Abstract
Purpose: The exercise heart rate (HR)/oxygen uptake (VO2) relationship, expressed as beats/metabolic equivalent (MET), represents chronotropic efficiency (CE), a widely cited “normal value” ~10 beats/MET. This analysis examined the range of beats/MET values observed at peak oxygen uptake (VO2peak) in patients with and without heart failure and the impact of superimposed atrial fibrillation (AF) versus sinus rhythm (SR).
Methods: From Medline and Google Scholar searches, a database of 100 studies for SR and 46 for AF was identified. Study requirements included: 1. HRrest, 2. HRpeak and 3. Measured peak oxygen uptake i.e. VO2peak. From these data, the following were determined: (a) HR reserve (HRR) [HRpeak – HRrest], (b) For VO2peak, beats/MET equalled HRR/(peak METs -1) and (c) HR index (HRI) [HRpeak/HRrest].
Results: VO2peak, expressed as METs, was grouped from <4 METs to a maximum of >14 METs. For SR, beats/MET ranged from 14.9 ± 3.8 for VO2peak <4 METs to 8.9 ± 0.8 for VO2peak > 14 METs. For AF, beats/MET ranged from 20.5 ± 5.9 for VO2peak<4 METs to 15.1 ± 2.0 for a VO2peak range of 6.0–7.9 METs. For comparable MET ranges, beats/MET were 21% to 38% higher for AF than SR.
Conclusions: These unique findings establish a range of beats/MET, reflecting the considerable variability in CE in health and disease for VO2peak. The most compromised group was AF with heart failure, >20 beats/MET, compared with <9 beats/MET for elite endurance athletes. Future studies are needed to clarify the potential clinical utility and/or prognostic significance of this metric.
Keywords
Beats/MET, Heart rate reserve, Heart rate index, Sinus rhythm, Atrial fibrillation
Introduction
The adaptation of cardiac output (CO) to increasing exercise intensity can be compromised by atherosclerotic cardiovascular disease (ASCVD) resulting in reduced maximal or peak oxygen uptake (VO2peak). Within a physiological range of daily activities requiring multiples of the resting energy expenditure, expressed as 1 metabolic equivalent (MET) or 3.5 mLO2/kg/min) [1], the relationship between CO and oxygen consumption (VO2) is linear [2]. Stroke volume (SV) can be reduced from ASCVD or structural heart disease, with a failure to normally increase during exercise [3]. The primary compensatory mechanism to maintain an appropriate VO2 is an increase in heart rate (HR), together with blood volume redistribution and increased tissue extraction of oxygen [4–6].
Swain et al. have studied the relative relation between HR and VO2 for the purpose of exercise prescription using ?HR/?VO2 i.e. (HR activity – HR rest)/(METs activity – 1 MET) which, when applied to maximal performance, equals heart rate reserve (HRR)/(peak METs – 1), where HRR = HRpeak – HRrest [7,8]. This, by definition, represents “chronotropic efficiency” (CE), where the “beats/MET” increment also reflects the inotropic efficiency of the heart. With compromised cardiac function, “beats/MET” increases. This term is relevant to CO during incremental exercise, as it indicates the impact of altered SV, with the “normal” value for CE ~10 beats/MET [9,10].
Although chronotropic incompetence, (attenuation of the HR response to exercise) and heart rate recovery, HRR1min, (delayed HR decrease during exercise recovery) have been extensively studied to determine their potential prognostic utility, [11–13] few data are available regarding the impact of aging and ASCVD on CE. Progression of ASCVD can lead to heart failure (HF), with either reduced or preserved ejection fraction. Both are associated with increased mortality, stroke and hospitalization, which appears to be exacerbated by the transition from sinus rhythm (SR) to atrial fibrillation (AF) [14,15]. Several studies indicate that restoration of SR with catheter ablation reduces symptomatology, decreases hospitalization and increases survival [16–18].
The present analysis used a large exercise database to determine the impact of both SR and AF on CE, clarifying the range of beats/MET at VO2 peak associated with this disease-related common arrhythmia, with and without HF.
Methods
Methodology
This study employed a physiological data analysis using results (heart rate and oxygen uptake) extracted from previously published exercise studies meeting selected criteria, to clarify the heart rate/oxygen uptake relationship at VO2peak, expressed as “beats/MET”. To date, limited data are available regarding the variability in this metric. To assess the continuum in “beats/MET” in health and disease, a large database was constructed to evaluate the range in values of this variable as well as relevant potential modulators. Recognizing that heart rhythm was integral to methodology and outcomes, separate data sets were constructed for both SR and AF. Other possible influencers, including the level of cardiorespiratory fitness (VO2peak) and HF, were also examined.
Study selection
MEDLINE, Google Scholar and cross-referencing were used to identify exercise studies of SR and AF, with exercise or aerobic capacity determined during cycle ergometry, treadmill testing or both. For SR, a limit of 100 studies was set, involving subjects with and without ASCVD as well as structural heart disease. In the limited number of included HF studies (N = 19), methodology had to clearly state that subjects were in SR as AF was an exclusion criterion. For AF, 46 studies were identified, 17 of which involved HF. Suitability for the AF database included subjects that had chronic/permanent AF with no evidence of electrical pacing at the time of exercise testing. Paroxysmal AF was an exclusion criterion. To avoid redundancy or duplicative inclusions, study selections excluded publications having similar patient cohorts based on the date of publication or research canters involved. Details of the SR and AF studies used are shown in the Supplementary files.
Eligibility criteria
For eligibility for final selection, studies were required to have the following information:
1. Resting HR (HRrest), 2. Peak HR (HRpeak) and 3. Peak VO2 (VO2peak) as a direct measurement of VO2 expressed either as milliliters of oxygen per kilogram per minute (mL/kg/min) or as METs, determined by conventional gas analysis equipment. VO2 measurements were converted to METs using the definition of measured VO2/VO2rest with VO2rest equal to 3.5 mL O2/kg/min [1].
From group mean values of HRrest and HRpeak, both HRR [HRpeak – HRrest] and HR index (HRI), [HRpeak/HRrest] were calculated. A regression analysis of HRIpeak to VO2peak, expressed as METs was determined separately for SR and AF.
Statistical analyses
Categorical variables were expressed as numbers and percentages with continuous variables expressed as mean ± standard deviation. Student’s paired t test (2-tailed) was used to compare HR-derived and VO2 variables. Excel Data Analysis was used to determine the linear relationship (least squares method) of HRI to METs of VO2 data with the inclusion of the coefficient of determination (R2) and the standard error of the estimate (SEE).
Results
The demographics of the SR and AF databases are shown in Table1. (References and patient characteristics [age, gender, test methodology (e.g., treadmill, cycle ergometer), test protocol and clinical status] for SR and AF are listed in Supplementary Material).
|
Sinus Rhythm |
Atrial Fibrillation |
|
|
Studies |
100 |
46 |
|
Subjects (median per study) |
28,936 (68.5) |
3,452 (31.5) |
|
Age range years (median) |
10–70 (45.0) |
48–79 (64.8) |
|
Gender, %men |
70 |
74 |
|
Data Points |
228 |
97 |
|
Results expressed as total number for studies, number of subjects, age range in years, gender as %men and data points (combined submaximal and maximal). |
||
The most notable features relate to the larger number of subjects contributing to the SR database, 28,936 compared with 3,452 subjects in the AF database, and a more diverse age range for SR, 10–70 years, the median age being 45.0 years and for AF, a range from 48–79 years, with a median age of 64.8 years. Gender profiles were similar; SR, 70% men and AF, 74% men.
The limitation of VO2peak expressed as METs in AF versus SR is shown in the comparative histogram distribution below (see Figure 1).
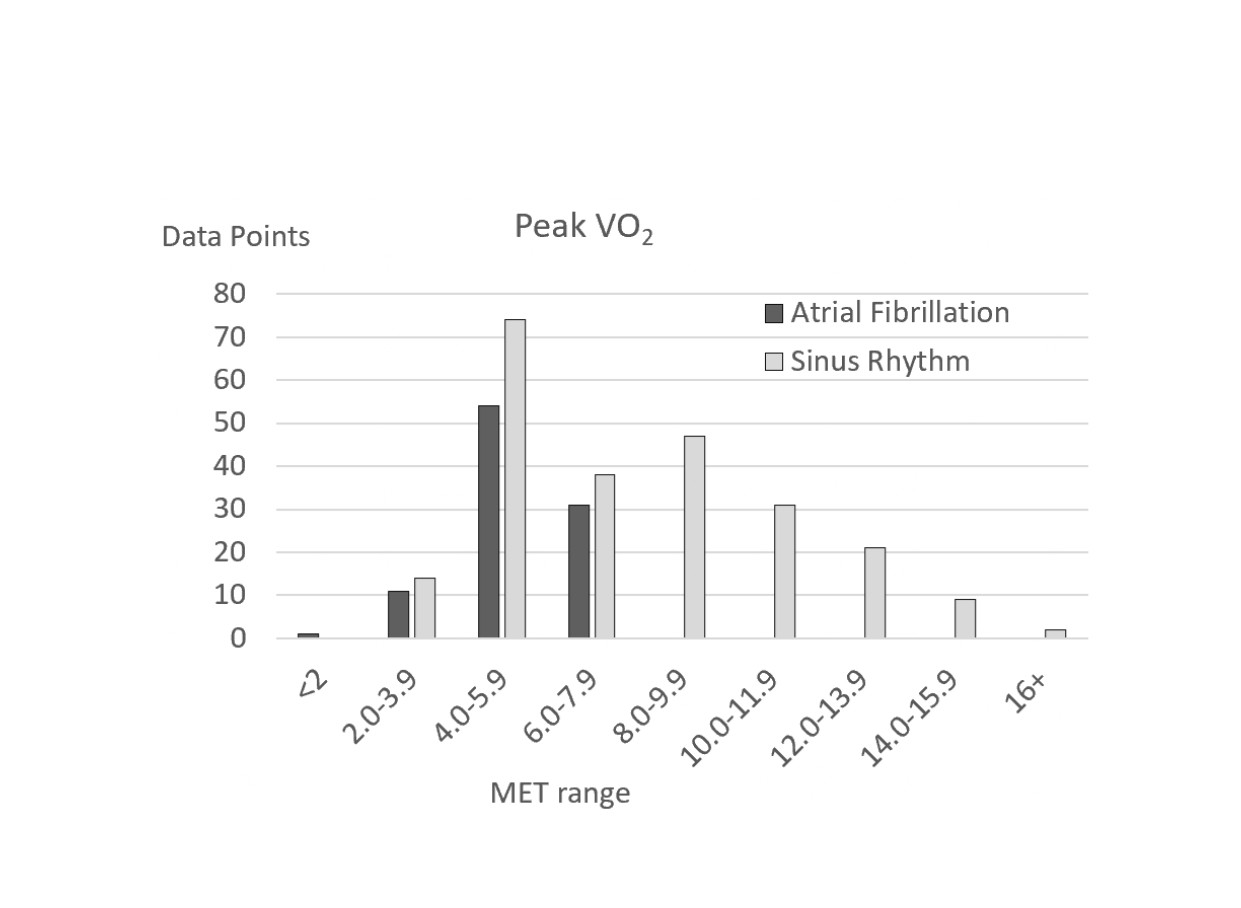
Figure 1. Exercise capacity expressed as Peak METs for sinus rhythm and atrial fibrillation (peak METs were expressed in increments of 1.9 METs and ranged from <2 METs to 16+ METs).
For AF, there was a total of 97 data points ranging from 1.4 METs to a maximum of 7.4 METs. By comparison, for SR with a total 228 data points, VO2peak ranged from 2.9 METs to 16.3 METs. The higher number of data points for both SR and AF in the 4.0–5.9 MET range related to the inclusion of HF studies to allow for a more comprehensive analysis of heart rhythm on CE. For VO2peak for both SR and AF, peak CE was calculated from the formula, (HRpeak – HRrest)/(VO2peak -1) expressed as beats/MET. Results for both SR and AF were grouped into seven V?O2peak categories ranging from <4 METs to >14 METs, the increment with each MET category being 1.9 METs, as shown in Table 2 and in graphic form in Figure 2.
|
MET range |
N |
HRR |
METs |
beats/MET |
|
Atrial Fibrillation <4 4.0-5.9 6.0-7.9 |
12 54 31 |
46.1 ± 16.2 67.6 ± 14.7 83.2 ± 10.6 |
3.3 ± 0.6 5.1 ± 0.6 6.5 ± 0.5 |
20.5 ± 5.9 16.5 ± 3.1 15.1 ± 2.0 |
|
|
|
|
|
|
|
Sinus Rhythm <4 4.0-5.9 6.0-7.9 8.0-9.9 10.0-11.9 12.0-13.9 14+ |
14 74 37 41 30 21 11 |
38.0 ± 8.5 51.6 ± 10.6 74.2 ± 13.2 92.8 ± 10.1 107.3 ± 14.1 120.5 ± 6.5 127.0 ± 10.8 |
3.6 ± 0.3 4.9 ± 0.6 6.9 ± 0.6 8.9 ± 0.6 10.8 ± 0.5 12.9 ± 0.7 15.4 ± 0.6 |
14.9 ± 3.8 13.3 ± 2.4 12.5 ± 1.8 11.8 ± 1.2 11.0 ± 1.2 10.2 ± 0.8 8.9 ± 0.8 |
|
Abbreviations: HRR: Heart Rate Reserve; MET: Metabolic Equivalent; beats/MET: Beats Per Metabolic Equivalent. N: number of data points; for METs and beats/MET values. Results are expressed as Mean ± SD. |
||||
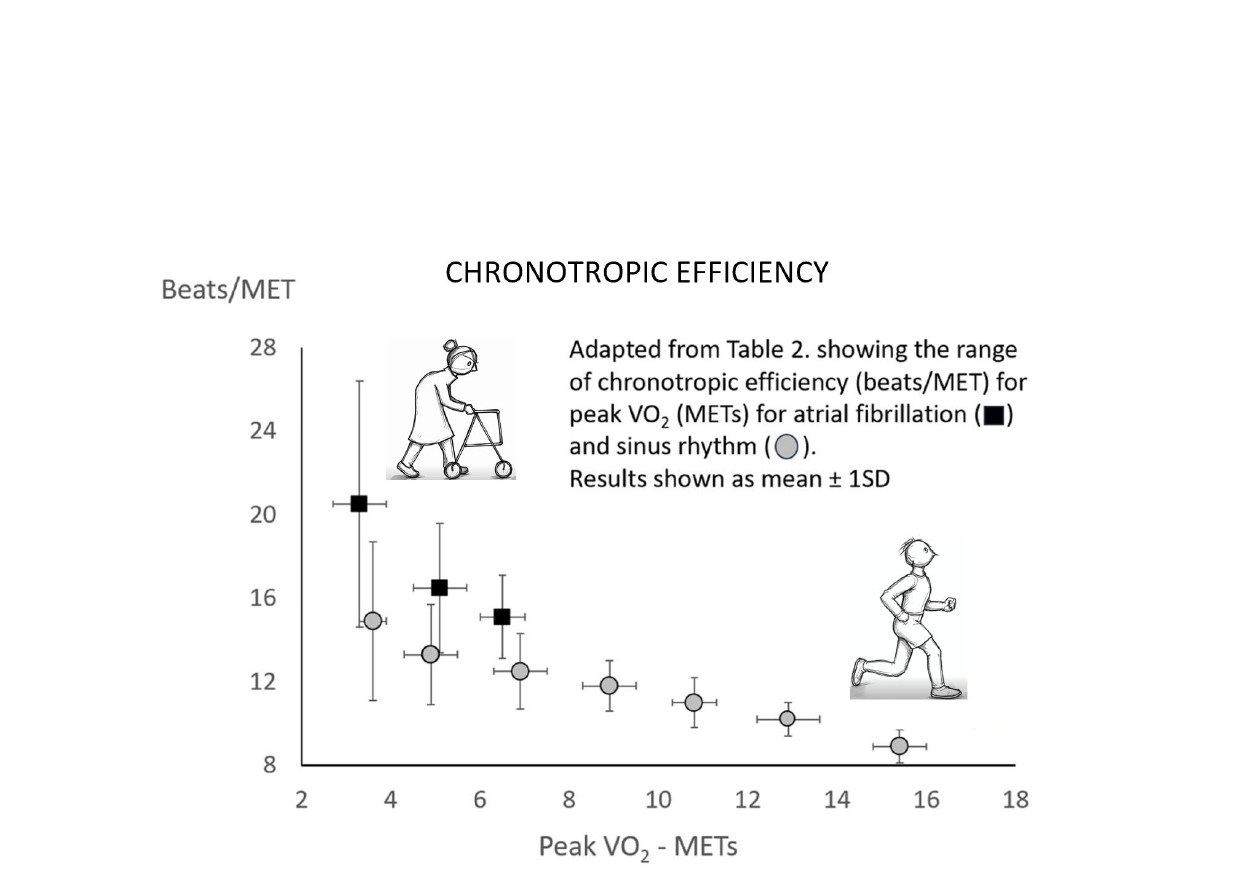
Figure 2. Chronotropic Efficiency.
Three MET ranges (< 4, 4.0–5.9 and 6.0–7.9 METs) are common to both AF and SR. For the lowest MET range, <4 METs, beats/MET was 37.6% greater for AF than SR with respective values being 20.5 ± 5.9 and 14.9 ± 3.8 beats/MET. For the 4.0–5.9 and 6.0–7.9 MET categories, the percentage difference was 24.1% and 20.8%, respectively. For both rhythms there is a decreasing gradient in beats/MET with increasing VO2peak MET category. For SR this decreases from 14.9 ± 3.8 beats/METs for the category of <4 METs to 8.9 ± 0.8 beats/MET for the 14+ METs category. For AF, beats/MET decreases from 20.5 ± 5.9 for < 4 METs to 15.1 ± 2.0 for the 6.0–7.9 MET category. Inclusion of HF studies in both heart rhythm databases provided a comparison of HR parameters, as shown in Table 3.
|
|
Sinus Rhythm |
Atrial Fibrillation |
P value |
|
Studies |
19 |
17 |
|
|
Data points |
54 |
26 |
|
|
HRrest |
75.9 ± 9.3 |
75.9 ± 7.1 |
0.98 |
|
HRpeak |
131.7 ± 15.3 |
131.4 ± 19.2 |
0.94 |
|
HRR |
55.8 ± 14.3 |
55.4 ± 16.5 |
0.92 |
|
METs |
5.2 ± 1.3 |
4.1 ± 0.9 |
<0.001 |
|
beats/MET |
13.6 ± 2.3 |
18.4 ± 5.1 |
<0.001 |
|
Abbreviations: HRrest: Resting Heart Rate; HRpeak: Peak Heart Rate; HRR: Heart Rate Reserve; METs: Metabolic Equivalents. Results expressed as Mean ± SD |
|||
In subjects with HF, although the HR values for HRrest, HRpeak and HRR for both SR and AF are remarkably similar, the mean MET and beats/MET results show highly significant differences. For V?O2peak METs, mean levels for SR and AF were 5.2 ± 1.3 and 4.1 ± 0.9 METs, respectively (P<0.001) and for beats/MET, respective levels for SR and AF were 13.6 ± 2.3 and 18.4 ± 5.1 (P<0.001). Linear regression of the relationship of VO2peak expressed as METs to HRI for both SR and AF is shown in Figure 3 (Figure 3a. Sinus rhythm, Figure 3b. Atrial fibrillation).
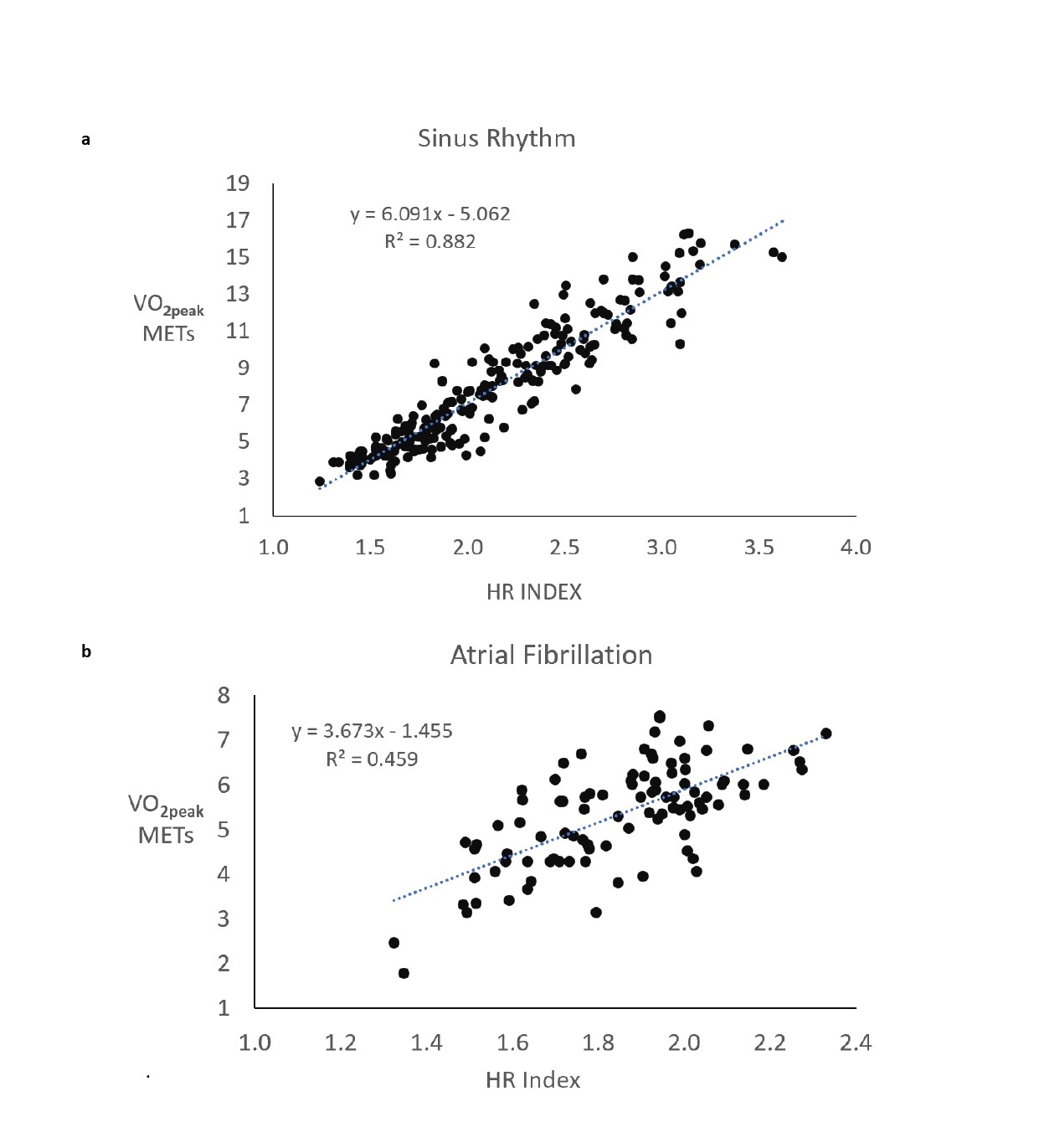
Figure 3. Linear regression of the relationship of VO2peak expressed as METs to HRI for both SR and AF. a) Sinus rhythm, b) Atrial fibrillation.
For SR, linear regression was 6.091x – 5.062 (R2 = 0.882, SEE 1.16 METs or 3.96 mL O2/kg/min.) and for AF, linear regression was 3.673x – 1.455 (R2 = 0.459, SEE 0.85 MET or 2.97 mL O2/kg/min).
Discussion
The present analysis evaluated the impact of cardiac rhythm, specifically SR versus AF, a common manifestation of ASCVD and/or structural heart disease, on CE expressed as beats/MET. Swain et al. presented data in the relative form of % ?HRR/% ?VO2, whereas in this study, results are expressed in absolute terms, HR for HRR and METs for ?VO2 [7, 8]. The authors conducted this investigation to clarify the variability associated with the simplistic generalization that the “normal” value of CE ~10 beats/MET [9,10].
Our findings show that as cardiac function is progressively compromised by disease, there is a reduction in VO2peak from normal age-related values. CE expressed as beats/MET increases, and concomitant AF further increases the magnitude of compromise.
For both SR and AF, with decreasing levels of VO2peak there is a commensurate increase in CE as beats/MET. As a linear relationship exists between CO and VO2 (Fick principle) this indicates that the higher HR associated with beats/MET is a mechanism compensating for a reduction in SV [19,20]. For SR, for the VO2peak category with greatest impairment, i.e. <4 METs, the corresponding value was 14.9 ± 3.8 beats/MET. For the highest VO2 peak category of >14 METs, the corresponding value was 8.9 ± 0.8 beats/MET. The gradient for AF was even greater, the <4 MET category having a corresponding value of 20.5 ± 5.9 beats/MET.
In determining the effect of heart rhythm on left ventricular performance, an analysis of the HRI/VO2 relationship was undertaken. The consistency of the HRI/VO2 relationship for SR is again shown in the results of this study with the linear regression equation reflecting previous studies [21,22]. For SR, 88.2% of the variance in VO2peak data (expressed as METs) is explained by HRI. By comparison, for AF the variance in VO2peak data was substantially lower at 45.9%. This difference between the SR and AF may be explained by abnormal cardiac function arising from AF which limits preload. In comparing the effect of SR and AF on men with HF, investigators reported a VO2peak 20% lower in patients with AF, the loss of atrial contraction being a major contributing factor [23]. For the AF/HF group, VO2peak was 13.8 mL/kg/min (3.9 METs) compared with 17.1 mL/kg/min (4.9 METs) in the SR/HF group, results similar to that shown in Table 3 derived from this study [23]. In AF, multiple mechanisms can compromise CO during exercise. These may include: shortened diastolic filling times which may lead to the development of tachycardia induced myopathy [17]; elevated left atrial and left ventricular filling pressures; impaired left ventricular relaxation and diastolic dysfunction; atrial and ventricular remodeling, fibrosis, and myopathy associated with chronicity [24]; and, increased mitral regurgitation, reported in a significant proportion of patients with chronic AF, [25–28] or combinations thereof.
As “beats/MET” at VO2peak has the potential to serve as a prognostic indicator, a comparison with chronotropic incompetence is of interest. However, for several reasons, this analysis was beyond the scope of our study. Different definitions of chronotropic incompetence based on the percentage of age-predicted maximal heart rate attained have been used in previous studies focused on prognosis [29]. Moreover, with the frequent use of beta-blockers in treating cardiovascular disease, particularly HF, the percentage of achieved age predicted maximal heart may be markedly attenuated and further influenced by the time of beta-blocker ingestion [30]. Alternative definitions, such as chronotropic index and metabolic reserve have been suggested. Finally, there is no current standard definition of chronotropic incompetence that applies to all cardiovascular disease states and adherence to prescribed pharmacological treatment agents may serve as an additional confounder.
Three relevant issues are pertinent to this discussion. First, AF may be symptomatic and limit physical activity. Data from two large scale studies, the Euro Heart Survey on Atrial Fibrillation (1,554 subjects with permanent AF) and the Orbit-AF study (2,054 subjects with persistent and long-standing persistent AF) reported associated symptoms in 55% to 62% of subjects [31,32]. Additionally, patients with AF are confronted with quality of life issues that may impact their medical management [33].
Second, whereas the safety and efficacy of catheter ablation in treating AF, most notably symptomatic paroxysmal AF and subsets with HF, has been reported [34–36], the overwhelming majority of people with chronic AF currently rely on optimal medical management of cardiac function and relevant comorbidities. Accordingly, Australia has an estimated population of 500,000 with chronic AF [37]. Recent Australian Medicare statistics listed 11,068 catheter ablations for 2024–2025, which represents ~ 2% of the total AF population [38].
Third, the safest and most effective methods for exercise testing and training in chronic AF have been reviewed [39]. A recent study of 86 patients with AF (mean age 69 years, 66% male, mean baseline VO2peak, 5.1 METs) compared high intensity interval training with moderate intensity continuous training [40]. No significant post-intervention differences between the two groups were observed in either a 6-minute walk test distance or quality of life measures. Dropouts were higher in the high intensity interval training group, and the authors noted the greater number of exercise-related complications (e.g., joint injuries) in this cohort [40]. Collectively, these data and other recent reports [41] suggest caution when initiating high intensity interval training in previous sedentary patients with known or suspected ASCVD, especially those with impaired left ventricular function (i.e., HF). The present findings extend these observations and suggest that in such patients with concomitant AF, CE is further compromised, suggesting the advisability of initiating more moderate exercise regimens in this patient subset, particularly in unsupervised, nonmedical settings.
Conclusions
The generalization that the HR/VO2 relation, reflected by CE ~10 beats/MET is applicable to a healthy untrained population, requires a broader perspective. With aerobic capacity ranging from severe functional impairment due to HF to high levels of cardiorespiratory fitness observed in elite endurance athletes, this metric required clarification in varied populations. The present study identified a range of CE from 8.9 beats/MET in trained athletes to 20.5 beats/MET in patients with severe HF and concomitant AF, reflecting the impact of health and disease on cardiac function, namely the interplay of CO and its determinants, HR and SV. Further research is warranted to determine whether this HR/VO2 derived variable, expressed as beats/MET, provides independent and additive prognostic significance that may be helpful in the management and risk stratification of patients with ASCVD and/or structural cardiac abnormalities.
Study Limitations
In using HR data from two databases, 100 studies for SR and 46 studies for AF, no attempt was made to discriminate the method for measurement of HR. HRrest may be recorded in a supine, seated, or standing position using various time intervals at rest before measurement. As such, this measurement lacks standardization. Similarly, HRpeak may relate to a single or time-averaged measurement. No specifications were placed on the method or timing of direct measurement of VO2peak, other than with conventional gas analysis equipment. As “beats/MET” can be considered a HR- derived variable, the authors arbitrarily labelled it “chronotropic efficiency”, acknowledging that this metric has been previously reported in the literature and is widely considered as ~10 beats/MET [9,10]. The present findings suggest that this value may vary considerably in health and disease, highlighting the modulating impact of VO2 peak, HF as well as heart rhythm (SR vs AF), either alone or in combination, with practical implications for exercise testing, training and prescription.
Conflict of Interest
There are no conflicts of interest for either of the authors related to this study. No funding was requested or received for this investigation.
Acknowledgements
The authors thank the staff of the Gold Coast University Hospital Library for their invaluable help in sourcing reference material.
References
2. Jones NL. Clinical Exercise Testing. 4th Edition. Philadelphia: WB Saunders; 1997.
3. Del Buono MG, Arena R, Borlaug BA, Carbone S, Canada JM, Kirkman DL, et al. Exercise Intolerance in Patients With Heart Failure: JACC State-of-the-Art Review. J Am Coll Cardiol. 2019 May 7;73(17):2209–25.
4. Yoshida S, Adachi H, Murata M, Tomono J, Oshima S, Kurabayashi M. Importance of compensatory heart rate increase during myocardial ischemia to preserve appropriate oxygen kinetics. J Cardiol. 2017 Sep;70(3):250–4.
5. Piña IL, Apstein CS, Balady GJ, Belardinelli R, Chaitman BR, et al. American Heart Association Committee on exercise, rehabilitation, and prevention. Exercise and heart failure: A statement from the American Heart Association Committee on exercise, rehabilitation, and prevention. Circulation. 2003 Mar 4;107(8):1210–25.
6. Wolsk E, Kaye DM, Komtebedde J, Shah SJ, Borlaug BA, Burkhoff D, et al. Determinants and consequences of heart rate and stroke volume response to exercise in patients with heart failure and preserved ejection fraction. Eur J Heart Fail. 2021 May;23(5):754–64.
7. Swain DP, Leutholtz BC. Heart rate reserve is equivalent to% VO2Reserve, not to% VO2max. Medicine & Science in Sports & Exercise. 1997 Mar;29(3):410–4.
8. Swain DP, Franklin BA. Counterpoint: theoretical and empirical basis for equating heart rate reserve with VO2 reserve. J Clin Exerc Physiol. 2021 Sep 1;10(3):97–101.
9. Fletcher GF, Ades PA, Kligfield P, Arena R, Balady GJ, Bittner VA, et al; American Heart Association Exercise, Cardiac Rehabilitation, and Prevention Committee of the Council on Clinical Cardiology, Council on Nutrition, Physical Activity and Metabolism, Council on Cardiovascular and Stroke Nursing, and Council on Epidemiology and Prevention. Exercise standards for testing and training: a scientific statement from the American Heart Association. Circulation. 2013 Aug 20;128(8):873–34.
10. Writing Committee, EACPR:, Guazzi M, Adams V, Conraads V, Halle M, Mezzani A, Vanhees L, et al. Clinical recommendations for cardiopulmonary exercise testing data assessment in specific patient populations. Eur Heart J. 2012 Dec 1;33(23):2917–27.
11. Lauer MS, Francis GS, Okin PM, Pashkow FJ, Snader CE, Marwick TH. Impaired chronotropic response to exercise stress testing as a predictor of mortality. JAMA. 1999 Feb 10;281(6):524–9.
12. Magrì D, Piepoli M, Gallo G, Fiori E, Correale M, Attanasio A, et al. Chronotropic incompetence across heart failure categories. Eur J Prev Cardiol. 2025 Aug 25;32(11):972–80.
13. Qiu S, Cai X, Sun Z, Li L, Zuegel M, Steinacker JM, et al. Heart Rate Recovery and Risk of Cardiovascular Events and All-Cause Mortality: A Meta-Analysis of Prospective Cohort Studies. J Am Heart Assoc. 2017 May 9;6(5):e005505.
14. Son MK, Park JJ, Lim NK, Kim WH, Choi DJ. Impact of atrial fibrillation in patients with heart failure and reduced, mid-range or preserved ejection fraction. Heart. 2020 Aug;106(15):1160–8.
15. Fauchier L, Bisson A, Bodin A. Heart failure with preserved ejection fraction and atrial fibrillation: recent advances and open questions. BMC Med. 2023 Feb 13;21(1):54.
16. Rattka M, Pott A, Kühberger A, Weinmann K, Scharnbeck D, Stephan T, et al. Restoration of sinus rhythm by pulmonary vein isolation improves heart failure with preserved ejection fraction in atrial fibrillation patients. Europace. 2020 Sep 1;22(9):1328–36.
17. Reddy YNV, Borlaug BA, Gersh BJ. Management of Atrial Fibrillation Across the Spectrum of Heart Failure With Preserved and Reduced Ejection Fraction. Circulation. 2022 Jul 26;146(4):339–57.
18. Cho Y, Oh IY, Park JJ, Oh BH, Jeon ES, Kim JJ, et al. Impact of successful restoration of sinus rhythm in patients with atrial fibrillation and acute heart failure: Results from the Korean Acute Heart Failure registry. Cardiol J. 2022;29(3):472–80.
19. Geerts BF, Aarts LP, Jansen JR. Methods in pharmacology: measurement of cardiac output. Br J Clin Pharmacol. 2011 Mar;71(3):316–30.
20. Agostoni P, Cattadori G, Vignati C, Apostolo A, Farina S, Salvioni E, et al. Deceived by the Fick principle: blood flow distribution in heart failure. Eur J Prev Cardiol. 2024 Dec 4;31(17):2001–10.
21. Wicks JR, Oldridge NB, Nielsen LK, Vickers CE. HR index--a simple method for the prediction of oxygen uptake. Med Sci Sports Exerc. 2011 Oct;43(10):2005–12.
22. Wicks JR, Oldridge NB, Franklin BA. Heart Rate Index-An Alternative Exercise-Based Equation for Estimating Peak VO 2. J Cardiopulm Rehabil Prev. 2025 Mar 1;45(2):139–45.
23. Pardaens K, Van Cleemput J, Vanhaecke J, Fagard RH. Atrial fibrillation is associated with a lower exercise capacity in male chronic heart failure patients. Heart. 1997 Dec;78(6):564–8.
24. Staerk L, Sherer JA, Ko D, Benjamin EJ, Helm RH. Atrial Fibrillation: Epidemiology, Pathophysiology, and Clinical Outcomes. Circ Res. 2017 Apr 28;120(9):1501–17.
25. Martin AC, Bories MC, Tence N, Baudinaud P, Pechmajou L, Puscas T, et al. Epidemiology, Pathophysiology, and Management of Native Atrioventricular Valve Regurgitation in Heart Failure Patients. Front Cardiovasc Med. 2021 Oct 25;8:713658.
26. Naser JA, Michelena HI, Lin G, Scott CG, Lee E, Kennedy AM, et al. Incidence, risk factors, and outcomes of atrial functional mitral regurgitation in patients with atrial fibrillation or sinus rhythm. Eur Heart J Cardiovasc Imaging. 2023 Oct 27;24(11):1450–7.
27. Bertrand PB, Schwammenthal E, Levine RA, Vandervoort PM. Exercise Dynamics in Secondary Mitral Regurgitation: Pathophysiology and Therapeutic Implications. Circulation. 2017 Jan 17;135(3):297–314.
28. Coisne A, Lancellotti P, Vannan MA. Mitral regurgitation, the left atrium and atrial fibrillation: unlikely bedfellows or natural kindreds? Eur Heart J Cardiovasc Imaging. 2024 Apr 30;25(5):587–8.
29. Brubaker PH, Kitzman DW. Chronotropic incompetence: causes, consequences, and management. Circulation. 2011 Mar 8;123(9):1010–20.
30. Zweerink A, van der Lingen AL, Handoko ML, van Rossum AC, Allaart CP. Chronotropic incompetence in chronic heart failure: a state-of-the-art review. Circulation: Heart Fail. 2018 Aug;11(8):e004969.
31. Nieuwlaat R, Capucci A, Camm AJ, Olsson SB, Andresen D, Davies DW, et al; European Heart Survey Investigators. Atrial fibrillation management: a prospective survey in ESC member countries: the Euro Heart Survey on Atrial Fibrillation. Eur Heart J. 2005 Nov;26(22):2422–34.
32. Freeman JV, Simon DN, Go AS, Spertus J, Fonarow GC, Gersh BJ, et al; Outcomes Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT-AF) Investigators and Patients. Association Between Atrial Fibrillation Symptoms, Quality of Life, and Patient Outcomes: Results From the Outcomes Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT-AF). Circ Cardiovasc Qual Outcomes. 2015 Jul;8(4):393–402.
33. Abu HO, Saczynski JS, Mehawej J, Tisminetzky M, Kiefe CI, Goldberg RJ, et al. Clinically Meaningful Change in Quality of Life and Associated Factors Among Older Patients With Atrial Fibrillation. J Am Heart Assoc. 2020 Sep 15;9(18):e016651.
34. Andrade JG, Champagne J, Deyell MW, Essebag V, Lauck S, Morillo C, et al; EARLY-AF Study Investigators. A randomized clinical trial of early invasive intervention for atrial fibrillation (EARLY-AF) - methods and rationale. Am Heart J. 2018 Dec;206:94–104.
35. Packer DL, Mark DB, Robb RA, Monahan KH, Bahnson TD, Moretz K, et al; CABANA Investigators. Catheter Ablation versus Antiarrhythmic Drug Therapy for Atrial Fibrillation (CABANA) Trial: Study Rationale and Design. Am Heart J. 2018 May;199:192–9.
36. Parwani AS, Kääb S, Friede T, Tilz RR, Bauersachs J, Frey N, et al. Catheter-based ablation to improve outcomes in patients with atrial fibrillation and heart failure with preserved ejection fraction: Rationale and design of the CABA-HFPEF-DZHK27 trial. Eur J Heart Fail. 2024 Oct;26(10):2203–12.
37. AIHW (Australian Institute of Health and Welfare) (2020) Atrial fibrillation in Australia, AIHW, Australian Government, accessed 21 April 2026.
38. Services Australia - Australian Government. Item Number, Medicare Statiistics 2024-25. 2025.
39. Keteyian SJ, Ehrman JK, Fuller B, Pack QR. Exercise Testing and Exercise Rehabilitation for Patients With Atrial Fibrillation. J Cardiopulm Rehabil Prev. 2019 Mar;39(2):65–72.
40. Reed JL, Terada T, Vidal-Almela S, Tulloch HE, Mistura M, Birnie DH, et al. Effect of High-Intensity Interval Training in Patients With Atrial Fibrillation: A Randomized Clinical Trial. JAMA Netw Open. 2022 Oct 3;5(10):e2239380.
41. Quindry JC, Franklin BA, Chapman M, Humphrey R, Mathis S. Benefits and Risks of High-Intensity Interval Training in Patients With Coronary Artery Disease. Am J Cardiol. 2019 Apr 15;123(8):1370–7.