Abstract
Background: Diastasis recti is defined as an interrecti distance (IRD) over 23 mm in Beninese postpartum women. Its prevalence is 46%. The Curl-up acutely reduces the IRD but it increases the linea alba distortion
and it is considered to be hyperpressive. When Curl-up is combined with Diaphragmatic aspiration (DA) the intra-abdominal pressure is lower. Moreover, combining Curl-up with transversus abdominis activation
is recommended to decrease the linea alba distortion. However, the effect of this DA combined with Curlup on the IRD is not known in postpartum women.
Objectives: To study the acute effect of the DA combined with Curl-up, and of other abdominal exercises on IRD.
Methods: Beninese postpartum women diagnosed with diastasis recti participated in this cross-sectional study. IRD was measured at 5 cm above umbilicus with an ultrasound in 6 conditions performed in random order: rest, DA, Curl-up, Drawing-in, DA+Curl-up, Drawing-in+Curl-up. Values were expressed as median ± IQR and IRD was compared across these conditions using Friedman test and Wilcoxon test for post-hoc pairwise comparisons.
Results: Forty-nine women aged between 22 and 39 participated in this study. Compared to rest (26.7 ± 9.5 mm), no significant IRD difference was observed during either DA (26.0 ± 8.5 mm) or Drawing-in (29.0
± 10.0 mm), but IRD during Drawing-in was significantly larger than that during DA. Curl-up (18.7 ± 8.9 mm), Drawing-in+Curl-up (22.9 ± 9.7 mm) and DA+Curl-up (21.8 ± 9.3 mm) decreased the IRD (p<0.001). This decrease was the largest during Curl-up (p<0.001).
Conclusion: Compared to rest, DA and Drawing-in did not decrease IRD but their combination with Curlup slightly decreased IRD. Future studies are needed to investigate the acute effect of the combination of DA with Curl-up on the linea alba distortion.
Clinical Implication: Physiotherapists are regularly confronted with the management of the diastasis recti in postpartum women. DA combined with Curl-up can be used for management of diastasis recti in postpartum.
Keywords
Interrecti distance, Diaphragmatic aspiration, Hypopressive exercise, Curl-up, Ultrasound, Postpartum women, Benin
Introduction
During pregnancy, abdominal muscles changes are observed, especially the rectus abdominis muscles which stretch and move apart from each other to make room for the developing baby [1]. This spacing is called the interrecti distance (IRD). It occurs at the linea alba whose width is greatly increased in late pregnancy and even several months after delivery despite the physiological recovery observed during the first postpartum weeks [2-4]. Beyond a certain threshold which varies according to the studies, this large IRD becomes pathological and is diagnosed as diastasis recti. In a recent study of Beninese postpartum women who gave birth 6 weeks to 6 months earlier, the defined threshold was 23 mm at 5 cm above the umbilicus, with a diastasis recti prevalence of 46% [5]. A key objective of postpartum rehabilitation is to reduce the IRD below the threshold of diastasis recti. No evidence-based guidelines have been formulated so far [6-8].
In the last few years, many studies have focused on the IRD reduction after a training program in postpartum women [9-17]. Various exercises have been proposed in the different protocols used. All protocols showed positive results in reducing the IRD. However, only one protocol compared two groups performing different programs and none of these studies proposed a control group. In addition, these protocols combined several exercises and the specific effect of each exercise is not known. Recently, three studies have showed a significant IRD decrease as a result of a training protocol focused on one exercise, specifically hypopressive exercise, Curl-up and Drawing-in [18-20]. The lack of a control group in Ramirez-Jiménez et al. [20] study (hypopressive exercise), the small number of participants in Igwe, Okoye [18] study (Curl-up) and the fact that the participants in Tuttle et al. [19] study (Drawing-in) performed other activities (dance, walking, running) are limitations to these studies. In addition, these results have not yet been confirmed by other similar studies.
The acute effect of abdominal exercises has also been investigated with very different results depending on the exercise. The Curl-up was repeatedly showed to significantly reduce the IRD whether in nulliparous, postpartum or parous women [21-27]. During Drawing-in, an IRD increase was observed in postpartum and parous women, the increase being sometimes statistically significant and sometimes not [21,24]. Two studies that examined hypopressive exercises reported no IRD change in men, nulliparous and postpartum women during these exercises [22,28].
According to these results, the Curl-up is the most studied exercise and has shown a systematic IRD reduction both acutely and during training. However, its practice in postpartum women raises reservations due to its suspected hyperpressive effect and to the observed increase in linea alba distortion [27]. A combination of Curl-up with the belly drawing-in showed a smaller linea alba distortion, but IRD reduction was also smaller or non-significant depending on the level of measurement [27]. Lee and Hodges [27] explained the smaller linea alba distortion by the transversus abdominis activation. Two recent studies showed that, during the hypopressive exercises prone by Caufriez [29], the transversus abdominis muscle was activated [30] and no linea alba distortion was observed [28]. We wondered whether an hypopressive exercise combined with Curl-up could also acutely reduce the IRD. A low intra-abdominal pressure and a moderate pelvic floor activation have recently been observed during the combination of Curl-up with a specific hypopressive exercise i.e., Diaphragmatic aspiration (DA) [31]. This DA+Curl-up combination appeared therefore to be a safe exercise for the pelvic floor but its acute effect on IRD is not known.
The aim of this study was to investigate the acute effect of DA+Curl-up and other abdominal exercises (Curl-up, DA, Drawing-in, Drawing-in+Curl-up) on the IRD in Beninese postpartum women diagnosed with diastasis recti.
Materials and Method
Study design
This cross-sectional study investigated the acute effect of DA+Curl-up and other abdominal exercises on the IRD in Beninese postpartum women and was conducted at the Clinique Universitaire de Médecine Physique et Réadaptation (CUMPR), in the Centre National Hospitalier Universitaire Hubert Koutoukou Maga (CNHU-HKM) in Cotonou (Benin). All participants received an explanation of the objectives and requirements for participation in the study and then completed a consent form. Experimental procedures were performed in accordance with the Declaration of Helsinki and were approved by the Ethics Committee of CUMPR (N°01-2020/MS/CNHU-HKM/CER/CUMPR).
Participants
The participants were postpartum women recruited from the patients attending the CUMPR from June 2020 to August 2021. To be included participants had to be aged between 18 and 40, have given birth more than 6 weeks and less than 6 months earlier, have an IRD of at least 23 mm measured at 5 cm above the umbilicus [5]. Women being pregnant, having given birth within the previous 6 weeks or more than 6 months earlier, having undergone abdominal surgery within the previous 6 months excepted caesarean, and women who were unable to perform all the exercises correctly were excluded from the study.
Protocol
At the first appointment, information regarding age, parity, time elapsed since the last childbirth were collected, biometric data (height and weight), abdominal strength, abdominal endurance and IRD were measured. Participants who met the inclusion criteria were taught the different experimental conditions. If their ability to perform the conditions was insufficient, another appointment was scheduled to improve it. If it was satisfactory, an appointment was scheduled to collect data. At this data collection session, IRD was measured at 5 cm above the umbilicus during 6 conditions (Figure 1): Rest (in supine position with arms alongside the body and knees bent); Curl-up (with hands towards the knees bent, lift the head and the trunk slowly to the tip of the scapula); Drawing-in (with arms alongside the body and knees bent, draw the belly in to bring the umbilicus closer to the spine); Diaphragmatic aspiration (DA) (with arms alongside the body and knees bent, exhale gradually through the mouth by draw-in the belly, then hold the breath and pull the abdomen upwards); Drawing-in+Curl-up (do Drawing-in and add Curl-up); DA+Curl-up (do DA and add Curl-up). Exercises were performed in a random order defined by the participant who selected a number between 1 and 9. Each number corresponded to a predefined order. The IRD was measured while the subjects maintained the final position at the end of each condition. Each exercise was performed twice.
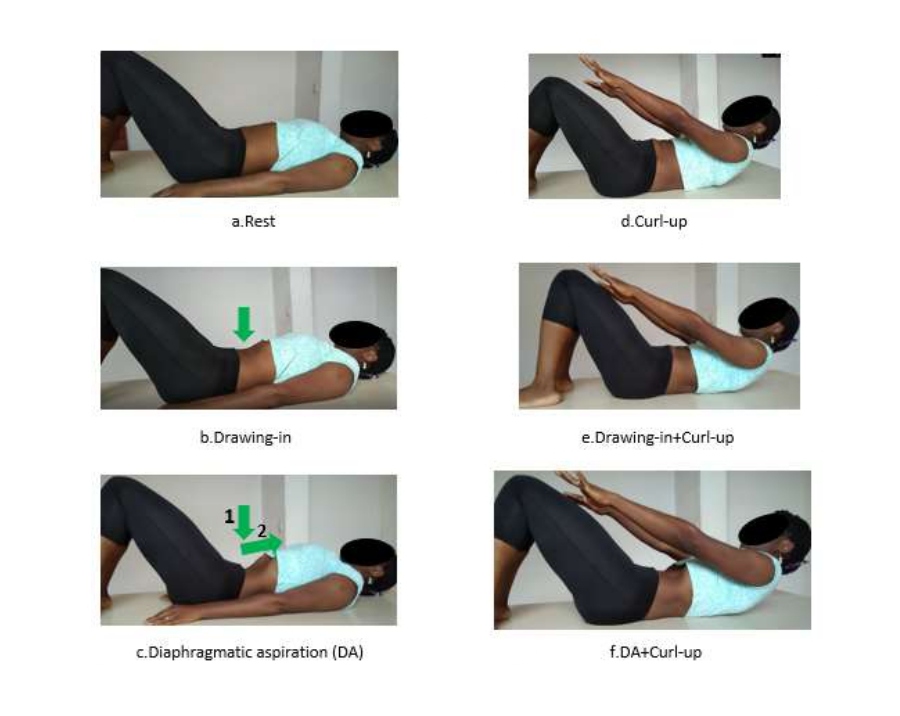
Figure 1. Illustration of the different abdominal exercises performed.
Data collection
IRD measurement was performed by a physiotherapist who had 15 years of experience and trained in ultrasound measurement with one year of experience in the use of this tool. Ultrasound is a valid and reliable tool to measure the IRD [32-37]. The Intra-Class Correlation Coefficient [95% confidence interval] for the IRD measurement above the umbilicus was 0.98 [0.92-0.99] in Chiarello, McAuley [32]. For this study, we used an ultrasound device Chison Eco, 5-11 MHz wideband Linear Probe. The participant was positioned supine, with bent knees. A mark was made at 5 cm above the upper edge of the umbilicus and measurements were made at this level. The examiner applied gel to the abdomen and placed the probe transversely over the skin mark without any pressure [32,33]. The image was then captured and the IRD measured, on the screen with the ultrasound calipers, as the space between the two sheaths of the rectus abdominis muscle as described by Djivoh et al. [5].
Abdominal muscle strength was measured using manual muscle testing according to Hislop et al. [38]. The participant was lying on the back with the knees bent and tried to lift the head and shoulders without moving the pelvis and the feet. The testing was rated from 0 to 5 depending on the final position.
0: does not lift anything;
1: only lifts the head;
2: lifts the head and the upper part of the shoulders with the arms extended towards the knees;
3: lifts the head and shoulders up to the point of the scapula with the arms extended towards the knees;
4: lifts the head and shoulders to the point of the scapula with the arms crossed on the chest;
5: lifts the head and shoulders to the point of the scapula with the hands at the back of the neck.
Abdominal muscle endurance was evaluated using position 2 of the manual testing described above. The participant maintained the position as long as possible. The measurement was expressed in seconds [39,40].
The abdominal skinfold was measured at 2 cm at the right of the umbilicus [41]. The measure was taken with ultrasound as the distance between the superficial part of the skin and the rectus abdominis muscle as described in previous study [5]. Biometric data (weight and height) were measured using a telescopic height scale (Seca 220).
Statistical analysis
For each condition, the average IRD value measured during two repetitions was used for statistical analysis using SPSS 27 software. Normality of distribution was assessed using Kolmogorov-Smirnov test. Due to non-normal distribution, non-parametric tests were used and the results were presented as median with interquartile range (IQR). The Friedman test was used to compare IRD across the 6 conditions and the post hoc Wilcoxon test for related samples to identify specific differences. The level of significance was set at 5%. It was adjusted for post hoc test by dividing 0.05 by the number of pairwise comparisons. The effect size (r) was calculated by dividing the z statistic by the square root of the number of cases (n) [42].
Results
One hundred and twenty-one postpartum women responded to our request. Sixty-two women were excluded because of having an IRD of less than 23 mm and ten were excluded because they were unable to correctly perform the exercises after two appointments. Figure 2 shows the flowchart for the recruitment of participants. The characteristics of the forty-nine women who were enrolled in this study are summarized in Table 1. They were aged (median ± IQR) 30.9 ± 7.0 years old with BMI average 23.1 ± 6.1 kg/m2. Table 2 presented the IRD for each condition. The IRD differed significantly among the 6 conditions: X2 = 208.9, ddl = 5, p<0.001. Compared to rest, no significant IRD change was observed during DA (p=0.1) and Drawing-in (p=0.08), but IRD was significantly larger during Drawing-in compared to DA (p=0.001). The IRD decreased significantly when Curl-up, Drawing-in+Curl-up and DA+Curl-up were performed (p<0.001). This decrease was larger during Curl-up than during the combined exercises (p<0.001).
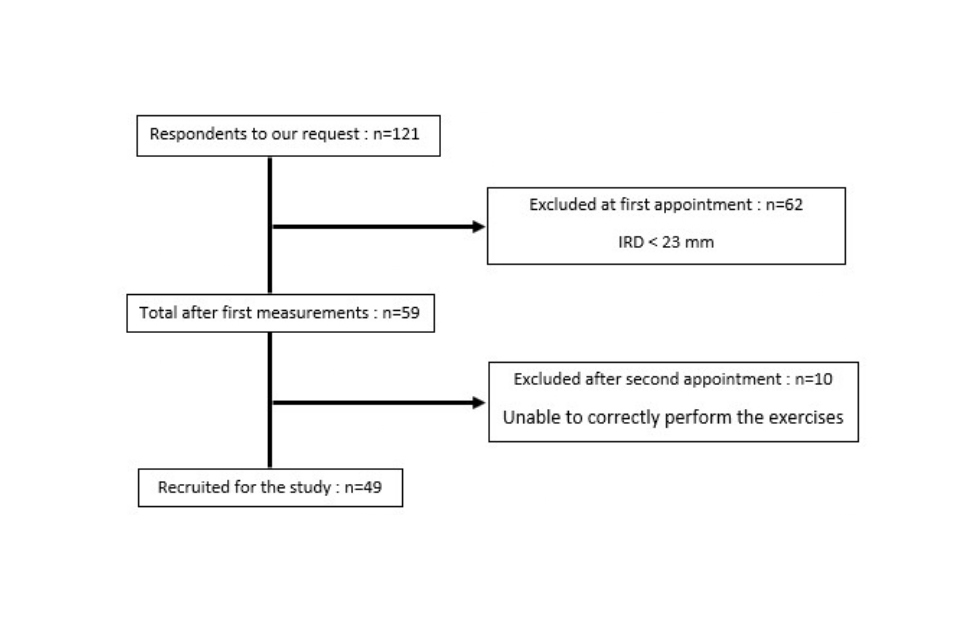
Figure 2. Participants recruitment flowchart.
|
Variables |
Values (Median±IQR) |
|
Age (years) |
30.9±7.0 |
|
Parity (child) |
2±1 |
|
Time since the last delivery (weeks) |
18±13 |
|
BMI (kg/m2) |
23.1±6.1 |
|
Skinfold (mm) |
12.4±9.3 |
|
Strength (0 – 5) |
3±1 |
|
Endurance (sec) |
56±39 |
|
Abbreviations: IQR: Interquartile Range; BMI: Body Mass Index. |
|
|
Conditions |
IRD (mm) |
Pairwise comparisons (Compared to Rest) |
||
|
Median |
IQR |
p-value |
r |
|
|
Rest |
26.7 |
9.5 |
- |
- |
|
Curl-up*† |
18.7 |
8.9 |
< 0.001 |
0.6 |
|
Drawing-in |
29.0 |
10.0 |
0.08 |
0.1 |
|
DA† |
26.0 |
8.5 |
0.1 |
0.1 |
|
Drawing-in+Curl-up*† |
22.9 |
9.7 |
< 0.001 |
0.3 |
|
DA+Curl-up*† |
21.8 |
9.3 |
< 0.001 |
0.4 |
|
Abbreviations: IRD: Interrecti Distance; IQR: Interquartile Range; DA: Diaphragmatic Aspiration. *Significant difference compared to Rest; *Significant difference compared to Drawing-in; p<0.05. r effect size=z√n |
||||
Discussion
Key findings
IRD values were measured 5 cm above the umbilicus with ultrasound in 49 Beninese postpartum women. Curl-up was the abdominal exercise during which IRD was the most reduced. Smaller significant IRD reductions were observed during Curl-up combinations with Drawing-in and DA. IRD was not modified during DA. A non-significant IRD increase was observed during Drawing-in practiced alone.
Characteristics of the sample
This study included Beninese postpartum women who gave birth 6 weeks to 6 months earlier. Out the 121 women approached, 59 were selected because they had an IRD greater than 23 mm, which corresponded to a diastasis recti prevalence of 49% very close to the prevalence (46%) observed in a recent study based on a similar population [5]. The participants in our study had a median strength of 3, similar to those reported in two other studies, one on a similar Beninese population [5], and the other on Chinese postpartum women [4]. According to Hislop et al. [38], an optimal strength corresponds to ratings of 4 and 5. This shows that postpartum women with diastasis recti have insufficient abdominal strength that deserves to be improved during the rehabilitation program. Similarly, compared to values measured in nulliparous women (65 to 117 seconds) [4,39,40,43], endurance values measured in postpartum women are poor, respectively 56 seconds in this study, 55 seconds in a previous one [5], and much lower values (8 to 15 seconds) in the study of Liaw et al. [4]. In this last study, the selected position for endurance evaluation was the level 3 of the manual testing rather than the level 2 in the current study.
IRD during Curl-up
At 5 cm above umbilicus, we observed a significant IRD decrease during Curl-up. This confirms that the Curl-up acutely decreases the IRD, whatever the measurement tool (ultrasound or calipers), the population (nulliparous, postpartum or parous women) and the measurement level above umbilicus [21,23-27,44]. The reduction of IRD during Curl-up can be explained by the straightening of the left and right rectus abdominis muscles from their arc-like orientation at rest [27]. Despite this systematic IRD reduction effect, the practice of Curl-up alone is not recommended due to its distortion effect on the linea alba [27,45]. Its combination with Drawing-in is rather advised in order to benefit from both the IRD reduction during Curl-up and the reduction of linea alba distortion during transversus abdominis activation.
IRD during Drawing-in and combination with Curl-up
IRD during Drawing-in (29.0 mm) was larger than during rest (26.7 mm) but this increase was not statistically significant. Published data regarding the effect of Drawing-in on IRD reported IRD increases either significant or not depending on the studies. Under umbilicus, significant IRD increases were systematically observed (references et population ?). Above umbilicus, both significant (reference) and non-significant (reference) IRD increases were reported in parous and postpartum women. Further studies are needed to clarify the acute effect of Drawing-in on the IRD.
During Drawing-in combined with Curl-up, a significant IRD reduction was observed contrary to the result of a previous study [44]. In that previous study, IRD was measured using calipers and the reference position was Head-lift rather than rest because a minimal rectus abdominis muscle contraction is required for IRD measurement with the calipers. This small contraction reduced IRD during Head-lift [21] which can explain the difference in results. Lee and Hodges [27] also observed a significant IRD reduction between rest and transversus abdominis activation combined with Curl-up at U point (just above umbilicus).
IRD during DA and combination with Curl-up
In our study, IRD did not change significantly during DA compared to rest, consistent with the results of two recent studies, one in postpartum women [28] and the other in men and nulliparous women [22]. The authors of this last study explained the lack of effect by the involuntary activation of transversus abdominis during hypopressive exercises, contrary to its voluntary activation during Drawing-in which increases the IRD below the umbilicus [21,24]. The effect of voluntary or involuntary activation of the transversus abdominis muscles on the IRD needs to be more investigated. In our opinion, the lack of difference between rest and DA could be explained by an IRD increase during the DA first phase (Drawing-in) followed by an IRD decrease during the second phase (aspiration phase - see DA instructions in Protocol). This hypothesis is supported by the observation that IRD was significantly smaller in DA compared to Drawing-in. During DA, IRD was reduced when the abdomen was pulled up during the aspiration, probably because the two rectus abdominis muscles come closer to each other due to the stretching of their fibers. Diaphragmatic aspiration performed without any belly Drawing-in could therefore potentially result in a significant IRD reduction. This should be further investigated bearing in mind that Drawing-in has been showed to reduce the linea alba distortion.
This study was the first to investigate the acute effect, on the IRD, of the combination of the DA with Curl-up, a rather complex movement requiring several learning sessions. This combination significantly reduced IRD compared to rest but this reduction was smaller than that observed during Curl-up alone. The same combination, unlike the Drawing-in+Curl-up combination, has recently been showed to promote less increase in intra-abdominal pressure and more pelvic floor muscles activation than Curl-up alone [31]. Combining DA with Curl-up appears therefore promising regarding postpartum rehabilitation as it seems to combine the positive effects of each exercise, IRD reduction due to Curl-up and intra-abdominal pressure reduction due to DA. Its acute effects on the linea alba distortion deserves to be studied, as well as its training effects on abdominal muscles strength and endurance, IRD reduction and linea alba stiffness.
Strength
This study investigated the acute effect of the combination of the Diaphragmatic aspiration with the Curl-up on the interrecti distance in postpartum women. Hypopressive exercises are increasingly offered to postpartum women, but their effects on the interrecti distance remain very little explored. Specifically, the combination of Diaphragmatic aspiration with Curl-up had never been studied before. This combination reduced the interrecti distance. Its effects on other aspects of abdominal function (strength, endurance, circumference, linea alba stiffness and distortion...) and pelvic floor (tonus, strength, endurance, urinary incontinence, organ prolapse...) deserve to be studied in the future.
Our study is focused on postpartum women diagnosed with diastasis recti and the selection was done using the IRD threshold developed from a population with similar characteristics [5]. The 6 exercises were performed in random order with standardized instructions. Ultrasonography has been shown to be a reliable and valid method to assess IRD [32-37], and the physiotherapist who conducted the measurements was trained for the use of this tool. All participants were trained in the various exercises of the study before data collection.
Limitation
The interrecti distance measurement was performed at a single level at 5 cm above umbilicus and only in supine position in this study, although the effect of exercises varies depending on the measurement level and position according to published data [21,23,24,27,30]. Then the results of this study cannot be applied to other measurement levels and positions. The inclusion criteria (IRD >23mm) were chosen considering the preliminary results of a previous study [5]. Further analysis of the data from this study showed that even women with an IRD smaller than 23 mm could be diagnosed with diastasis recti if they had a slack linea alba, an abdominal strength less than 3 and an abdominal endurance below 60 seconds. The inclusion of these women in the current study would possibly have allowed for a normal distribution of the data and the use of parametric statistical tests more likely to result in significant differences between exercises [46,47].
Clinical implications
Physiotherapists are regularly confronted with the management of the diastasis recti in postpartum women [48,49]. They resort to various exercises including Curl-up which is quite controversial because it has been shown to increase the linea alba distortion [27] and to be one of the exercises practiced by women suffering from pelvic floor disorders [50-52]. As an alternative, Drawing-in and hypopressives exercises are recommended in postpartum [27,29,53], although their effects on the diastasis recti are not clearly known. This study brings arguments in favor of the combination of Diaphragmatic Aspiration with Curl-up that acutely reduces the interrecti distance in postpartum women diagnosed with diastasis recti. The acute effects observed in this study encourage the initiation of a randomized clinical trial focused on the training effects of this combination on the interrecti distance.
Conclusion
This study investigated the acute effect of various abdominal exercises on the interrecti distance in Beninese postpartum women at 5 cm above umbilicus. The Diaphragmatic Aspiration had no effect on the interrecti distance. The interrecti distance was increased during Drawing-in and this increase was non-significant in comparison to rest but significant compared to Diaphragmatic Aspiration. The combination of Curl-up with Diaphragmatic aspiration or with Drawing-in slightly decreased the interrecti distance compared to rest but less than the decrease observed during Curl-up alone. These combinations deserve to be more studied to clarify their acute effect on the linea alba and their training effect on abdominal and pelvic floor function.
References
2. Mota P, Pascoal AG, Carita AI, Bø K. Normal width of the inter-recti distance in pregnant and postpartum primiparous women. Musculoskeletal Science and Practice. 2018 Jun 1;35:34-7.
3. Coldron Y, Stokes MJ, Newham DJ, Cook K. Postpartum characteristics of rectus abdominis on ultrasound imaging. Manual Therapy. 2008 Apr 1;13(2):112-21.
4. Liaw LJ, Hsu MJ, Liao CF, Liu MF, Hsu AT. The relationships between inter-recti distance measured by ultrasound imaging and abdominal muscle function in postpartum women: a 6-month follow-up study. Journal of Orthopaedic & Sports Physical Therapy. 2011 Jun;41(6):435-43.
5. Djivoh YS, Kpadonou T, Puttemans T, De Jaeger D. Diastasis recti in the Beninese population: Cross-sectional study from normal values to diagnosis. South African Journal of Physiotherapy. 2022 Nov 15;78(1):9.
6. Gruszczyńska D, Truszczyńska-Baszak A. Exercises for pregnant and postpartum women with diastasis recti abdominis–literature review. Advances in Rehabilitation. 2018;32(3):27-35.
7. Michalska A, Rokita W, Wolder D, Pogorzelska J, Kaczmarczyk K. Diastasis recti abdominis—a review of treatment methods. Ginekologia Polska. 2018;89(2):97-101.
8. Gluppe S, Engh ME, Bø K. What is the evidence for abdominal and pelvic floor muscle training to treat diastasis recti abdominis postpartum? A systematic review with meta-analysis. Brazilian Journal of Physical Therapy. 2021 Jul 21.
9. Mahalakshmi V, Sumathi G, Chitra TV, Ramamoorthy V. Effect of exercise on diastasis recti abdominis among the primiparous women: a quasi-experimental study. International Journal of Reproduction, Contraception, Obstetrics and Gynecology. 2016 Dec 1;5(12):4441-7.
10. Khandale SR, Hande D. Effects of abdominal exercises on reduction of diastasis recti in postnatal women. IJHSR. 2016 Jun;6(6):182-91.
11. Walton LM, Costa A, LaVanture D, McIlrath S, Stebbins B. The effects of a 6 week dynamic core stability plank exercise program compared to a traditional supine core stability strengthening program on diastasis recti abdominis closure, pain, oswestry disability index (ODI) and pelvic floor disability index scores (PFDI). Phys Ther Rehabil. 2016 Apr 11;3(1):3.
12. Acharry N, Kutty RK. Abdominal exercise with bracing, a therapeutic efficacy in reducing diastasis-recti among postpartal females. Int J Physiother Res. 2015;3(2):999-05.
13. Mesquita LA, Machado AV, Andrade AV. Physiotherapy for reduction of diastasis of the recti abdominis muscles in the postpartum period. Revista Brasileira de Ginecologia e Obstetrícia. 1999;21:267-72.
14. Thabet AA, Alshehri MA. Efficacy of deep core stability exercise program in postpartum women with diastasis recti abdominis: a randomised controlled trial. Journal of Musculoskeletal & Neuronal Interactions. 2019;19(1):62.
15. Gluppe SL, Hilde G, Tennfjord MK, Engh ME, Bø K. Effect of a postpartum training program on the prevalence of diastasis recti abdominis in postpartum primiparous women: a randomized controlled trial. Physical Therapy. 2018 Apr 1;98(4):260-8.
16. Theodorsen NM, Strand LI, Bø K. Effect of pelvic floor and transversus abdominis muscle contraction on inter-rectus distance in postpartum women: a cross-sectional experimental study. Physiotherapy. 2019 Sep 1;105(3):315-20.
17. Keshwani N, Mathur S, McLean L. The impact of exercise therapy and abdominal binding in the management of diastasis recti abdominis in the early post-partum period: a pilot randomized controlled trial. Physiotherapy Theory and Practice. 2021 Sep 2;37(9):1018-33.
18. Igwe SE, Okoye GC. Abdominal Exercises Enhance Closure Of Diastasis Recti Abdominis Condition And Improves Quality Of Life Among Women Who Have Undergone Multiple Pregnancies. Academic Journal of Current Research. 2020 Apr 30;7(4):36-45.
19. Tuttle LJ, Fasching J, Keller A, Patel M, Saville C, Schlaff R, et al. Noninvasive treatment of postpartum diastasis recti abdominis: a pilot study. Journal of Women’s Health Physical Therapy. 2018 May 1;42(2):65-75.
20. Ramírez-Jiménez M, Alburquerque-Sendín F, Garrido-Castro JL, Rodrigues-de-Souza D. Effects of hypopressive exercises on post-partum abdominal diastasis, trunk circumference, and mechanical properties of abdominopelvic tissues: a case series. Physiotherapy Theory and Practice. 2021 Nov 17:1-2.
21. Gluppe SB, Engh ME, Bø K. Immediate effect of abdominal and pelvic floor muscle exercises on interrecti distance in women with diastasis recti abdominis who were parous. Physical Therapy. 2020 Aug 12;100(8):1372-83.
22. Cuña-Carrera D, Soto-González M, Alonso-Calvete A, González-González Y, Lantarón-Caeiro EM. Immediate effects of different types of abdominal exercises on the inter-rectus distance. Isokinetics and Exercise Science. 2021 Jan 1;29(1):31-7.
23. Sancho MF, Pascoal AG, Mota P, Bø K. Abdominal exercises affect inter-rectus distance in postpartum women: a two-dimensional ultrasound study. Physiotherapy. 2015 Sep 1;101(3):286-91.
24. Mota P, Pascoal AG, Carita AI, Bø K. The immediate effects on inter-rectus distance of abdominal crunch and drawing-in exercises during pregnancy and the postpartum period. Journal of Orthopaedic & Sports Physical Therapy. 2015 Oct;45(10):781-8.
25. Pascoal AG, Dionisio S, Cordeiro F, Mota P. Inter-rectus distance in postpartum women can be reduced by isometric contraction of the abdominal muscles: a preliminary case-control study. Physiotherapy. 2014 Dec 1;100(4):344-8.
26. Chiarello CM, McAuley JA, Hartigan EH. Immediate effect of active abdominal contraction on inter-recti distance. Journal of Orthopaedic & Sports Physical Therapy. 2016 Mar;46(3):177-83.
27. Lee D, Hodges PW. Behavior of the linea alba during a curl-up task in diastasis rectus abdominis: an observational study. Journal of Orthopaedic & Sports Physical Therapy. 2016 Jul;46(7):580-9.
28. Arranz-Martín B, Navarro-Brazález B, Sánchez-Sánchez B, McLean L, Carazo-Díaz C, Torres-Lacomba M. The Impact of Hypopressive Abdominal Exercise on Linea Alba Morphology in Women Who Are Postpartum: A Short-Term Cross-Sectional Study. Physical Therapy. 2022 Aug;102(8):pzac086.
29. Caufriez M. Gymnastique Abdominale Hypopressive Online.
30. Ithamar L, de Moura Filho AG, Rodrigues MA, Cortez KC, Machado VG, de Paiva Lima CR, Moretti E, Lemos A. Abdominal and pelvic floor electromyographic analysis during abdominal hypopressive gymnastics. Journal of Body work and movement therapies. 2018 Jan 1;22(1):159-65.
31. Djivoh YS, De Jaeger D. Intra-abdominal and perineal pressures during abdominal exercises: A cross sectional study in postpartum women. Neurourology and Urodynamics. 2022 Oct 31.
32. Chiarello CM, McAuley JA. Concurrent validity of calipers and ultrasound imaging to measure interrecti distance. Journal of Orthopaedic & Sports Physical Therapy. 2013 Jul;43(7):495-503.
33. Rejano-Campo M, Pizzoferrato AC. Échographie en rééducation pelvi-périnéale: quelles applications?. Kinésithérapie, la Revue. 2021 Jan 1;21(229):25-32.
34. Van de Water AT, Benjamin DR. Measurement methods to assess diastasis of the rectus abdominis muscle (DRAM): a systematic review of their measurement properties and meta-analytic reliability generalisation. Manual Therapy. 2016 Feb 1;21:41-53.
35. Mota P, Pascoal AG, Sancho F, Bø K. Test-retest and intrarater reliability of 2-dimensional ultrasound measurements of distance between rectus abdominis in women. Journal of Orthopaedic & Sports Physical Therapy. 2012 Nov;42(11):940-6.
36. Keshwani N, McLean L. Ultrasound imaging in postpartum women with diastasis recti: intrarater between-session reliability. Journal of Orthopaedic & Sports Physical Therapy. 2015 Sep;45(9):713-8.
37. Keshwani N, Mathur S, McLean L. Validity of inter-rectus distance measurement in postpartum women using extended field-of-view ultrasound imaging techniques. Journal of Orthopaedic & Sports Physical Therapy. 2015 Oct;45(10):808-13.
38. Hislop H, Avers D, Brown M. Daniels and Worthingham's muscle Testing-E-Book: Techniques of manual examination and performance testing. Elsevier Health Sciences; 2013 Sep 27.
39. Fransoo P, Dassain C, Mattucci P. Mise en pratique du test de Shirado: Implementation of the Shirado test. Kinésithérapie, la Revue. 2009 Mar 1;9(87):39-42.
40. Ito T, Shirado O, Suzuki H, Takahashi M, Kaneda K, Strax TE. Lumbar trunk muscle endurance testing: an inexpensive alternative to a machine for evaluation. Archives of Physical Medicine and Rehabilitation. 1996 Jan 1;77(1):75-9.
41. Vispute SS, Smith JD, LeCheminant JD, Hurley KS. The effect of abdominal exercise on abdominal fat. The Journal of Strength & Conditioning Research. 2011 Sep 1;25(9):2559-64.
42. Fritz CO, Morris PE, Richler JJ. Effect size estimates: current use, calculations, and interpretation. Journal of Experimental Psychology: General. 2012 Feb;141(1):2.
43. Shrier I, Feldman D, Klvana J, Rossignol M, Abenhaim L. Comparison between tests of fatigue and force for trunk flexion. Spine. 2003 Jul 1;28(13):1373-8.
44. Djivoh YS, De Jaeger D. Acute effect of Sit-up versus Curl-up on the interrecti distance: A cross-sectional study in parous women. Progrès en Urologie. 2022 Sep 1;32(11):776-83.
45. Beamish N, Green N, Nieuwold E, McLean L. Differences in linea alba stiffness and linea alba distortion between women with and without diastasis recti abdominis: the impact of measurement site and task. Journal of Orthopaedic & Sports Physical Therapy. 2019 Sep;49(9):656-65.
46. Whitley E, Ball J. Statistics review 6: Nonparametric methods. Critical Care. 2002 Dec;6(6):1-5.
47. Ahsanullah M, Kibria BM, Shakil M. Normal distribution. InNormal and Student st Distributions and Their Applications 2014;7-50.
48. Sperstad JB, Tennfjord MK, Hilde G, Ellström-Engh M, Bø K. Diastasis recti abdominis during pregnancy and 12 months after childbirth: prevalence, risk factors and report of lumbopelvic pain. British Journal of Sports Medicine. 2016 Sep 1;50(17):1092-6.
49. Turan V, Colluoglu C, Turkuilmaz E, Korucuoglu U. Prevalence of diastasis recti abdominis in the population of young multiparous adults in Turkey. Ginekologia polska. 2011;82(11).
50. Salvatore S, Serati M, Laterza R, Uccella S, Torella M, Bolis PF. The impact of urinary stress incontinence in young and middle-age women practising recreational sports activity: an epidemiological study. British Journal of Sports Medicine. 2009 Dec 1;43(14):1115-8.
51. Fozzatti C, Riccetto C, Herrmann V, Brancalion MF, Raimondi M, Nascif CH, Marques LR, Palma PP. Prevalence study of stress urinary incontinence in women who perform high-impact exercises. International Urogynecology Journal. 2012 Dec;23(12):1687-91.
52. Simpson S, Deeble M, Thompson J, Andrews A, Briffa K. Should women with incontinence and prolapse do abdominal curls? International Urogynecology Journal. 2016 Oct;27(10):1507-12.
53. Madokoro S, Miaki H. Relationship between transversus abdominis muscle thickness and urinary incontinence in females at 2 months postpartum. Journal of Physical Therapy Science. 2019;31(1):108-11.