Abstract
Background and aims: Caudal epidural block is a commonly used technique for perineal surgeries in children. It is also used for chronic pain management in adults. Due to anatomical changes and variation, failure rate of caudal block in adults is very high with conventional landmark guided technique even in experienced hands. With the advent of ultrasonography, the success rate of caudal block has improved leading to resurgence of interest. This study aims to find effectiveness of USG guided caudal block for post-operative analgesia in adult perineal surgeries. It also compares Ropivacaine 20 ml of 0.25% versus Dexamethasone 8 mg added as an adjuvant to Ropivacaine in terms of the duration of post-operative analgesia, patient satisfaction and any side effects.
Methods: In a randomized and double blind study, 60 patients scheduled for Perineal surgery under spinal anesthesia were randomly divided into two equal groups, Group R (n=30) and Group D (n= 30). Out of 60 patients enrolled, two patients were excluded and 58 patients were analyzed. After surgery, ultra-sound guided caudal block with Ropivacaine 0.25% 20 ml was given in group R and Ropivacaine 0.25% 20 ml and 8 mg Dexamethasone was given in group D in each patient. The NRS at 4, 6, 8, 10,12,14,16,18, 20, 22, and 24 hours after the caudal block was noted. The primary objective was to find the duration of post-operative analgesia (first request to rescue analgesia) and compare the two groups. The secondary objectives were to compare total amount of tramadol consumption between the two groups in 24 hours, to compare the pain scores (NRS) and patient satisfaction.
Results: Duration of post-operative analgesia i.e. time to first analgesic request was 15.24 ± 4.57 h in Group R compared to 17.72 ± 4.71 h in Group D. This result was statistically significant (p=0.04). The total tramadol consumption over 24 hours was comparable in group R and group D (p = 0.08). Pain scores (NRS) were comparable in group R and group D at all-time points of 4h, 6h, 8h,10h,12h,14h, 16h,18h, 20h, 22h, and 24h (p>0.05). Patient satisfaction in both groups was comparable (p=0.41). No patient had any block related complication.
Conclusion: The study concludes that USG guided caudal block is an effective mode of post-operative analgesia in adult perineal surgeries. Adding Dexamethasone to Ropivacaine increases the duration of post-operative analgesia compared to Ropivacaine. The total amount of tramadol consumption, pain scores and patient satisfaction were comparable between the two groups. Hence USG guided caudal block can be incorporated in multimodal analgesia for adult perineal surgeries.
Keywords
Adult Caudal block, Post-operative analgesia, Perineal surgeries
Introduction
Perineal surgeries, encompassing genitourinary, colorectal, and obstetric procedures, constitute a diverse array of interventions that often entail significant postoperative pain. Effective management of postoperative pain is essential not only for patient comfort but also for facilitating early mobilization, reducing complications, and enhancing overall recovery outcomes [1].
Caudal block using local anesthetics with adjuvants is one of the most established regional analgesic techniques to provide intra and post-operative analgesia in pediatric perineal surgeries. But very few literature is available on USG guided caudal block in adults for post-operative analgesia.
Caudal block in adults and elderly is technically challenging as with growth locating sacral hiatus is difficult using conventional landmark guided technique. Failure rate of caudal epidural block in adults is high even in experienced hands. With the advent of ultrasonography, it has been demonstrated to be highly effective in accurately guiding the needle entering the caudal epidural space with resurgence of interest in caudal block in adult for chronic pain relief and postoperative analgesia [3]. Caudal block has various advantages in anorectal surgery. First, it is technically a simple, single shot technique. Secondly, it can be used as a sole anesthesia technique, avoiding complications related to general anesthesia. Third, it improves postoperative pain relief, shortens the time in the recovery room, and enables early mobilization [5]. Also, it has lesser degree of hemodynamic instability, and minimal motor blockade compared to conventional epidural. Complications such as post dural puncture headache are also rarely encountered [6]. This study aims to throw more light on caudal block in adults for post-operative analgesia in perineal surgeries. It aims to compare 20 ml 0.25% Ropivacaine versus 20 ml 0.25% Ropivacaine with Dexamethasone 8 mg as an adjuvant in terms of the duration of post-operative analgesia, patients’ satisfaction, and any side effects.
Methods
After ethical clearance from our hospital and registration with the Clinical Trial Registry of India (CTRI/2023/01/048883), this prospective double blinded randomized trial was done at teaching industrial hospital from July 2022 to January 2024. After taking informed written consent, a total of 60 patients aged between 18–70 years scheduled for perineal surgery under subarachnoid block and belonging to American Society of Anesthesiologists (ASA) grade I to III were enrolled for this study. Refusal to participate, contraindications to regional anesthesia (allergy, bleeding diathesis, infection at the site of block), uncontrolled diabetes mellitus, anatomical abnormality, subarachnoid block failure were exclusion criteria (Figure 1).
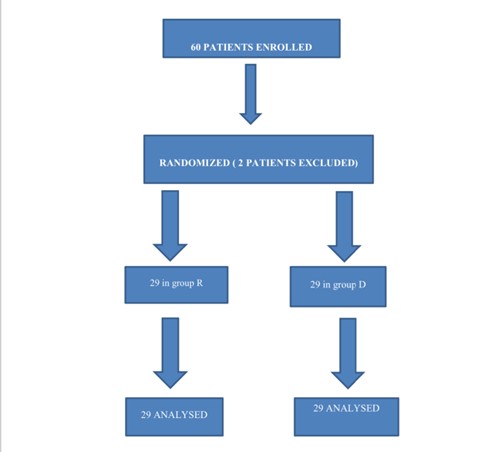
Figure 1. Consort flow diagram for enrollment, group allocation, follow-up and analysis. Group-R (0.25% Ropivacaine), Group-D (0.25% Ropivacaine with Dexamethasone 8 mg).
This study aims to compare the analgesic efficacy 20 ml of 0.25% Ropivacaine versus Dexamethasone 8 mg added as an adjuvant to Ropivacaine for caudal block in adult perineal surgery as postoperative analgesia.
The primary objective was to compare the duration of post-operative analgesia (first request to rescue analgesia). The secondary objectives were to compare total amount of tramadol consumption between the two groups in 24 hours, to compare the pain scores, Numeric Rating Scale (NRS) and patient satisfaction in 24 hours postoperatively.
Each patient was enrolled in the study after obtaining a detailed history and conducting a clinical examination during the pre-anesthetic check-up. All 60 eligible patients were randomly allocated to either: group R or group D (n=30 in each group) by using random envelopes. Patients were given antibiotic prophylaxis after securing an 18–20-gauge intravenous cannula and taken to the operating room, here intravenous fluid was started, and standard non-invasive monitors (ECG, NIBP, pulse oximetry) were attached. Then the patients were made to sit for CNB. All the patients were given sub arachnoid block under full aseptic conditions with 2.4 ml 0.5% Bupivacaine (Heavy) using a 26-gauge Quinke’s needle. Caudal block was performed post-operatively within 30 minutes after the perineal surgery. Patients were placed in left lateral position with hips and knees flexed. Under strict aseptic precautions, Caudal block was performed as per standard technique as follows: With the patient in the lateral decubitus position with hips and knee flexed, a linear high-frequency transducer was placed transversely in the midline to obtain a transverse view of the sacral hiatus. The bony prominences of the two sacral cornua appear as two hyperechoic reversed U-shaped structures. Between the two cornua, two hyperechoic band-like structures the sacrococcygeal ligament superiorly and the dorsal bony surface of the sacrum inferiorly was identified. A 21-gauge needle was inserted between the two cornua into the sacral hiatus and the sacrococcygeal ligament was penetrated. The transducer was then rotated 90 degrees to obtain a longitudinal view of the sacrum and sacral hiatus, and the needle was advanced into the sacral canal. The injection was given after negative aspiration for blood or cerebrospinal fluid. The drug was given in the caudal space according to the group assigned.
After the block the observer was called to note the time of block. The time of completion of block was taken as 0-point time reference, and all the subsequent observation was done within this reference ?0. The patients were shifted to post anesthesia care unit (PACU). The vitals were recorded and documented intraoperatively.
Postoperatively injection paracetamol 1 gm 8 hourly continued as a part of the multimodal analgesia. Injection tramadol 50 mg intravenously was given as rescue analgesia when NRS was > 4 up to a maximum dose of 200 mg in 24 hours and the time was recorded. If pain was not controlled with maximum dose of tramadol, those patients were given alternate analgesic and these patients were excluded. Numerical Rating Scale for post–operative pain was recorded at 4, 6, 8, 10, 12, 14, 16, 18, 20, 22, and 24 hours. Time of first rescue analgesia and total requirement of tramadol in 24 hours was noted. Patient’s satisfaction score was also noted using rating score (1 - disatisfied, 2-satisfied, 3- highly satisfied) assessed 24 hours after the surgery.
Sample size was calculated using the following formula
N = 2σ (zcrit + zpwr)2 / D2
Where
N = sample size per group
σ = standard deviation
z crit = standard normal deviate for 0.05 significance = 1.96
z pwr = standard normal deviate for 80% power = 0.842
D = difference of means
The values were obtained using data from the previous study by Prasad, et al [5].
We took mean duration of analgesia of 478.04 ± 61.22 min of the Dexamethasone group from the previous study, and postulate it to be 10% longer than Ropivacaine only group. Taking the confidence level = 95% and desired power of study as 80%.
Each group required 26 patients, and considering 10% attrition and rounding of the figure total 60 patients were taken up. The results were analyzed using statistical software (MedCalc version 20.0). Continuous data was assessed for normality using the Kolmogorov-Smirnov test of normality. Normally distributed data (represented as Mean ± SD) was assessed using the student’s t-test (two tailed, equal variances) and non-normally distributed data [represented as median (range)] were assessed using the Mann-Whitney U-test. Ordinal data were represented as median & interquartile range (IQR) and assessed using the Mann-Whitney U-test. A p-value <0.05 was considered significant.
Results
A total of 60 patients were enrolled, two patients were excluded and 58 patients were analyzed. Demographic variables, duration of surgery in group R and group D were comparable (p>0.05) (Table 1).
|
Variables |
Group R |
Group D |
p - value |
|
Age (years), Mean (SD) |
44.24 ± |
47.20 ± 15.89 |
0.43 |
|
Male/Female |
22/7 |
17/12 |
0.16 |
|
ASA class I/II/III |
8/16/5 |
5/16/8 |
0.50 |
|
Weight (kg), Mean (SD) |
68.03 ± |
67.27 ± 13.10 |
0.81 |
|
Height (cm), Mean (SD) |
163.37 ± |
162.55 ± 8.60 |
0.71 |
|
Duration of surgery (hr), Mean (SD) |
0.76 ± 0.39 |
0.92 ± 0.40 |
0.13 |
|
Tramadol used (mg), Median [IQR (75-25)] |
50[50(100-50)] |
50[25(50-25)] |
0.08 |
 12.89
12.89
The time to first analgesic request was (mean ± SD) 15.24 ± 4.57 h in Group R compared to (mean ± SD) 17.72 ± 4.71h in Group D. This result was statistically significant (p=0.04) (Figure 2). Post block Numeric rating score (NRS) was comparable in group R and group D at all-time points of 4h, 6h, 8h, 10h, 12h, 14h, 16h, 18h, 20h, 22h, and 24h (p>0.05) (Table 2). Numeric rating score (NRS) at 24 h in group R was (mean ± SD) 3.06 ± 0.79 and in group D was (mean ± SD) 2.89 ± 1.01 p=0.47 (comparable).The total tramadol consumption over 24 hours in both the groups were calculated using Mann Whitney U and in group R was Median [IQR] = 50[50(100-50)], while in group D was Median [IQR] = 50[25(50–25)] p-value = 0.08 were comparable. Patient’s satisfaction in both groups was comparable (p=0.41) (Table 3). No patient had any block related complication.
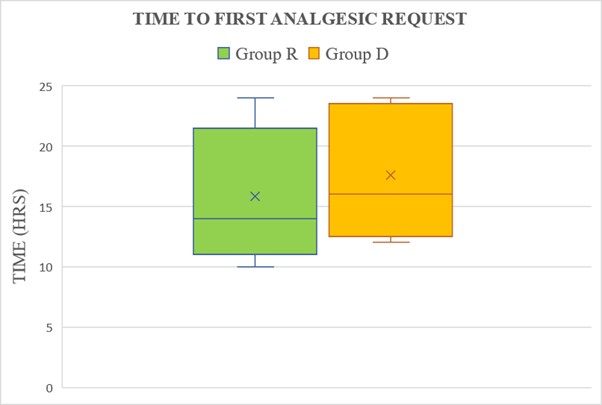
Figure 2. Box and plot graph showing time to first analgesic request. The × and middle line in each box represent the mean and median value respectively, the outer margins of the box represent the interquartile range and the whiskers represent the 10th and 90thpercentile at each point. [p-value=0.04, significant, Student T test (Unpaired)].
|
Time |
Group R |
Group D |
p- value |
|
4 hr |
1.20 ± 1.08 |
0.93 ± 0.92 |
0.30 |
|
6 hr |
1.55 ± 0.98 |
1.58 ± 1.01 |
0.89 |
|
8hr |
2.13 ± 0.95 |
1.96 ± 0.98 |
0.50 |
|
10 hr |
3.13 ± 1.48 |
2.79 ± 0.81 |
0.27 |
|
12 hr |
4 ± 1.71 |
3.44 ± 1.57 |
0.20 |
|
14 hr |
4.24 ± 1.70 |
3.48 ± 1.32 |
0.06 |
|
16 hr |
4.17 ± 1.10 |
3.75 ± 1.32 |
0.02 |
|
18 hr |
4.06 ± 1.09 |
3.55 ± 1.12 |
0.08 |
|
20 hr |
4.13 ± 1.18 |
3.72 ± 1.36 |
0.22 |
|
22 hr |
3.55 ± 1.15 |
3.37 ± 1.01 |
0.54 |
|
24 hr |
3.06 ± 0.79 |
2.89 ± 1.01 |
0.47 |









|
No. of subjects |
Group R |
Group D |
p-value |
|
Dissatisfied |
5 |
5 |
0.41 |
|
Satisfied |
20 |
16 |
|
|
Highly Satisfied |
4 |
8 |
|
Discussion
Several studies have shown good results with caudal block for post-operative analgesia in pediatric perineal surgeries. We hypothesized that USG guided caudal block in adulthood could be a good analgesic technique for post-operative analgesia in perineal surgeries. We aimed at comparing duration of analgesia with Ropivacaine and Ropivacaine with Dexamethasone as adjuvant. This prospective randomized trial was conducted to determine the benefit of adding Dexamethasone to Ropivacaine as an adjuvant in caudal block in terms of pain scores and duration of analgesia.
Conclusion
Therefore, we concluded that adding dexamethasone to Ropivacaine in caudal block increases the duration of post-operative analgesia (Time to first analgesic request) compared to Ropivacaine alone in adult perineal surgery. The total amount of tramadol consumption, pain scores and patient satisfaction were comparable between the two groups.
Declaration of Patient Consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial Support and Sponsorship
Nil.
Conflicts of Interest
There are no conflicts of interest.
References
2. Kao SC, Lin CS. Caudal Epidural Block: An Updated Review of Anatomy and Techniques. Biomed Res Int. 2017;2017:9217145.
3. Xie L, Tao H, Bao F, Zhu Y, Fang F, Bao X, et al. Major complications of caudal block: A prospective survey of 973 cases in adult anorectal surgery. Heliyon. 2023 Oct 6;9(10):e20759.
4. Vadhanan P, Rajendran I, Rajasekar P. Ultrasound-Guided Caudal Epidural Anesthesia in Adults for Anorectal Procedures. Anesth Essays Res. 2020 Apr-Jun;14(2):239–42.
5. Krishna Prasad GV, Khanna S, Jaishree SV. Review of adjuvants to local anesthetics in peripheral nerve blocks: Current and future trends. Saudi J Anaesth. 2020 Jan-Mar;14(1):77–84.
6. Kim EM, Lee JR, Koo BN, Im YJ, Oh HJ, Lee JH. Analgesic efficacy of caudal dexamethasone combined with ropivacaine in children undergoing orchiopexy. Br J Anaesth. 2014 May;112(5):885–91.