Abstract
Introduction: Iron deficiency (ID), prevalent in 10.6% of heart failure with reduced ejection fraction (HFrEF) patients, has been linked to poorer clinical outcomes. The existing literature have provided insight into long-term impacts of the association, but the in-hospital outcomes remain unexplored. This study utilizes data from the National Inpatient Sample (NIS) to bridge this gap.
Method: NIS database for the years 2020 to 2022 was used to identify adult patients (aged ≥18 years) hospitalized with a primary diagnosis of HFrEF. Patients were further stratified based on the presence or absence of ID. Propensity score matching in a 1:1 ratio was performed using STATA, adjusting for age, sex, and relevant comorbidities. Univariate logistic and linear regression analyses were conducted before and after matching to assess clinical outcomes.
Results: Among 6,738,392 patients hospitalized with HFrEF from 2020 to 2022, 398,230 had comorbid ID, predominantly females and Blacks. After 1:1 propensity score matching, 52,930 pairs were analyzed. ID patients had higher rates of acute kidney injury (36.5% vs. 30.3%, OR: 1.30, P<0.001), blood transfusion (64% vs. 36%, OR: 1.89, P<0.001), and longer hospital stay (7.95 vs. 6.92 days, P<0.001). Despite greater resource utilization, they had lower in-hospital mortality (22.1% vs. 27.9%, OR: 0.67, P<0.001), cardiogenic arrest (10.14% vs. 11.17%, OR: 0.91, P=0.03), need for inotropes (5.18% vs. 6.40%, OR: 0.81, P=0.03), ECMO use (0.56% vs. 1.31%, OR: 0.42, P<0.001), and balloon pump insertion (4.3% vs. 6.1%, OR: 0.69, P<0.001).
Conclusion: ID in HFrEF patients is associated with increased rates of acute kidney injury, blood transfusion, and prolonged hospital stay. Despite greater resource utilization, patients with ID demonstrated significantly lower in-hospital mortality and fewer critical interventions. These findings underscore the complex clinical profile of HFrEF patients with concomitant ID and highlight the need for continued research to guide optimal management and improve patient outcomes.
Keywords
Iron deficiency, Heart failure with reduced ejection fraction, In-hospital outcomes, Resource utilization, Mortality, Length of hospital stay
Introduction
Heart failure (HF) is a common and serious clinical syndrome resulting from myocardial dysfunction, currently affecting an estimated 6.7 million Americans, with prevalence projected to rise to 8.5 million by 2030 [1,2]. HF is linked to preventable complications and a significant economic burden, underscoring the importance of studying its comorbidities. ID with or without anemia is a frequent comorbidity in patients with HFrEF, with a prevalence of approximately 55% in all heart failure patients [3]. In the context of heart failure, iron deficiency is diagnosed as ferritin level less than 100 ng/mL, or a ferritin level of 100–299 ng/mL along with a transferrin saturation (TSAT) less than 20% [4,5].
The development of ID in HF is initially driven by elevated hepcidin levels in the setting of systemic inflammation, which impairs iron release from enterocytes and the reticuloendothelial system [6]. With advancing heart failure, however, additional mechanisms contribute, including intestinal dysfunction secondary to mucosal edema, delayed gastric emptying, and impaired motility along with reduced dietary iron intake due to poor oral intake, collectively exacerbating the progression of ID [6–8].
In recent years, numerous studies have documented the impact of ID in patients with HFrEF. These studies demonstrated a higher mortality rate and lower quality of life in HFrEF patients with ID versus HFrEF patients without ID [9,10]. Other studies highlighted that in patients with HFrEF, ID was independently linked to lower peak oxygen uptake (VO2) and poorer ventilatory efficiency (higher VE/VCO2 slope), reflecting diminished exercise capacity [11,12].
While prior studies have documented the effects of ID in patients with HFrEF, there is a need for a larger retrospective analysis to comprehensively assess its impact on in-hospital mortality, resource utilization, and complications such as cardiogenic shock. Although one prior study evaluated this association using the NIS, the analysis was limited to a single year of data and limited outcomes, restricting the ability to capture broader national trends and outcomes. This study therefore seeks to address these gaps by evaluating the clinical outcomes, including morbidity and mortality, associated with the coexistence of ID and HFrEF using a nationally representative dataset. We hypothesized that the presence of iron deficiency in patients hospitalized with HFrEF would be associated with higher in-hospital mortality, greater healthcare resource utilization, and an increased risk of complications, including cardiogenic shock. These findings can help clinicians identify HFrEF patients with iron deficiency who may need closer monitoring for complications while guiding treatment decisions to optimize outcomes.
Methods
Data source
This retrospective study utilized data from the National Inpatient Sample (NIS) spanning January 2020 to December 2022. The NIS, part of the Healthcare Cost and Utilization Project (HCUP) and administered by the Agency for Healthcare Research and Quality (AHRQ), is the largest publicly accessible inpatient database in the U.S. It captures discharge data from a representative sample of hospitals and covers approximately 97% of the U.S. population. As all data are anonymized, this study was exempt from institutional review board (IRB) approval under HCUP’s data use agreement.
Study population
We included adult patients (≥18 years) hospitalized with a primary diagnosis of HFrEF, identified using ICD-10 codes ranging from I5020 to I5043. The cohort was then stratified based on the presence of ID with or with coexistent anemia, which was defined using ICD-10 codes D50, D508, and D509. Patients with missing demographic or clinical variables were excluded from the analysis.
Covariates and comorbidities
We assessed patient demographics (age, sex, race/ethnicity, income level, insurance status, and hospital characteristics such as region and bed size). Comorbid conditions were determined using ICD-10 coding algorithms and included hypertension, diabetes, hyperlipidemia, coronary artery disease, chronic kidney disease, and cerebrovascular disease. These factors were included in the propensity score model to account for potential confounding.
Outcomes
The primary outcome of interest was in-hospital mortality. Secondary endpoints included key inpatient complications such as cardiogenic shock, cardiac arrest, mechanical circulatory support (including intra-aortic balloon pump and ECMO), inotropic agent use, arrhythmias, acute kidney injury (AKI), and the need for blood transfusion. Health resource utilization was evaluated using hospital length of stay (LOS) and total hospitalization charges (TOTCHG), extracted through corresponding ICD-10 diagnosis/procedure codes and cost variables in the NIS.
Statistical analysis
To adjust for baseline differences between groups, we performed 1:1 propensity score matching using nearest-neighbor matching with a caliper width of 0.02, implemented in STATA. The matching process included demographic characteristics and key comorbidities. Adequate covariate balance post-matching was confirmed by non-significant p-values (>0.05) (Figure 1).
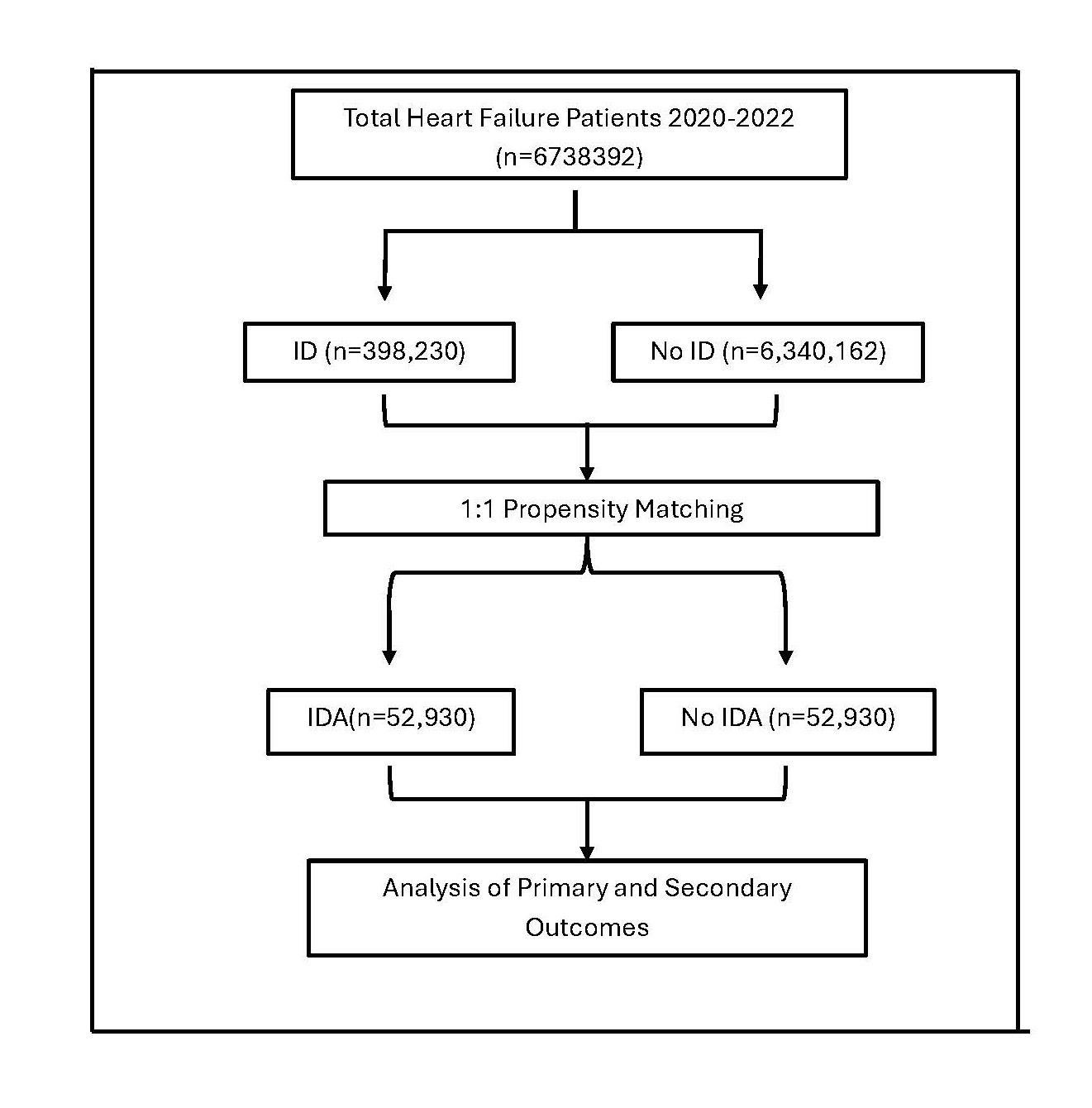
Figure 1. Schematics of study design.
We used chi-square tests for categorical comparisons and independent t-tests for continuous variables. Logistic regression models were applied to estimate odds ratios (ORs) and 95% confidence intervals (CIs) for binary outcomes, while linear regression models were used for continuous outcomes such as LOS and TOTCHG. A p-value <0.05 was considered statistically significant. All analyses were conducted using STATA.
Results
From 2020 to 2022, we identified a total of 6,738,392 adult hospitalizations for HFrEF across the United States. Among these, 398,230 cases (approximately 5.9%) had a concurrent diagnosis of ID. In the unmatched cohort, both groups were generally comparable, although patients with ID were slightly younger than those without (68.9 vs 69.2 years; MD=−0.24 years; 95% CI: −0.37 to −0.11; p<0.001). A higher proportion of ID patients were female (43.14% vs 36.26%; OR=1.33; 95% CI: 1.31 to 1.35; p<0.001) and Blacks (25.53% vs 9.97%; OR=1.37; 95% CI: 1.35 to 1.39; p<0.001). On the contrary, a smaller proportion of ID patients were Whites (60.38% vs 66.08%; OR=0.79; 95% CI: 0.77 to 0.80; p<0.001). Geographically, ID patients were more often admitted in the Midwest (26.41% vs 22.89%; OR=1.21; 95% CI=1.19 to 1.23; P<0.001). Regarding comorbidities, iron-deficient patients had significantly higher rates of DM (72.6% vs 69.0%; OR=1.21; 95% CI: 1.20 to 1.23; p<0.001) and chronic kidney disease (33.7% vs 29.9%; OR=1.19; 95% CI: 1.17 to 1.21; p<0.001), while lower rates of CVA (0.38% vs 0.46%; OR=0.82; 95% CI=0.73 to 0.46%;P=0.001) (Table 1).
|
Variable |
HFrEF and iron deficiency |
HFrEF and no iron deficiency |
Comparison |
|
|
Mean AGE |
68.94036 (68.77401 69.10671) |
69.18053 (69.09145 69.26961) |
-0.2401691 (-0.3665027 to -0.1138356, P<0.001) |
|
|
FEMALE |
171,779.9 (167954.7 175605.2) |
2,299,274 (2252697 2345850) |
1.333255 (1.312722 to 1.354109, P<0.001) |
|
|
RACE |
White |
240,451 (60.38%) |
4,189,579 (66.08%) |
.787113 .7757213 .798672, P<0.001) |
|
Blacks |
101,668 (25.53%) |
1,266,130(19.97%) |
1.368894 (1.346308 1.391859, P<0.001) |
|
|
Hispanics |
35,243 (8.85%) |
546,522 (8.62%) |
1.027367(1.00151 1.053891, P=0.038) |
|
|
Asian |
8,363(2.10%) |
143,288 (2.26%) |
.9257784 (.8802504 .9736612, P=0.003) |
|
|
Americans |
2,867(0.72%) |
42,479(0.67%) |
1.060674 (-.9732113 1.155997, P=0.180 |
|
|
Others |
9,677 (2.43%) |
151,530(2.39%) |
1.01559 (-0.000898 to .9689181 1.06451, P=0.519) |
|
|
HOSPITAL REGION |
Northeast |
70,566 (17.72%) |
1,085,436 (17.12%) |
1.042908 (1.023529 1.062654, P<0.001) |
|
Midwest |
105,172.49 (26.41%) |
1,451,263(22.89%) |
1.20926 (1.18974 1.229101, P<0.001) |
|
|
South |
156,305 (39.25%) |
2,636,239 (41.58%) |
0.907964 (0.8947674 0.9213552, P<0.001) |
|
|
West |
66,186 (16.62%) |
1,167,858 (18.42%) |
0.8825383 0.8657766 0.8996245, P<0.001) |
|
|
BEDSIZE |
Small |
79,248 (19.9%) |
1,331,434 (21.0%) |
0.9341446 .917574 .9510144, P<0.001) |
|
|
Medium |
105,690 (26.54%) |
1,748,885 (27.60%) |
.9478333 (0.9326133 0.9633016, P<0.001) |
|
|
Large |
213,292 (53.56%) |
3,258,209 (51.39%) |
1.090739 (1.075209 1.106494, P<0.001) |
|
PRIMAY PAYER |
Medicare |
269,840.5(67.76%) |
4,264,393 (67.26%) |
1.023636 (1.008091 1.039421, P=0.003) |
|
|
Medicaid |
58,500 (14.69%) |
809,005 (12.76%) |
1.17719 (1.153525 1.20134, P<0.001) |
|
|
HMO |
48,584 (12.2%) |
885,721(13.97%) |
0.8558154 (-0.8373456 0.8746926, P<0.001) |
|
|
Self-pay |
10,911.5(2.74%) |
187,035 (2.95%) |
0.9250348 (0.8853927 .966451, P<0.001 |
|
|
No charge |
717 (0.18%) |
12,680 (0.20%) |
0.9054961 (0.7658634 1.070587, P=0.2450) |
|
|
Other |
9,717 (2.42) |
180,695 (2.85%) |
0.8507247 (0.8122668 0.8910035, P<0.001 |
|
MEDIAN HOSEHOLD INCOME |
$1-$51999 |
141,929 (35.64%) |
2,127,124 (33.55%) |
1.094025 (1.077709 1.110587, P<0.001) |
|
|
$52000-$65999 |
104,814 (26.32%) |
1,694,091 (26.72%) |
.9784975 (-.9626237 .994633, P=0.009) |
|
|
$66000-$87999 |
87,411 (21.95%) |
1,432,877 (22.60%) |
.9623752 (-.9457695 .9792725, P<0.001) |
|
|
$88000 or more |
64,115 (16.10%) |
1,086,070 (17.13%) |
.927917 (-.9099034 .9462872, P<0.001) |
|
COMORBIDITIES |
DM |
289,349.9 (282,862 295,837.7) |
4,411,393 (4,319,852 4,502,934) |
1.2133 (1.196037 1.230812, P<0.001) |
|
|
HTN |
133,799.9 (130367.7 137,232.2) |
2,065,594 (2,020,983 2,110,205) |
1.047111 (1.031352 1.06311, P<0.001) |
|
|
HLD |
217,524.9 (215515.8 219,534) |
3,340,858 (3,308,883 3,372,833) |
1.08069 (1.065264 1.09634, P<0.001) |
|
|
CAD |
228,964.9 (223617.1 234,312.6) |
3,616,724 (3,540,585 3,692,862) |
1.018601 (1.003956 1.033459, P=0.013) |
|
|
CVA |
1,515 (1,337.214 to 1,692.786) |
29,454.98 (28,402.59 to 30,507.37) |
0.8181887 (0.7288123 0.9185256, P=0.001) |
|
|
CKD |
134,229.9 (130789.4 137,670.4) |
1,899,894 (1,857,726 1,942,062) |
1.188298 (1.170402 1.206468, P<0.001 |
In the unmatched analysis, patients with ID had significantly lower in-hospital mortality compared to non-ID patients (4.44% vs6.45%; OR = 0.67; 95% CI: 0.65 to 0.70; p<0.001). They also experienced lower rates of cardiac arrest (1.93% vs 2.68%; OR=0.71; 95% CI: 0.68 to 0.75; p<0.001), reduced need for inotropes (2.97% vs 3.14%; OR=0.92; 95% CI: 0.87 to 0.98; p=0.010), balloon pump insertion (0.80% vs 1.0%; OR = 0.80; 95% CI: 0.73 to 0.88; p<0.001), and ECMO use (0.10% vs 0.17%; OR=0.60; 95% CI: 0.46 to 0.75; p<0.001). However, ID was associated with significantly higher risk of acute kidney injury (38.45% vs 31.12%; OR=1.38; 95% CI: 1.36 to 1.40; p<0.001), increased need for blood transfusion (11.47% vs 5.64%; OR=2.17; 95% CI: 2.11 to 2.23; p<0.001), and greater hospital length of stay (7.95 vs 6.92 days; MD = 1.03 days; 95% CI: 0.95 to 1.11; p<0.001). Risk of cardiogenic shock (5.03% vs 5.12%; OR=0.98; 95% CI=0.94 to 1.02; P=0.399), risk of arrhythmia (16.85% vs 17.30%; OR=0.97; 95% CI=0.95 to 0.99; P=0.05) and total hospital charges were comparable between the two groups ($103847.4 vs $103411.7; mean difference =$435.52; 95% CI: −$1,364 to $2,235; p=0.635) (Table 2).
|
OUTCOME |
HFrEF with iron deficiency (N=398,230) |
HFrEF without iron deficiency (N=6,340,162) |
Mean Difference/ Odds Ratio |
P-value |
|
Mortality |
17,680 (4.44%) |
408,920 (6.45%) |
0.6738437 (95% CI 0.6497163 to 0.698867) |
P<0.001 |
|
LOS |
7.954196 |
6.923728 |
1.030468 (95% CI 0.9501994 to 1.110737) |
P<0.001 |
|
TOTCHG |
103,847.2 |
103,411.7 |
435.5207 (95% CI -1364.012 to 2235.053) |
P=0.635 |
|
Cardiogenic Shock |
20,045 (5.03%) |
324,720 (5.12%) |
0.9818848 (95% CI 0.9410238 to 1.02452) |
P=0.399 |
|
Cardiac arrest |
7,695 (1.93%) |
170,065 (2.68%) |
0.7148681 (95% CI 0.6790315 to 0.752596) |
P<0.001 |
|
Arrythmia |
67,115 (16.85%) |
1,096,575 (17.30%) |
0.9692397 (95% CI 0.9484588 to 0.9904758) |
P=0.05 |
|
Inotropic need |
11,715 (2.94%) |
200,800 (3.17%) |
0.926695 (95% CI 0.8747244 to 0.9817533) |
P=0.010 |
|
ECMO |
415 (0.10%) |
11,020 (0.17%) |
0.5991432 (95% CI 0.4756374 to 0.754719) |
P<0.001 |
|
Balloon pump |
3,195 (0.80%) |
63,525 (1.00%) |
0.7991308 (95% CI 0.7280133 to 0.8771955) |
P<0.001 |
|
AKI |
153,130 (38.45%) |
1,973,404 (31.12%) |
1.382484 (95% CI 1.360694 to 1.404622) |
P<0.001 |
|
Blood transfusion |
45,685 (11.47%) |
357,300 (5.64%) |
2.169878 (95% CI 2.111048 to 2.230347) |
P<0.001 |
After performing a 1:1 propensity score matching (n=52,930 per group), the comparative associations remained consistent. Iron-deficient patients had persistently lower odds of in-hospital mortality (22.0% vs 33.6%; OR=0.64; 95% CI: 0.60 to 0.68; p<0.001), cardiac arrest (10.14% vs 11.16%; OR=0.91; 95% CI: 0.87 to 1.05; p=0.03), inotrope use (5.19% vs 6.40%; OR=0.81; 95% CI: 0.66 to 0.99; p=0.038), balloon pump use (4.26% vs 6.11%; OR=0.69; 95% CI: 0.59 to 0.82; p<0.001), and ECMO (0.50% vs 1.31%; OR=0.42; 95% CI: 0.30 to 0.61; p<0.001). However, they remained at significantly increased risk for AKI (19.99% vs 16.83%; OR=1.31; 95% CI: 1.27 to 1.35; p<0.001), arrhythmias (82.47% vs 91.29%; OR=0.88; 95% CI: 0.84 to 0.93; p<0.001), and blood transfusion (63.91% vs 35.92%; OR=1.89; 95% CI: 1.71 to 2.09; p<0.001). Length of stay was significantly prolonged in the ID group (7.75 vs 7.21 days; MD=0.53; 95% CI: 0.34 to 0.72; p<0.001), while total hospital charges remained similar ($103021.5 vs $101962.2; MD=$1,052.31; 95% CI: −$6,712.68 to $8,817.30; p=0.791). Similarly, the risk of cardiogenic shock was comparable between the two groups (25.74% vs 26.87%; OR=0.96; 95% CI=0.83 to 0.99; P=0.332) (Table 3).
|
OUTCOME |
HFrEF with iron deficiency (N=52,930) |
HFrEF without iron deficency (N=52,930) |
Mean Difference/ Odds Ratio |
P-value |
|
Mortality |
11,665 (22.04%) |
17,815 (33.66%) |
0.638773 (95% CI 0.6005196 to 0.6794631) |
P<0.001 |
|
LOS |
7.746983 |
7.214071 |
0.5329125 (95% CI 0.3447565 to 0.7210684) |
P<0.001 |
|
TOTCHG |
103,021.5 |
101,969.2 |
1,052.313 (95% CI -6,712.675 to 8,817.302) |
P=0.791 |
|
Cardiogenic Shock |
13,625 (25.74%) |
14,220 (26.87%) |
0.9558864 (95% CI 0.8284564 to 0.9905287) |
P=0.332 |
|
Cardiac arrest |
5,365 (10.14%) |
5,910 (11.16%) |
0.9058752 (95% CI 0.8726243 to 1.047093) |
P=0.030 |
|
Arrythmia |
43,650 (82.47%) |
48,320 (91.29%) |
0 .8842637 (95% CI 0.8390446 to 0.9319198) |
P<0.001 |
|
Inotropic need |
2,745 (5.19%) |
3,390 (6.40%) |
0.80774 (95% CI 0.6603389 to 0.9880441) |
P=0.038 |
|
ECMO |
295 (0.50%) |
695 (1.31%) |
0.4238181 (95% CI 0.2956036 to 0.607644) |
P<0.001 |
|
Balloon pump |
2,255 (4.26%) |
3,235 (6.11%) |
0.6944601 (95% CI 0.5871499 to 0.8213827) |
P<0.001 |
|
AKI |
10,555 (19.99%) |
8,906 (16.83%) |
1.308095 (95% CI 1.267086 to 1.350432) |
P<0.001 |
|
Blood transfusion |
33,825 (63.91%) |
19,015 (35.92%) |
1.892992 (95% CI 1.71218 to 2.092893) |
P<0.001 |
Discussion
Summarization of results
In this large retrospective analysis of adults hospitalized with HFrEF using the NIS database (2020–2022), patients with ID demonstrated a paradoxically lower rate of in-hospital mortality and a slightly shorter length of stay compared with those without ID, despite similar hospitalization costs. Although the incidence of cardiac arrest was marginally lower in the ID cohort, these patients exhibited higher rates of arrhythmias and acute kidney injury (AKI). Furthermore, the use of advanced heart failure therapies, including inotropes, intra-aortic balloon pump (IABP), and extracorporeal membrane oxygenation (ECMO), was significantly lower among patients with ID. Collectively, these findings suggest that while ID may predispose to greater renal and arrhythmic complications, it is paradoxically associated with lower in-hospital mortality, shorter hospitalizations, and reduced reliance on advanced circulatory support interventions.
Explanation behind significant outcomes
The lower in-hospital mortality and shorter hospital stay among ID patients likely reflect differences in clinical management rather than a direct protective physiological effect. Patients with known ID often receive enhanced hemodynamic surveillance, timely blood transfusions, and intravenous iron supplementation, which collectively improve oxygen delivery and myocardial efficiency. These interventions facilitate earlier stabilization, reduce decompensations, and may account for the observed shorter hospitalizations and lower mortality. The reduced use of inotropes, IABP, and ECMO among ID patients may similarly represent a lower rate of worsening due to more careful observation and management. Moreover, clinicians may also adapt less aggressive management strategies, reflecting caution to avoid therapies that increase myocardial oxygen demand or bleeding risk in patients with reduced oxygen-carrying capacity [13].
Conversely, the higher incidence of AKI among ID patients may be attributed to compromised renal oxygenation and perfusion. ID reduces hemoglobin therefore decreasing arterial oxygen content, limiting oxygen delivery to the renal cortex and predisposing nephrons, especially within the outer medulla, to ischemic injury [14,15]. As medulla already works at maximum oxygen extraction capacity, even a small drop in oxygen leads to medullary hypoxia and ischemic stress. In the setting of HFrEF, these effects are compounded by elevated venous congestion, diuretic exposure, and activation of the renin–angiotensin–aldosterone system, collectively heightening renal vulnerability [16]. Similarly, chronic myocardial hypoxia in ID induced anemia can disrupt electrophysiologic stability, prolonging action potential duration and promoting atrial and ventricular arrhythmias [17].
Evidence from existing literature
The results of this study align with and extend prior research exploring ID’s impact on heart failure outcomes. Bess et al. (2024) reported reduced adjusted mortality, and shorter hospital stays among iron deficient HFrEF patients, attributing these trends to intensified monitoring and targeted correction of ID [18]. Goldenberg et al. (2017) observed increased ventricular arrhythmia risk in anemic patients with implantable cardioverter-defibrillators, supporting the hypothesis that impaired oxygen delivery promotes electrical instability [19]. In contrast, our finding of a slightly lower cardiac arrest rate diverges from Xu et al. (2019), who reported higher arrest rates in iron deficient patients with acute coronary syndrome and cardiogenic shock, underscoring that ID’s prognostic influence may differ between chronic and acute ischemic contexts [20,21].
Regarding renal outcomes, Han et al. (2015) demonstrated that anemia independently increases AKI risk in critically ill patients, consistent with our findings that renal hypoxia and hemodynamic stress underlie the elevated AKI rates observed [22]. Finally, our observation of lower utilization of inotropes, IABP, and ECMO parallels prior evidence that clinicians often withhold or delay invasive support in patients with anemia due to concerns about limited oxygen transport, increased bleeding risk, and uncertain benefit [23]. Together, these findings highlight the complex interaction between ID, organ-specific complications, and treatment intensity in patients with HFrEF, emphasizing the need for balanced, individualized care strategies.
Limitations
This study has limitations typical of administrative database analyses. Reliance on ICD-10 coding introduces potential misclassification, and the lack of laboratory data prevents confirmation of true biochemical iron deficiency or assessment of anemia severity. Medication details, transfusion practices, intravenous iron use, and timing of interventions are unavailable, limiting causal interpretation. The NIS captures hospitalizations rather than individual patients, precluding longitudinal follow-up or evaluation of readmissions. Residual confounding from unmeasured clinical factors is possible, and findings may be influenced by practice variations during the COVID-19 era. These limitations warrant cautious interpretation.
Conclusion
In this national cohort of adults hospitalized with HFrEF, iron deficiency was associated with lower in-hospital mortality, shorter length of stay, and reduced use of advanced circulatory support, despite higher rates of arrhythmias and acute kidney injury. Although we initially hypothesized that iron deficiency would be associated with worse in-hospital outcomes, the observed patterns suggest that these findings may reflect differences in clinical recognition, monitoring, and management intensity rather than a protective physiological effect of iron deficiency. These results highlight the clinical complexity of iron deficiency in heart failure and underscore the need for standardized inpatient screening and management pathways. Prospective studies incorporating laboratory parameters and treatment data are needed to better clarify the underlying mechanisms and optimize patient care.
Conflict of Interest
The authors have no conflict of interest to disclose.
Source of Funding
The authors involved in the formulation of this manuscript have not received any form of financial support from agencies in the public, commercial, or not-for-profit sectors.
Acknowledgment
None to declare.
Authorship Contribution Statement
Rohab Sohail: Conceptualization, Methodology, Validation, Formal analysis, Software, Writing-original draft and Writing-review and editing.
Ridda Khattak: Conceptualization, Project administration and Writing-original draft.
Zaraq Ahmad Khan: Conceptualization, Validation and Writing-original draft.
Hafsa Mansoor: Writing-original draft.
Madihah Alam: Writing-original draft.
Shahryar Chaudhry: Writing-Original draft.
Prakhar Anand: Writing-original draft.
Andrei Feldiorean: Writing-original draft
Vyom Patel: Writing-original draft.
Lindsey Marie Valdiviez: Writing-original draft.
Ibraheem Murtaza: Writing-original draft.
Sahil Desai: Visualization.
Joseph Deutsch: Writing-review and editing and Supervision.
References
2. Cheema B, Chokshi A, Orimoloye O, Ardehali H. Intravenous Iron Repletion for Patients With Heart Failure and Iron Deficiency: JACC State-of-the-Art Review. J Am Coll Cardiol. 2024 Jun 25;83(25):2674–89.
3. Lindberg F, Lund LH, Benson L, Linde C, Orsini N, Carrero JJ, Savarese G. Iron deficiency in heart failure: Screening, prevalence, incidence and outcome data from the Swedish Heart Failure Registry and the Stockholm CREAtinine Measurements collaborative project. Eur J Heart Fail. 2023 Aug;25(8):1270–80.
4. Graham FJ, Guha K, Cleland JG, Kalra PR. Treating iron deficiency in patients with heart failure: what, why, when, how, where and who. Heart. 2024 Sep 25;110(20):1201–7
5. Masini G, Graham FJ, Pellicori P, Cleland JGF, Cuthbert JJ, Kazmi S, et al. Criteria for Iron Deficiency in Patients With Heart Failure. J Am Coll Cardiol. 2022 Feb 1;79(4):341–51
6. McDonagh T, Macdougall IC. Iron therapy for the treatment of iron deficiency in chronic heart failure: intravenous or oral? Eur J Heart Fail. 2015 Mar;17(3):248–62
7. van der Wal HH, Grote Beverborg N, Dickstein K, Anker SD, Lang CC, Ng LL, et al. Iron deficiency in worsening heart failure is associated with reduced estimated protein intake, fluid retention, inflammation, and antiplatelet use. Eur Heart J. 2019 Nov 21;40(44):3616–25
8. Habeeb HA, Todd F, Valsalan R, Schembri E, Noyhar JK, Yip G, et al. Prevalence and Adverse Outcomes of Iron Deficiency in Heart Failure. Curr Cardiol Rev. 2025;21(5):e1573403X351268
9. Wienbergen H, Pfister O, Hochadel M, Fach A, Backhaus T, Bruder O, et al Long-term effects of iron deficiency in patients with heart failure with or without anemia: the RAID-HF follow-up study. Clin Res Cardiol. 2019 Jan;108(1):93–100.
10. von Haehling S, Doehner W, Evertz R, Garfias-Veitl T, Derad C, Diek M, et al. Ferric carboxymaltose and exercise capacity in heart failure with preserved ejection fraction and iron deficiency: the FAIR-HFpEF trial. Eur Heart J. 2024 Oct 5;45(37):3789–800.
11. Jankowska EA, Rozentryt P, Witkowska A, Nowak J, Hartmann O, Ponikowska B, et al. Iron deficiency predicts impaired exercise capacity in patients with systolic chronic heart failure. J Card Fail. 2011 Nov;17(11):899–906.
12. Alharbi A, Shah M, Bansal N, Franz A, Kwak ES, Alsughayer A, et al. Outcomes and complications of heart failure with iron deficiency anemia: a nationwide analysis. Hosp Pract (1995). 2024 Aug;52(3):84–90
13. Obradovic D, Loncar G, Zeymer U, Pöss J, Feistritzer HJ, Freund A, et al. Impact of anaemia and iron deficiency on outcomes in cardiogenic shock complicating acute myocardial infarction. Eur J Heart Fail. 2024 Feb;26(2):448–57.
14. Lombardi Y, Ridel C, Touzot M. Anaemia and acute kidney injury: the tip of the iceberg? Clin Kidney J. 2020 Dec 31;14(2):471–3.
15. Chávez-Iñiguez JS, Ibarra-Estrada M, Carmona-Morales EJ, Ron-Magaña A, Claure-Del Granado R, Velez JC, et al. Effect of Intravenous Iron Dextran on Kidney Outcomes in Acute Kidney Injury with Iron Deficiency: A Randomized Trial. Kidney360. 2026 Jan 27.
16. Kassianides X, Hazara AM, Macdougall IC, Kalra PA, Bhandari S. The Impact of Intravenous Iron on Renal Injury and Function Markers in Patients With Chronic Kidney Disease and Iron Deficiency Without Anemia. Kidney Int Rep. 2021 Nov 24;7(2):322–6.
17. Bakogiannis C, Mouselimis D, Tsarouchas A, Papadopoulos CE, Theofillogiannakos EK, Lechat E, et al. Iron therapy and severe arrhythmias in HFrEF: rationale, study design, and baseline results of the RESAFE-HF trial. ESC Heart Fail. 2023 Apr;10(2):1184–92.
18. Bess O, Quevedo Ramirez A, Shaka A, Oredipe O, Bello J, Shaka H. A Comparison of Outcomes in Heart Failure Patients with and without Iron Deficiency Anemia: A National Database Analysis. Circulation. 2024 Nov 12;150(Suppl_1):A4145056-.
19. Goldenberg I, Barsheshet A, Laish-Farkash A, Swissa M, Schliamser JE, Michowitz Y, et al. Anemia and the Risk of Life-threatening Ventricular Tachyarrhythmias from the Israeli Implantable Cardioverter Defibrillator Registry. Am J Cardiol. 2017 Dec 15;120(12):2187–92.
20. Xu T, Liang D, Wu S, Zhou X, Shi R, Xiang W, et al. Association of hemoglobin with incidence of in-hospital cardiac arrest in patients with acute coronary syndrome complicated by cardiogenic shock. J Int Med Res. 2019 Sep;47(9):4151–62
21. Minhas AMK, Sagheer S, Shekhar R, Sheikh AB, Nazir S, Ullah W, et al. Trends and Inpatient Outcomes of Primary Atrial Fibrillation Hospitalizations with Underlying Iron Deficiency Anemia: An Analysis of The National Inpatient Sample Database from 2004 -2018. Curr Probl Cardiol. 2022 Oct;47(10):101001.
22. Han SS, Baek SH, Ahn SY, Chin HJ, Na KY, Chae DW, et al. Anemia Is a Risk Factor for Acute Kidney Injury and Long-Term Mortality in Critically Ill Patients. Tohoku J Exp Med. 2015 Dec;237(4):287–95
23. Cherbi M, Levy B, Merdji H, Puymirat E, Bonnefoy E, Vardon F, et al. Hemoglobin in cardiogenic shock: the lower, the poorer survival. J Intensive Care. 2025 Jun 23;13(1):36.