron toxicity in neurodegenerative diseases. Neurol Res Surgery. 2018;1:1-3.
470. Tang W, Zhu H, Feng Y, Guo R, Wan D. The Impact of Gut Microbiota Disorders on the Blood-Brain Barrier. Infect Drug Resist. 2020 Sep 29;13:3351-63.
471. An L, Wirth U, Koch D, Schirren M, Drefs M, Koliogiannis D, et al. The Role of Gut-Derived Lipopolysaccharides and the Intestinal Barrier in Fatty Liver Diseases. J Gastrointest Surg. 2022 Mar;26(3):671-83.
472. Viljoen M, Claassen N. Pathophysiological aspects of exposure to dampness-associated indoor mould and mycotoxins: A mini-overview. Journal of Hazardous Materials Advances. 2023 Feb 1;9:100228.
473. Lehman-McKeeman LD. ∝2u-Globulin Nephropathy. In: Sipes IG, McQueen CA, Gandolfi AJ, Editors. Comprehensive Toxicology, Vol 7. Oxford: Elsevier; 1997. p. 677-92.
474. NRC (National Research Council). Appendix A, Values and Limitations of Animal Toxicity Data. In, Intentional Human Dosing Studies for EPA Regulatory Purposes: Scientific and Ethical Issues. Committee on the Use of Third Party Toxicity Research with Human Research Participants. National Academies Press, Washington, DC, 2004. https://www.ncbi.nlm.nih.gov/books/NBK215893/ (accessed November 18, 2024).
475. Borchers A, Teuber SS, Keen CL, Gershwin ME. Food safety. Clin Rev Allergy Immunol. 2010 Oct;39(2):95-141.
476. Flemming J, Hudson B, Rand TG. Comparison of inflammatory and cytotoxic lung responses in mice after intratracheal exposure to spores of two different Stachybotrys chartarum strains. Toxicol Sci. 2004 Apr;78(2):267-75.
477. Meklin T, Reponen T, McKinstry C, Cho SH, Grinshpun SA, Nevalainen A, et al. Comparison of mold concentrations quantified by MSQPCR in indoor and outdoor air sampled simultaneously. Sci Total Environ. 2007 Aug 15;382(1):130-4.
478. Creppy EE. Update of survey, regulation and toxic effects of mycotoxins in Europe. Toxicol Lett. 2002 Feb 28;127(1-3):19-28.
479. Schothorst RC, van Egmond HP. Report from SCOOP task 3.2.10 "collection of occurrence data of Fusarium toxins in food and assessment of dietary intake by the population of EU member states". Subtask: trichothecenes. Toxicol Lett. 2004 Oct 10;153(1):133-43.
480. Rasmussen RR. Restindhold af malakitgrønt i dambrugsfisk. Dansk Kemi. 2007;88(1):39-41.
481. Hawksworth DL. The fungal dimension of biodiversity: magnitude, significance, and conservation. Mycological Research. 1991 Jun 1;95(6):641-55.
482. O'Brien HE, Parrent JL, Jackson JA, Moncalvo JM, Vilgalys R. Fungal community analysis by large-scale sequencing of environmental samples. Appl Environ Microbiol. 2005 Sep;71(9):5544-50.
483. Enoch DA, Yang H, Aliyu SH, Micallef C. The Changing Epidemiology of Invasive Fungal Infections. Methods Mol Biol. 2017;1508:17-65.
484. Bodis G, Toth V, Schwarting A. Role of Human Leukocyte Antigens (HLA) in Autoimmune Diseases. Rheumatol Ther. 2018 Jun;5(1):5-20.
485. U.S. EPA (United States Environmental Protection Agency). Climate Change Indicators: Heavy Precipitation. 2024. https://www.epa.gov/climate-indicators/climate-change-indicators-heavy-precipitation#ref1 (accessed, November 18, 2024).
486. Knutsen AP, Bush RK, Demain JG, Denning DW, Dixit A, Fairs A, et al. Fungi and allergic lower respiratory tract diseases. J Allergy Clin Immunol. 2012 Feb;129(2):280-91; quiz 292-3.
487. Bell JE, Herring SC, Jantarasami L, Adrianopoli C, Benedict K, Conlon K, et al. Impacts of extreme events on human health. In: The impacts of climate change on human health in the United States: U.S. Global Change Research Program, Washington, DC; 2016. pp.99–128. Available from: https://health2016.globalchange.gov/extreme-events (accessed November 18, 2024).
488. Zandalinas SI, Fritschi FB, Mittler R. Global Warming, Climate Change, and Environmental Pollution: Recipe for a Multifactorial Stress Combination Disaster. Trends Plant Sci. 2021 Jun;26(6):588-99.
489. Marvel K, Su W, Delgado R, Aarons S, Chatterjee A, Garcia ME, et al. Chapter 2: Climate Trends. In USGCRP (U.S. Global Change Research Program), Fifth National Climate Assessment. 2023. https://nca2023.globalchange.gov/chapter/2/ (accessed November 18, 2024).
490. Alothman AF, Althaqafi AO, Matar MJ, Moghnieh R, Alenazi TH, Farahat FM, et al. Burden and treatment patterns of invasive fungal infections in hospitalized patients in the Middle East: real-world data from Saudi Arabia and Lebanon. Infect Drug Resist. 2017 Feb 2;10:35-41.
491. Rayens E, Norris KA. Prevalence and Healthcare Burden of Fungal Infections in the United States, 2018. Open Forum Infect Dis. 2022 Jan 10;9(1):ofab593.
492. AlMaghrabi RS, Al-Musawi T, Albaksami O, Subhi AL, Fakih RE, Stone NR. Challenges in the Management of Invasive Fungal Infections in the Middle East: Expert Opinion to Optimize Management Using a Multidisciplinary Approach. Cureus. 2023 Aug 30;15(8):e44356.