Abstract
Pancreatic cancer, predominantly pancreatic ductal adenocarcinoma (PDAC), remains one of the most lethal malignancies, characterized by late diagnosis, aggressive tumor biology, and profound resistance to conventional therapies. Despite advances in surgical techniques and combination chemotherapy regimens such as FOLFIRINOX and gemcitabine-based therapies, survival outcomes remain poor, with five-year survival rates barely exceeding 10%. Recent progress in molecular oncology has provided critical insights into the genomic landscape of PDAC, highlighting key driver mutations, particularly in KRAS, as well as alterations in tumor suppressor genes including TP53, CDKN2A, and SMAD4. These discoveries have catalyzed the development of precision oncology approaches aimed at tailoring treatment based on individual tumor biology. Emerging therapeutic strategies include direct targeting of KRAS mutations, exploitation of DNA damage repair deficiencies using PARP inhibitors, and the integration of biomarker-driven treatment selection. Concurrently, novel diagnostic modalities such as liquid biopsy and exosome-based biomarkers offer non-invasive methods for real-time disease monitoring and early detection. Advances in artificial intelligence and multi-omics integration further enhance the ability to interpret complex biological data and guide personalized therapeutic decisions. This Narrative review synthesizes current evidence on the molecular drivers of pancreatic cancer and explores emerging precision oncology strategies, emphasizing the transition from conventional treatment paradigms toward adaptive, biomarker-guided approaches. The integration of molecular diagnostics, targeted therapies, and computational tools represents a promising pathway toward improving clinical outcomes in this highly aggressive disease.
Keywords
Pancreatic ductal adenocarcinoma (PDAC), Precision oncology, KRAS mutations, Liquid biopsy, Tumor microenvironment
Abbreviations
BRCA: Breast Cancer gene; CDKN2A: Cyclin-Dependent Kinase Inhibitor 2A; ctDNA: Circulating Tumor DNA; DNA: Deoxyribonucleic Acid; EMT : Epithelial-to-Mesenchymal Transition; FOLFIRINOX: Folinic acid, Fluorouracil, Irinotecan, and Oxaliplatin regimen; KRAS: Kirsten Rat Sarcoma viral oncogene homolog; MAPK: Mitogen-Activated Protein Kinase; PDAC : Pancreatic Ductal Adenocarcinoma; PARP: Poly (ADP-Ribose) polymerase; PI3K–AKT: Phosphoinositide 3-kinase–Protein kinase B pathway; TP53: Tumor Protein p53
Introduction
Pancreatic cancer remains one of the most aggressive and therapeutically challenging malignancies in contemporary oncology. Pancreatic ductal adenocarcinoma (PDAC), which accounts for the vast majority of pancreatic tumors, is characterized by rapid progression, early metastatic dissemination, and profound resistance to conventional therapies. Despite representing a smaller proportion of global cancer incidence, pancreatic cancer contributes disproportionately to cancer-related mortality and is projected to become one of the leading causes of cancer death in many regions within the next decade [1]. Current epidemiological estimates indicate that the five-year overall survival rate remains approximately 10–12%, reflecting only modest improvements over recent decades despite significant advances in oncologic care [2].
Several factors contribute to the poor prognosis associated with pancreatic cancer. The majority of patients present with locally advanced or metastatic disease at the time of diagnosis, rendering them ineligible for potentially curative surgical resection. Even among patients who undergo surgery, recurrence rates remain high due to the biologically aggressive nature of PDAC and the presence of micro metastatic disease at diagnosis [3]. Over the past decade, combination chemotherapy regimens such as FOLFIRINOX and gemcitabine combined with nab-paclitaxel have improved survival outcomes compared with earlier treatment protocols; however, these therapies remain limited by toxicity and the intrinsic chemoresistance of pancreatic tumors [4]. In addition, the highly desmoplastic tumor microenvironment characteristic of PDAC acts as a biological barrier to drug penetration and immune cell infiltration, further complicating therapeutic efforts [5].
In response to these challenges, recent research has increasingly focused on integrating multidisciplinary treatment strategies that combine surgical innovation, systemic therapy, and emerging diagnostic technologies. Minimally invasive pancreatic surgery, advances in perioperative management, and evolving ablative techniques have expanded the potential role of surgical intervention in selected patients [6]. At the same time, progress in molecular oncology has begun to reveal the complex genomic landscape of pancreatic cancer, highlighting the importance of oncogenic drivers such as KRAS mutations and alterations in DNA damage repair pathways [7]. These discoveries have stimulated growing interest in the development of molecularly targeted therapies and personalized treatment strategies aimed at improving outcomes in this highly lethal disease.
Molecular Drivers and Emerging Precision Oncology Strategies
The expanding understanding of pancreatic cancer genomics has provided critical insight into the biological mechanisms underlying disease progression and therapeutic resistance. Large-scale genomic analyses have demonstrated that PDAC is characterized by a limited number of dominant driver mutations, among which alterations in the KRAS oncogene are the most prevalent, occurring in more than 90% of cases [8]. KRAS mutations promote tumorigenesis through persistent activation of downstream signaling pathways, including the MAPK and PI3K–AKT cascades, which regulate cellular proliferation, metabolism, and survival. In addition to KRAS, recurrent alterations in tumor suppressor genes such as TP53, CDKN2A, and SMAD4 further contribute to genomic instability and aggressive tumor behavior [9]. These molecular alterations create a complex oncogenic network that drives tumor growth while simultaneously limiting the effectiveness of conventional cytotoxic therapies.
For many years, KRAS was widely regarded as an “undruggable” target due to its biochemical structure and high affinity for guanosine triphosphate, which complicated direct pharmacologic inhibition. Consequently, early therapeutic strategies focused on targeting downstream signaling pathways rather than the KRAS protein itself. However, these approaches achieved limited success because of pathway redundancy and adaptive resistance mechanisms within tumor cells [10]. More recently, advances in structure-based drug design have enabled the development of small-molecule inhibitors capable of selectively targeting specific KRAS mutant isoforms, representing a major breakthrough in precision oncology. Early clinical studies evaluating KRAS inhibitors, particularly those directed at the G12C mutation, have demonstrated encouraging antitumor activity in several solid malignancies, including pancreatic cancer [11]. Although KRAS G12C mutations occur less frequently in PDAC compared with other tumor types such as lung cancer, the development of inhibitors targeting additional variants including KRAS G12D and broader RAS signaling pathways has generated considerable optimism for expanding targeted therapeutic options in pancreatic cancer [12].
Beyond direct oncogenic targeting, the recognition of molecular heterogeneity within pancreatic cancer has further strengthened the rationale for precision medicine approaches. Subsets of patients harbor germline or somatic alterations in DNA damage repair genes such as BRCA1, BRCA2, and PALB2, which are associated with increased sensitivity to platinum-based chemotherapy and poly (ADP-ribose) polymerase (PARP) inhibitors [13]. These findings have led to the incorporation of germline genetic testing and molecular profiling into clinical practice guidelines for pancreatic cancer management. By identifying patients who may benefit from targeted therapies, genomic stratification has begun to reshape treatment algorithms and highlights the potential of individualized therapeutic strategies in a disease historically characterized by limited treatment options [14], with several emerging precision oncology strategies currently under active investigation (Table 1).
|
Therapeutic Strategy |
Molecular Target |
Clinical Relevance |
|
KRAS-targeted therapies |
KRAS G12C, G12D mutations |
Emerging targeted agents aimed at oncogenic KRAS signaling [10,13–15] |
|
DNA damage repair targeting |
BRCA1, BRCA2, PALB2 mutations |
Sensitivity to platinum-based chemotherapy and PARP inhibitors [16,17] |
|
Liquid biopsy monitoring |
Circulating tumor DNA (ctDNA), circulating tumor cells |
Non-invasive monitoring of tumor evolution and early recurrence [18,19] |
|
Exosome-based biomarkers |
Tumor-derived extracellular vesicles |
Potential early diagnostic and prognostic biomarkers [20,21] |
|
Artificial intelligence–driven multi-omics |
Genomic, transcriptomic and imaging data |
Integration of complex datasets for personalized treatment decisions [22] |
|
Tumor microenvironment (TME) targeting |
Stromal components, immune suppressive cells |
Combination strategies to overcome therapeutic resistance [7,23] |
While the identification of actionable genomic alterations represents a major advance in pancreatic cancer research, the successful implementation of precision oncology also requires diagnostic strategies capable of capturing the dynamic and heterogeneous nature of tumor biology [15]. Pancreatic tumors exhibit substantial intra- and intertumoral heterogeneity, reflecting the evolutionary pressures imposed by genetic instability, microenvironmental interactions, and therapeutic selection. Consequently, static tissue biopsies obtained at a single time point may not adequately represent the evolving genomic landscape of the disease. This limitation has stimulated increasing interest in minimally invasive diagnostic approaches capable of monitoring tumor evolution throughout the course of treatment [16].
Among these emerging technologies, liquid biopsy has gained considerable attention as a potential tool for real-time molecular profiling of pancreatic cancer. Circulating tumor DNA (ctDNA), circulating tumor cells, and extracellular vesicles released by tumor cells can be detected in peripheral blood and other biological fluids, providing valuable information regarding tumor genetics, clonal evolution, and therapeutic resistance. Several studies have demonstrated that ctDNA analysis can identify tumor-specific mutations including KRAS alterations with high specificity and may enable earlier detection of disease recurrence compared with conventional imaging modalities [17]. In addition to disease monitoring, liquid biopsy approaches may facilitate patient stratification for targeted therapies by identifying actionable genomic alterations without the need for repeated invasive tissue sampling [18].
Exosome-based diagnostics represent another promising component of this evolving diagnostic landscape. Exosomes are nanoscale extracellular vesicles secreted by tumor cells that carry diverse molecular cargo, including DNA fragments, messenger RNA, microRNA, and proteins. Because exosomes are abundant and stable in circulating body fluids, they offer an attractive platform for non-invasive cancer detection and biomarker discovery. Emerging evidence suggests that exosomal RNA and protein signatures derived from pancreatic tumors may provide sensitive markers for early disease detection and prognosis. Importantly, these vesicles also reflect the biological interactions between tumor cells and the surrounding microenvironment, offering insight into mechanisms that drive tumor progression and therapeutic resistance [19].
The integration of these molecular diagnostic tools with advances in computational biology is further accelerating the development of precision oncology frameworks in pancreatic cancer. Artificial intelligence and machine learning algorithms are increasingly being applied to large multi-omics datasets, enabling the identification of complex molecular patterns that may not be readily detectable using conventional analytic approaches [20]. By combining genomic sequencing, transcriptomic profiling, and advanced imaging data, AI-driven platforms have the potential to improve risk prediction, refine diagnostic accuracy, and guide personalized therapeutic decision-making [21]. These technologies may ultimately allow clinicians to transition from reactive treatment strategies toward proactive disease management based on predictive molecular modeling.
Within this evolving landscape, precision oncology is increasingly viewed as a dynamic process in which therapeutic strategies are continuously adapted according to the molecular characteristics of the tumor (Figure 1), the convergence of molecular biology, advanced diagnostics, and computational analysis is gradually transforming pancreatic cancer management from conventional multimodal therapy toward adaptive, precision-guided treatment strategies [22].
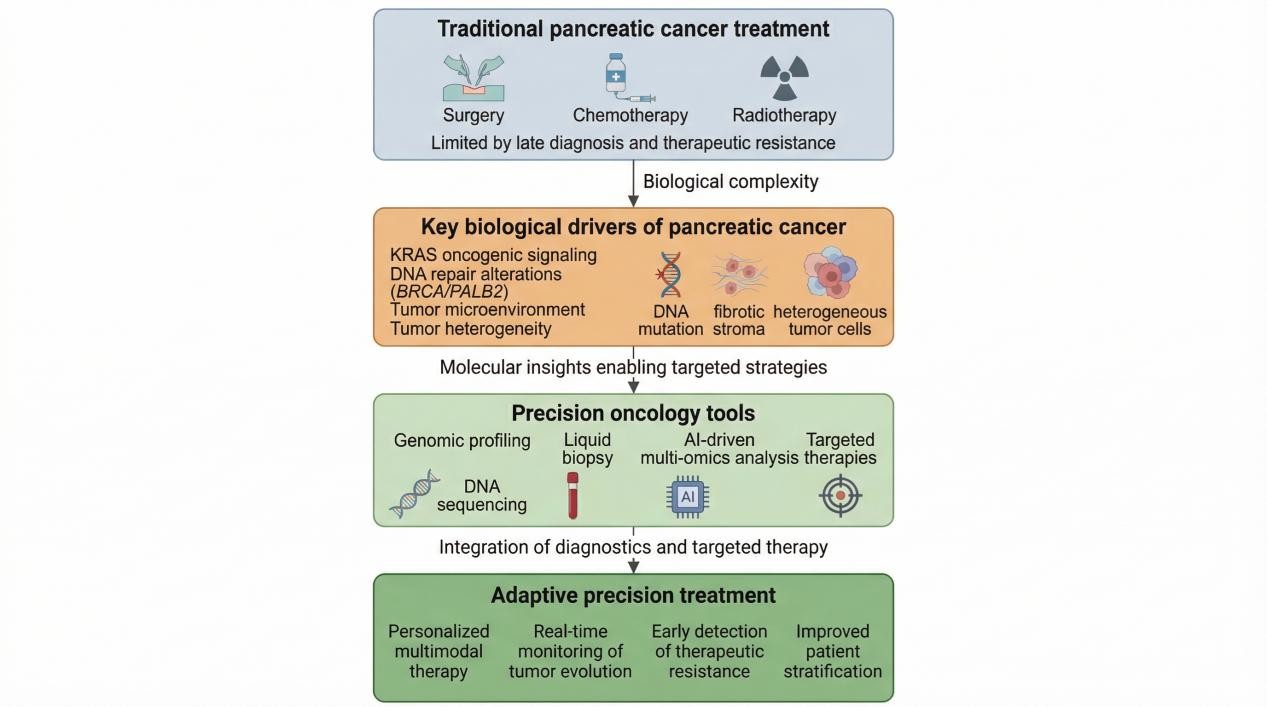
Figure 1. Conceptual framework illustrating the transition from conventional treatment strategies toward precision oncology in pancreatic cancer.
Traditional management approaches based primarily on surgery and cytotoxic chemotherapy are limited by late diagnosis, tumor heterogeneity, and therapeutic resistance. Advances in molecular profiling, liquid biopsy technologies, and computational analysis are enabling precision oncology approaches that integrate genomic insights with targeted therapeutics and real-time disease monitoring, ultimately supporting adaptive and personalized treatment strategies.
Adaptive Precision Oncology Paradigm
Future developments increasingly point toward a therapeutic paradigm in pancreatic cancer in which treatment strategies are guided by an integrated understanding of tumor genetics, microenvironmental biology, and dynamic disease monitoring. Rather than relying solely on conventional treatment algorithms based on anatomical staging, emerging approaches incorporate molecular profiling and biomarker-driven stratification to guide therapeutic decision-making. In this evolving framework, genomic alterations such as KRAS mutations and defects in DNA damage repair pathways provide critical entry points for targeted intervention, while advances in liquid biopsy technologies offer opportunities to monitor clonal evolution and therapeutic resistance throughout the course of treatment. At the same time, the growing recognition of the biological influence of the tumor microenvironment underscores the importance of combination strategies capable of overcoming stromal barriers and immune suppression that characterize pancreatic tumors [23].
Importantly, these innovations are unlikely to succeed in isolation. Instead, the future of pancreatic cancer therapy will likely depend on the integration of multiple complementary approaches that collectively address the complex biology of this disease. Targeted therapies directed against oncogenic drivers, molecular diagnostics capable of capturing tumor heterogeneity, and computational platforms designed to interpret large-scale multi-omics datasets may together enable the development of adaptive treatment strategies tailored to individual patients. Within such a precision oncology framework, therapeutic interventions can be continuously refined according to evolving molecular information, allowing clinicians to anticipate disease progression and adjust treatment strategies accordingly. This dynamic model of cancer care represents a fundamental shift from traditional static treatment paradigms and holds particular promise for malignancies such as pancreatic cancer, where rapid tumor evolution and therapeutic resistance have historically limited clinical progress [24].
Statement of Priorities for Future Research
Future research in pancreatic cancer should focus on advancing precision oncology through targeted and integrated approaches. Key priorities include expanding therapeutic strategies against common KRAS mutations and overcoming mechanisms of treatment resistance. There is also a need for prospective clinical trials to validate biomarker-driven therapies and the clinical utility of molecular profiling and liquid biopsy for patient stratification and disease monitoring (Figure 2). Improving early detection remains critical, with emphasis on developing and validating non-invasive biomarkers such as circulating tumor DNA and exosomal signatures. Additionally, further investigation of the tumor microenvironment is essential to identify effective combination therapies that can overcome stromal and immune barriers. Finally, integrating artificial intelligence with multi-omics data holds promise for enabling more accurate and adaptive personalized treatment strategies.
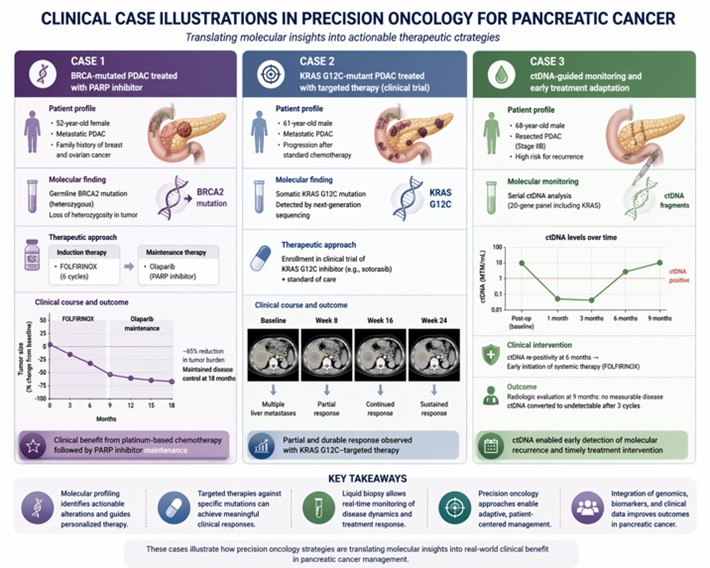
Figure 2. Clinical case illustrations demonstrating precision oncology approaches in pancreatic cancer, including biomarker-guided therapy selection, KRAS-targeted treatment strategies, and liquid biopsy–based real-time disease monitoring.
Limitations of the Manuscript
This manuscript has several limitations that should be acknowledged. First, as a narrative review, it is inherently subject to selection bias and does not follow a systematic methodology for literature inclusion, which may limit the comprehensiveness and reproducibility of the findings. Second, while the review highlights emerging precision oncology strategies, many of these approaches remain in early-phase clinical development, and robust evidence from large randomized controlled trials is still lacking. Third, the rapidly evolving nature of pancreatic cancer research means that newly published data, particularly in areas such as KRAS-targeted therapies and artificial intelligence applications, may not be fully captured. Fourth, the manuscript primarily focuses on molecular and technological advances and provides limited discussion on real-world implementation challenges, including cost, accessibility, and healthcare infrastructure limitations, which may affect the translation of precision oncology into routine clinical practice. Finally, heterogeneity in study designs, patient populations, and biomarker assessment methods across the cited literature may limit the generalizability of conclusions. Future work should incorporate systematic approaches and meta-analytic methods to provide more robust and quantitative assessments of emerging therapeutic and diagnostic strategies.
Clinical Case Illustrations in Precision Oncology
Emerging clinical evidence highlights the translational relevance of precision oncology approaches in pancreatic cancer. For instance, patients with germline BRCA1 or BRCA2 mutations have demonstrated meaningful clinical benefit from platinum-based chemotherapy followed by maintenance therapy with PARP inhibitors such as olaparib, reflecting the therapeutic vulnerability of DNA damage repair deficient tumors. Similarly, early-phase clinical trials investigating KRAS G12C inhibitors have reported objective responses in a subset of patients with advanced solid tumors, including pancreatic cancer, supporting the feasibility of directly targeting oncogenic drivers previously considered undruggable. In addition, liquid biopsy–guided monitoring using circulating tumor DNA has been shown to detect minimal residual disease and early recurrence earlier than conventional imaging, allowing timely modification of treatment strategies. Collectively, these clinical examples illustrate the potential of precision oncology to translate molecular insights into actionable therapeutic interventions in pancreatic cancer.
Conclusion
Although substantial progress has been achieved in understanding the molecular and biological complexity of pancreatic cancer, translating these insights into meaningful improvements in patient outcomes remains a major challenge. Continued advances in genomic profiling, liquid biopsy technologies, and computational medicine are progressively enabling the implementation of precision oncology strategies in clinical practice. The integration of these approaches with targeted therapeutics and multidisciplinary care may ultimately redefine the management of pancreatic cancer, transforming it from a uniformly lethal disease into one in which treatment is guided by the evolving molecular characteristics of each patient’s tumor. Achieving this goal will require sustained collaboration across clinical oncology, molecular biology, and data science, as well as prospective clinical trials designed to validate precision-guided treatment strategies and translate emerging molecular insights into meaningful improvements in patient outcomes.
Ethics Approval and Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Availability of Data and Materials
All data is available, and sharing is available as well as publication.
Authors' Contributions
Sakarie Mustafe Hidig: Writing the original draft, Validation, Project administration, Methodology, Investigation, Formal analysis, Data curation, Conceptualization.
Conflict of Interest
Authors declare no conflict of interest.
Funding
Authors declare no funding has been received in order to complete this study.
References
2. Cai J, Chen H, Lu M, Zhang Y, Lu B, You L, et al. Advances in the epidemiology of pancreatic cancer: Trends, risk factors, screening, and prognosis. Cancer Lett. 2021 Nov 1;520:1–11.
3. Springfeld C, Jäger D, Büchler MW, Strobel O, Hackert T, Palmer DH, Neoptolemos JP. Chemotherapy for pancreatic cancer. Presse Med. 2019 Mar;48(3 Pt 2):e159–74.
4. Conroy T, Desseigne F, Ychou M, Bouché O, Guimbaud R, Bécouarn Y, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med. 2011 May 12;364(19):1817–25.
5. Von Hoff DD, Ervin T, Arena FP, Chiorean EG, Infante J, Moore M, et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N Engl J Med. 2013 Oct 31;369(18):1691–703.
6. Wainberg ZA, Melisi D, Macarulla T, Pazo Cid R, Chandana SR, De La Fouchardière C, Dean A, Kiss I, Lee WJ, Goetze TO, Van Cutsem E, Paulson AS, Bekaii-Saab T, Pant S, Hubner RA, Xiao Z, Chen H, Benzaghou F, O'Reilly EM. NALIRIFOX versus nab-paclitaxel and gemcitabine in treatment-naive patients with metastatic pancreatic ductal adenocarcinoma (NAPOLI 3): a randomised, open-label, phase 3 trial. Lancet. 2023 Oct 7;402(10409):1272–81.
7. Hidig SM, Mujahid MUF, Kitaghenda FK, Hu Z. Advancing Therapeutic Strategies for Pancreatic Cancer: A Review of Surgical, Systemic and Diagnostic Innovations. Bratisl Med J. 2026;127:48–60.
8. Schneider M, Hackert T, Strobel O, Büchler MW. Technical advances in surgery for pancreatic cancer. Br J Surg. 2021 Jul 23;108(7):777–85.
9. Ghiglione N, Abbo D, Bushunova A, Costamagna A, Porporato PE, Martini M. Metabolic plasticity in pancreatic cancer: The mitochondrial connection. Mol Metab. 2025 Feb;92:102089.
10. Waddell N, Pajic M, Patch AM, Chang DK, Kassahn KS, Bailey P, et al. Whole genomes redefine the mutational landscape of pancreatic cancer. Nature. 2015 Feb 26;518(7540):495–501.
11. Hayashi A, Hong J, Iacobuzio-Donahue CA. The pancreatic cancer genome revisited. Nat Rev Gastroenterol Hepatol. 2021 Jul;18(7):469–81.
12. Collisson EA, Bailey P, Chang DK, Biankin AV. Molecular subtypes of pancreatic cancer. Nat Rev Gastroenterol Hepatol. 2019 Apr;16(4):207–20.
13. Ryan MB, Corcoran RB. Therapeutic strategies to target RAS-mutant cancers. Nat Rev Clin Oncol. 2018 Nov;15(11):709–20.
14. Canon J, Rex K, Saiki AY, Mohr C, Cooke K, Bagal D, et al. The clinical KRAS(G12C) inhibitor AMG 510 drives anti-tumour immunity. Nature. 2019 Nov;575(7781):217–23.
15. Hofmann MH, Gerlach D, Misale S, Petronczki M, Kraut N. Expanding the Reach of Precision Oncology by Drugging All KRAS Mutants. Cancer Discov. 2022 Apr 1;12(4):924–37.
16. Hidig SM, Kitaghenda FK. Next-generation Cancer Screening and Prevention: The Convergence of Liquid Biopsy Diagnostics. Artificial Intelligence and Precision Medicine. Compr Cancer Detect Prev. 2025;1(1):001-5.
17. Li X, Jiao Y, Liu YH. Precision medicine advances in pancreatic cancer driven by genomic and molecular alterations. World J Gastrointest Oncol. 2025 Nov 15;17(11):111264.
18. Cohen JD, Javed AA, Thoburn C, Wong F, Tie J, Gibbs P, et al. Combined circulating tumor DNA and protein biomarker-based liquid biopsy for the earlier detection of pancreatic cancers. Proc Natl Acad Sci U S A. 2017 Sep 19;114(38):10202–7.
19. Ma L, Guo H, Zhao Y, Liu Z, Wang C, Bu J, et al. Liquid biopsy in cancer current: status, challenges and future prospects. Signal Transduct Target Ther. 2024 Dec 2;9(1):336.
20. Yee NS, Zhang S, He HZ, Zheng SY. Extracellular Vesicles as Potential Biomarkers for Early Detection and Diagnosis of Pancreatic Cancer. Biomedicines. 2020 Dec 7;8(12):581.
21. Panda A, Falasca M, Ragunath K. Extracellular vesicles in pancreatic cancer: a new era in precision medicine. Transl Gastroenterol Hepatol. 2024 Apr 10;9:29.
22. Huang B, Huang H, Zhang S, Zhang D, Shi Q, Liu J, et al. Artificial intelligence in pancreatic cancer. Theranostics. 2022 Oct 3;12(16):6931–54.
23. Kung HC, Zheng KW, Zimmerman JW, Zheng L. The tumour microenvironment in pancreatic cancer - new clinical challenges, but more opportunities. Nat Rev Clin Oncol. 2025 Dec;22(12):969–95.
24. Kumari S, Peela S, Nagaraju GP, Srilatha M. Polysaccharides as therapeutic vehicles in pancreatic cancer. Drug Discov Today. 2025 Mar;30(3):104320.