Abstract
Objective: To successfully manage odontogenic maxillary sinusitis & subclinical oroantral communication post dental implant, using combined endoscopic & Caldwell Luc approach without removing dental implant.
Material and Methods: A 71-year-old lady with dental implants presented with odontogenic maxillary sinusitis + subclinical oroantral communication. Functional Endoscopic Sinus Surgery (FESS) was performed to clear the left-sided sinuses. The maxillary sinus was opened using Caldwell-Luc approach and a 0o endoscope introduced. Titanium screw of implant was thoroughly covered with bone wax. Diagnostic nasal endoscopy was done 3 weeks postoperatively wherein methylene blue dye was instilled into the opening of the maxillary sinus under endoscopic vision. Oral cavity was checked for dye leakage around the implant; there was no dye leakage suggesting the track around the screw had been obliterated successfully. This report was prepared according to CARE checklist.
Results: The patient is doing well 16 months postoperatively with no complaints of any foul-tasting discharge.
Conclusion: We conclude that FESS & Caldwell Luc approach is a successful combined approach to manage odontogenic maxillary sinusitis with oroantral communication and may allow salvage of dental implant, which would have to be removed otherwise.
Keywords
Odontogenic maxillary sinusitis, Caldwell-Luc procedure, Maxillary sinusitis, Odontogenic, Dental implants, Endoscope-assisted surgery, Case report
Background
Maxillary sinusitis is defined as an inflammation of the Schneiderian membrane (respiratory epithelium). It is acute if symptoms have been present for less than one month, subacute if lasting for 1–3 months and termed chronic if it is present for a period of more than three months [1].
Odontogenic maxillary sinusitis (OMS) is maxillary sinusitis caused by an underlying dental etiology such as tooth extraction, periapical/periodontal infections, or oroantral communication (OAC). Nowadays the incidence of odontogenic maxillary sinusitis (OMS) is found to be as high as 30% because of the increasing number of dental procedures, especially dental implants [2]. These procedures have resulted in increased number of complications such as formation of oroantral communication (OAC). Usually small OACs (3–5 mm diameter) close on their own, but larger ones as well as symptomatic smaller ones require surgical closure. Here we discuss a case of post dental implantation OMS, with symptomatic OAC managed successfully with combined approach Functional Endoscopic Sinus Surgery (FESS) + Caldwell Luc surgery.
Case Report
A 71 year-old lady reported to the ENT OPD with complaints of post nasal drip and foul-tasting discharge in her mouth around her left upper last teeth for the past one year. She had received dental implants (Titanium Alloy Grade 5 Endosteal implants) two years ago in her upper left jaw, last two teeth (molars). There was no history of pain, bleeding, swelling, any eye symptoms, loosening of implants or frank pus discharge from gums or nose. On examination there was no swelling in or around cheek or eye or gums; local examination revealed no obvious opening around the dental implant, but on blowing patient felt an air leak. Remaining ENT examination was within normal limits. A diagnostic nasal endoscopy revealed some degree of right-sided deviated nasal septum; rest examination was unremarkable. A contrast-enhanced CT scan of nose and paranasal sinuses revealed mucosal thickening in the left maxillary and anterior ethmoidal sinuses (Figure 1). We obtained CT as CBCT was not available in our institution. No obvious sinus track could be visualized. The right side sinuses were normal. There was no history of hypertension/diabetes mellitus/any other chronic illness or medications. Dental opinion was sought and local infection/periodontitis/implant infection were ruled out.
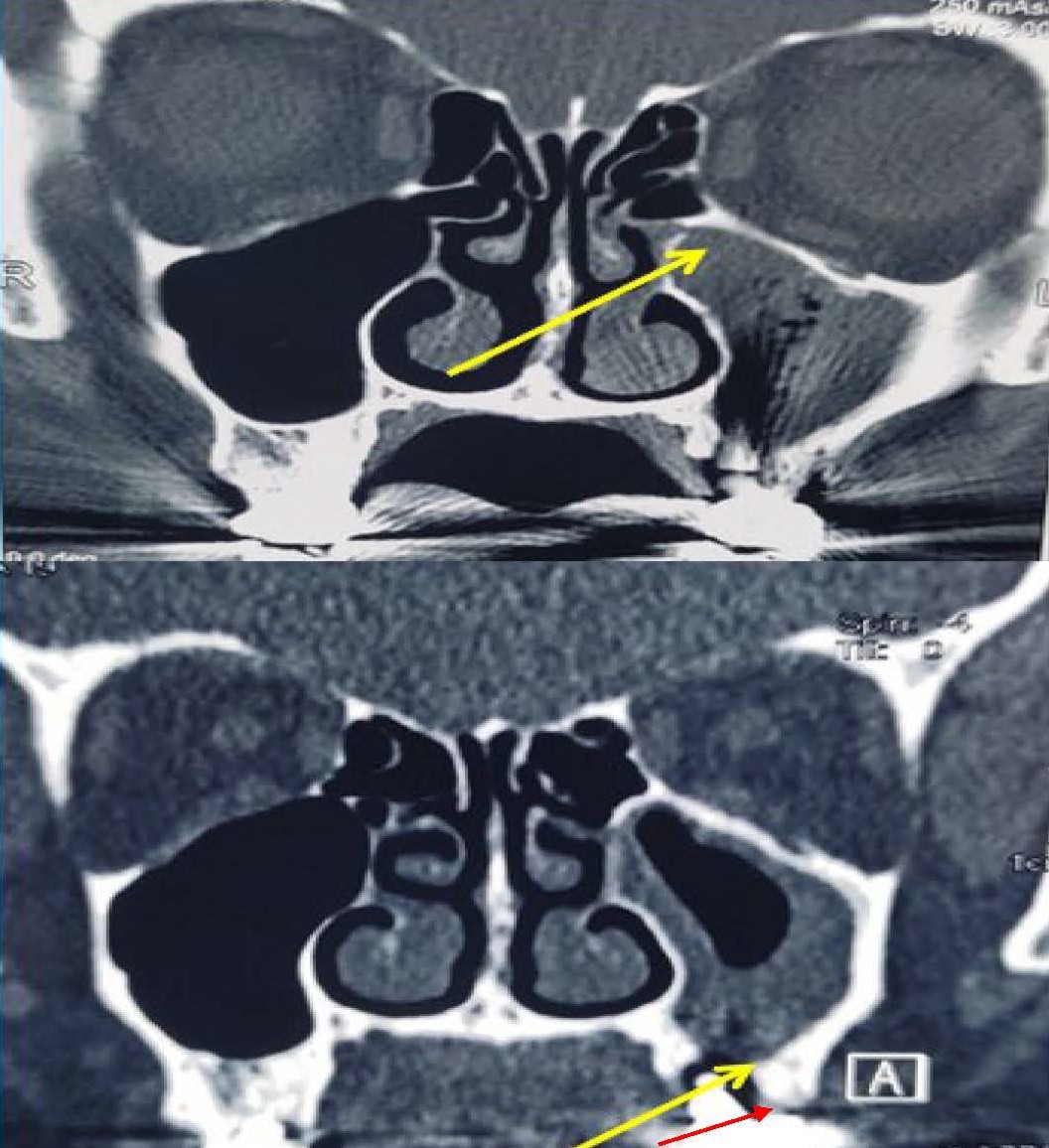
Figure 1. Upper panel showing CT image with arrow pointing to left maxillary sinus opacification, suggestive of odontogenic maxillary sinusitis. Lower panel: yellow arrow pointing to rarefaction. Red arrow pointing to presumptive area of breach i.e. possible site of oroantral fistula or leak.
Our goal was to address odontogenic maxillary sinusitis and oroantral communication together in one procedure. We carried out a functional endoscopic sinus surgery (FESS) to clear the left-sided sinuses and undertake left maxillary sinus exploration via Caldwell-Luc approach to identify and obliterate any sinus track if seen, simultaneously. Although Caldwell-Luc approach was done, FESS was also done in the same sitting because the ciliary movements of maxillary sinus cause mucus drainage of the sinus through the natural maxillary ostium only. Hence even if clearance of the sinus is done via Caldwell Luc, if the lateral nasal wall and hence maxillary ostium is not addressed and widened via FESS, normal pathways of mucus drainage are not addressed which may lead to recurrence of sinus infection and oroantral communication.
Ethical clearance was obtained from the hospital Ethics Committee and written informed consent from patient for performing the procedure under local anesthesia. Patient was given a choice of general anesthesia, but she preferred local anesthesia after being explained in detail about both local and general anesthesia, as she didn’t wish to undergo intubation and prolonged recovery. After performing FESS, the maxillary sinus was opened using Caldwell-Luc approach (Figure 2) and a 0o endoscope introduced into the maxillary sinus. Titanium screw of the dental implant could be seen arising from the floor of the sinus (Figure 3).
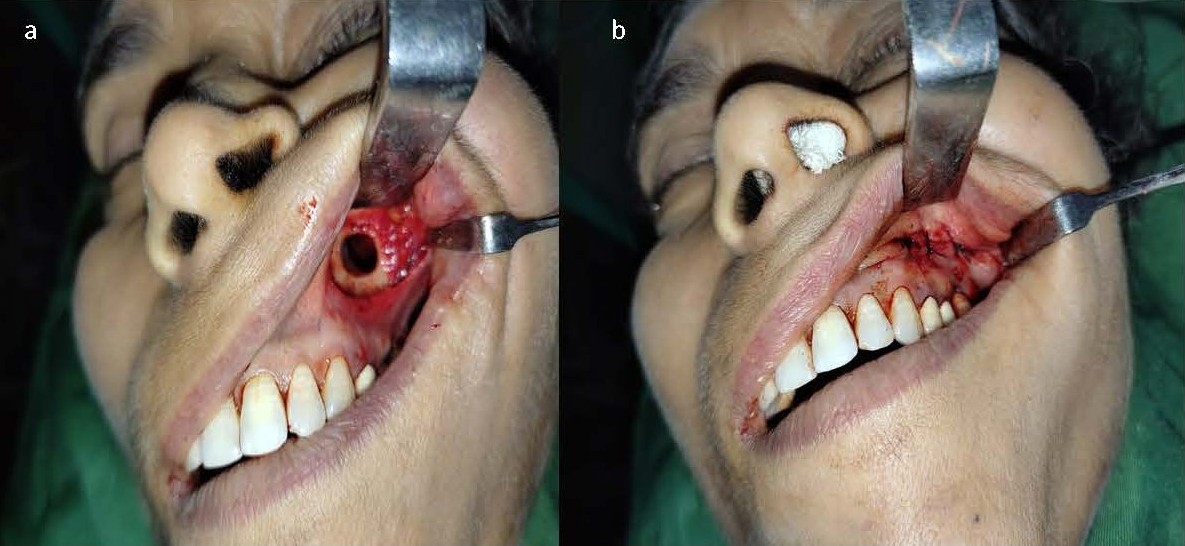
Figure 2. a) Caldwell Luc approach to left maxillary sinus. b) After closure.
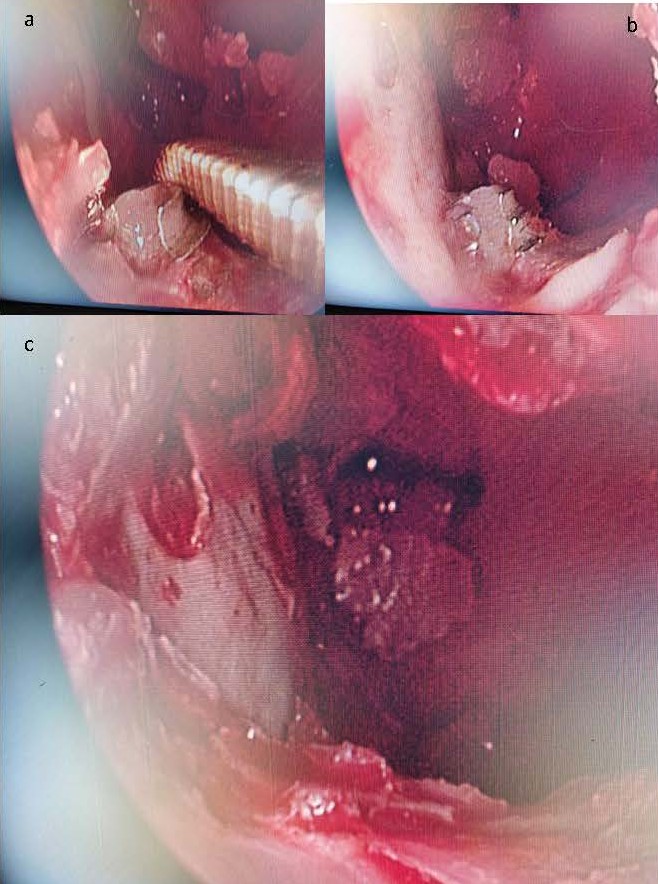
Figure 3. a) and b) 00 endoscopic view of the inside of the left maxillary sinus with instrument pointing to dental implant. c) View after covering implant thoroughly with bone wax.
Assessment of intraoperative leakage
Mucosa of the sinus was thoroughly debrided. Post-debridement, blood could be seen seeping around the dental implant in the oral cavity, suggestive of oroantral communication around the implant screw. The screw was thoroughly covered with bone wax (0.5–1 cubic centimetres approx.) all around its circumference and antibiotic-soaked gauze pack was placed in the sinus and left nasal cavity. Patient was given ice-packs to place on her cheek to prevent post-operative swelling. Packing was removed after 48 hours and patient was instructed to avoid brushing and chewing on that side for at least 3 weeks. The type of dental implant is shown in Figure 4.
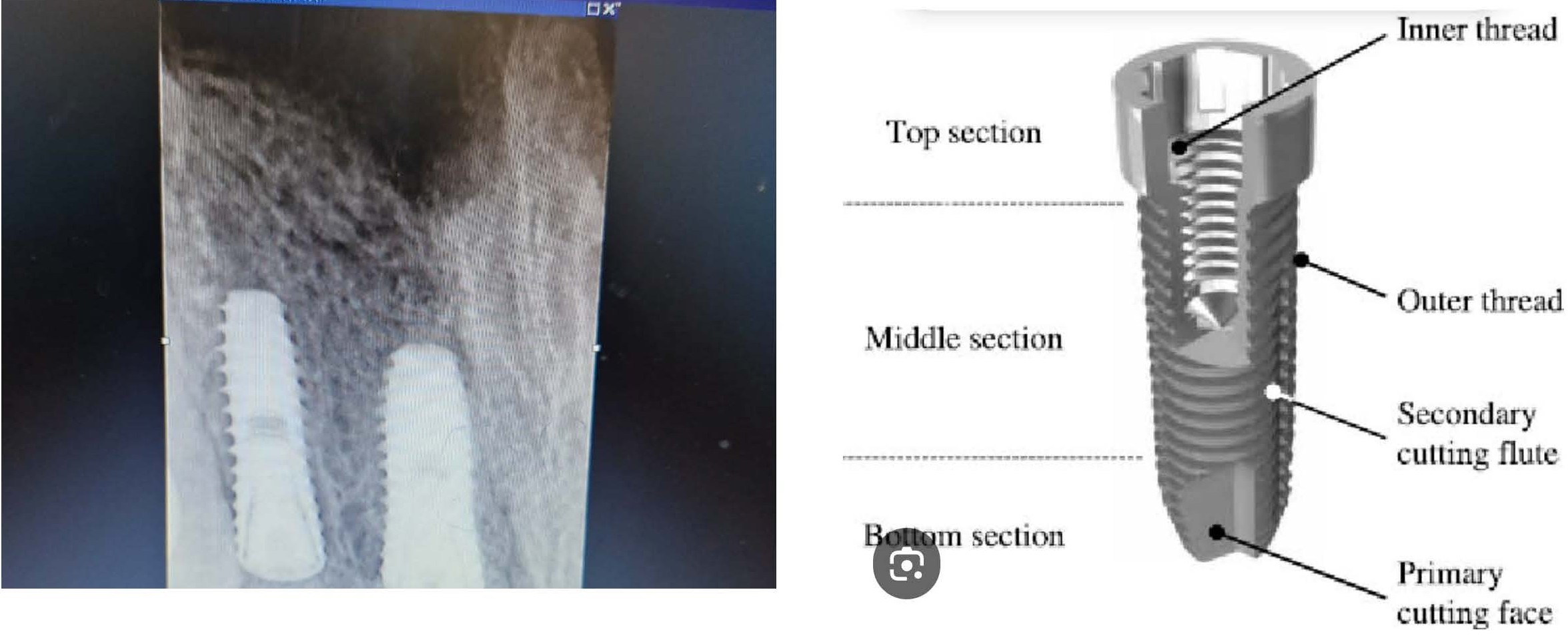
Figure 4. Left panel shows initial postoperative X-ray of patient. Right panel shows the type of titanium dental implant placed in the patient.
The patient tolerated the surgery well under local anesthesia. Vitals like blood pressure, oxygen saturation, and pulse rate were monitored throughout and were stable. Verbal feedback regarding pain and comfort was obtained constantly; there were no complaints of pain or discomfort. Antibiotics- co-amoxiclav 625 mg three times a day, metronidazole 400 mg three times a day-analgesics- diclofenac sodium and paracetamol combination three times a day, and pantoprazole 40 mg once a day were prescribed for 10 days postoperatively. Chlorhexidine mouthwash was advised after every meal.
A diagnostic nasal endoscopy was done 3 weeks postoperatively wherein methylene blue dye was instilled into the opening of the maxillary sinus under endoscopic vision. Oral cavity was checked for dye leakage around the implant; there was no dye leakage suggesting the track around the screw had been obliterated successfully. The patient is doing well sixteen months postoperatively with no complaints of any foul-tasting discharge.
Discussion
Odontogenic maxillary sinusitis (OMS) is sinus disease arising from dentoalveolar structures and causing damage to the maxillary sinus floor and epithelium. It is iatrogenic in about 66% cases, while other causes include apical and marginal periodontitis. It is an understudied form of sinusitis, the incidence of which is increasing nowadays because of the increase in the number of dental implant procedures [3].
Oroantral communication (OAC) is a pathological communication between the oral cavity and maxillary sinus which is iatrogenic most of the time. It may be acute (immediately following a dental intervention) or chronic (manifesting at a later time) [4]. Our patient had a chronic oroantral communication that manifested after one year of obtaining her dental implants. Although imaging did not show an obvious track, intraoperative blood staining around the implant during FESS + Caldwell Luc suggested to us a defect. Further 1-month, 3-month and 6-month postoperative nasal endoscopy done with methylene blue showed no leak. The patient reports resolution of her nasal and oral symptoms and is satisfied with the surgery. Her SNOT 22 score improved from 19 (preoperative) to 9 (postoperative).
FESS done in conjunction with OAC closure has advantage in restoring the normal physiology and aeration of the maxillary sinus, increasing chances of closure of the OAC [5]. Besides, it is a one-stage surgery resulting in better patient comfort. Despite this some authors still prefer doing 2-stage surgery [2]; FESS followed by delayed OAC closure. In our case we performed FESS first, widening the antrostomy, and then did a Caldwell Luc approach using the 00 endoscope to better visualize and manage the implant screw. We feel that performing definitive management of both pathologies in the same sitting would give better results. Our case is unique as we did not remove the implant but saved it; the absence of active infection made this novel approach feasible. There are reports in the literature regarding extrusion of bone wax post-surgery [6]. However, in our case no such sequelae were seen even after 16 months.
Management options
The standard management option would be to remove the dental implant, wait 6 to 8 weeks for spontaneous resolution of symptoms, and then perform a functional endoscopic sinus surgery and fistula closure if symptoms persisted. However, as our patient was insistent on saving her implant, we opted for this different and conservative approach.
Limitations of our study
There are some limitations of our report. The standard first line of management would be removal of the dental implant, as advised by the implantologist, but our patient was very unwilling for removal. Further discussion with the implantologist resulted in the decision to try for conservation of the implant if possible. They examined the implant and certified that there was no active infection.
Another limitation of our report is that it is a single report of one case. More cases are needed to ascertain outcomes. Our report can be the starting point for case series of such patients who are candidates for dental implant preservation.
Conclusion
The incidence of both OMS and OAC is increasing as a result of greater number of dental implants being done. OMS with OAC may be successfully managed with FESS and a modified Caldwell-Luc approach using the 00 endoscope, in selected patients. In absence of infection an attempt may be made to salvage a dental implant.
Patient Perspective (Obtained Verbally in the Local Language)
I used to have this foul-smelling discharge dripping into my throat, and foul taste around my dental implant for almost 1 year. My dentist suggested removal of the implant but I didn’t want to do it as I didn’t want to lose it and lose all the hard work that went into placing it. I sought ENT opinion and they suggested this novel approach to remove my symptoms and save the implant. I decided to go for it as it offered a chance to save my implant, which I was very keen on. The surgery was done in local anesthesia and I was comfortable during it except for initial pain during injection. Postoperatively I had to use ice-packs on my face to prevent swelling which was not very comfortable. I had a little bit of eye swelling which went off by next day, and no face swelling. The dentist cleared me for this surgery and allowed us to go ahead. Now 16 months down, I am satisfied with the surgery. There is no bad taste or smell, no unpleasant throat drip, and no feeling of air leak around my implant. I am on regular follow up.
Declarations
Ethics approval and consent to participate
Study ethically approved by Institutional Ethics Committee.
Written informed consent to participate obtained from patient.
Use of any animal or human data or tissue
Not applicable.
Written informed consent obtained from the patient for use of their data in the case presentation.
Consent for publication
Written informed consent obtained from patient.
Availability of data and material
Data available on request.
Competing interests
None.
Funding
None.
Authors' contributions
All authors contributed to this work in terms of procedure performed, follow up, research, drafting manuscript, editing and final approval.
JS, RA, and PS were involved in planning and carrying out the surgery and final approval of the manuscript.
RA, PS, and VR were responsible for research and drafting the manuscript, editing, and final approval of the manuscript.
Data availability statement
All data relevant to this clinical experience is available on request.
Acknowledgements
All Staff of Civil Hospital, Sector 6, Panchkula, Haryana 134109.
References
2. Psillas G, Papaioannou D, Petsali S, Dimas GG, Constantinidis J. Odontogenic maxillary sinusitis: A comprehensive Review. J Dent Sci. 2021 Jan;16(1):474–81.
3. Lechien JR, Filleul O, Costa de Araujo P, Hsieh JW, Chantrain G, Saussez S. Chronic maxillary rhinosinusitis of dental origin: a systematic review of 674 patient cases. Int J Otolaryngol. 2014;2014:465173.
4. Procacci P, Alfonsi F, Tonelli P, Selvaggi F, Menchini Fabris GB, Borgia V, et al. Surgical Treatment of Oroantral Communications. J Craniofac Surg. 2016 Jul;27(5):1190–6.
5. Andric M, Saranovic V, Drazic R, Brkovic B, Todorovic L. Functional endoscopic sinus surgery as an adjunctive treatment for closure of oroantral fistulae: a retrospective analysis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010 Apr;109(4):510–6.
6. Baird SM, Teh BM, Lim KKM, Campbell MC. Bone wax extrusion through postauricular wounds: A case series. Laryngoscope. 2018 Feb;128(2):369–72.