Abstract
Introduction: Healthcare providers (HCPs) and traditional healers (THs) play a pivotal role in the breast cancer treatment pathway and can impact access to timely and effective healthcare. This study aimed to assess the knowledge, attitudes, and practices regarding breast cancer treatment among HCPs and THs in Northern Tanzania.
Methods: Employing a cross-sectional design, data were collected among 528 respondents (308 HCPs and 220 THs), using a validated questionnaire. Modified Poisson regression analysis was performed to determine the knowledge and attitudinal factors associated with referral status.
Results: Overall, referrals to health care facilities were 49.8% (263/528); for HCPs, 55.8% (172/308) and THs, 41.4% (91/220). Multivariable analysis revealed that HCPs who believed that cancer patients face administrative discrimination (aRR: 1.53; 95%CI: 1.25, 1.87), that a patient is responsible for their own disease (aRR: 1.26; 95%CI: 1.00, 1.60), and don’t disclose patient information to others (aRR: 1.24; 95%CI: 1.01, 1.52) were more likely to refer patients. THs who hesitated to speak with cancer patients (aRR; 0.42; 95%CI: 0.19, 0.97), thought that cancer patients are socially marginalized (aRR; 0.30; 95%CI: 0.15, 0.59), that cancer patients are avoided by friends (aRR: 0.62; 95%CI: 0.45, 0.86) and that a patient is responsible for their own disease (aRR: 0.45; 95%CI: 0.33, 0.62) were less likely to refer patients.
Conclusion: The findings underscore the need for targeted educational programs to address the knowledge gaps and attitudes regarding breast cancer among THs, which could enhance their understanding and improve their referral practices. Bridging the knowledge gaps between HCPs and THs is crucial for improving cancer treatment and referrals in Northern Tanzania.
Keywords
Breast cancer, Knowledge, Attitude, Practice, Health care providers, Traditional healers, Northern Tanzania
Introduction
Breast cancer (BC) continues to be a significant public health challenge in Tanzania, where the incidence has risen dramatically in recent years [1,2]. According to the Global Cancer Observatory (2020), breast cancer is the most common cancer among women in Tanzania after cervical cancer, with an estimated age-standardized incidence rate of 36.6 per 100,000 women and a mortality rate of 17.7 per 100,000 women [3]. In countries with a very high human development, index (HDI), such as Norway, The Netherlands and Sweden, 1 in 12 women will be diagnosed with breast cancer in their lifetime, and 1 in 71 women will die of it. However, in countries with a low HDI, such as SSA countries, 1 in 48 women will die from BC [4].
These statistics indicate a pressing need for effective intervention strategies to improve early detection and diagnosis [1,5]. Several factors contribute to late diagnoses, including a lack of awareness and knowledge of breast cancer among patients and healthcare providers (HCPs), limited resources in healthcare facilities [5], and sociocultural barriers impacting patients' perceptions of the disease. Research by Sakafu et al. highlighted that misconceptions regarding breast cancer and inadequate training among HCPs significantly contribute to delayed diagnosis, further exacerbating the challenges associated with managing the disease [6].
Traditional healers (THs) play a pivotal role in the Tanzanian healthcare system in the context of breast cancer awareness and treatment [7,8]. Patients often initially seek help from traditional healers due to pervasive cultural beliefs and trust in traditional medicine, frequently delaying their visits to formal healthcare facilities. This reliance on alternative medicine can contribute to stage progression at the time of eventual diagnosis. Studies by [9–11] have demonstrated that traditional healers often lack adequate knowledge of cancer symptoms and the importance of timely referrals to medical practitioners (as cited in: [7]). Moreover, despite the existence of traditional medicine regulations such as receipt of complaints by Registrar, preliminary inquiry, registrar to hold preliminary inquiry, where no prima-facie case is established, procedure for inquiry, notification and publication of decisions of the council, appeal against decision of the council and conduct derogatory to traditional and alternative health profession which are administered by the Minister of health and are enforced, many healers continue to operate in a context where formal training on diseases like breast cancer is minimal, ultimately affecting patient outcomes [12,13].
Given these findings, it is crucial to investigate the current knowledge, attitudes, and practices of both HCPs and THs regarding breast cancer management. Understanding these perspectives is foundational to developing interventions for HCPs and THs, which can improve their knowledge of breast cancer and their timely referrals for diagnosis. By addressing gaps in knowledge and practice, we also aim to promote enhanced collaboration between the traditional and formal health sectors for cancer care, ultimately reducing the mortality rates associated with breast cancer in Tanzania [12]. The significance of this study lies in its potential to contribute to the early detection, diagnosis, and treatment of breast cancer in Tanzania. The aims of this study were 1) to assess the knowledge, attitudes, and practices of HCPs and THs for breast cancer early detection, diagnosis, and treatment in Tanzania, and 2) to determine associations with their referral practices.
The insights gained from this study may guide policy formulation and develop practical interventions to improve THs and HCPs’ knowledge of breast cancer, promote collaboration between the traditional and formal health sectors and timely referrals for diagnosis potentially reducing the mortality rates associated with breast cancer in Tanzania.
Methods
Design
We conducted an analytical cross-sectional study among HCPs and THs in the Kilimanjaro region of Tanzania between November 2023 and April 2024. Using a survey questionnaire, we interviewed participants from both hospital and community settings. The hospitals were at zonal, regional, district and health care centre levels. These different levels were purposely selected for their varied capacities in patient care, staff expertise, and numbers of patients attending with breast cancer-related complaints.
Setting
Moshi Urban/Municipality, Moshi District, Rombo, Hai and Mwanga are five of the seven Districts of the Kilimanjaro region in Tanzania (Figure 1). The Kilimanjaro region, covering an area of about 15,100 square kilometers, is one of 31 regions of Tanzania, known for its stunning landscapes and as the home of Mount Kilimanjaro. It is bordered to the north by the Arusha Region and the border of Kenya, to the east by the Tanga Region, to the south by the Manyara Region, and to the west by the Singida Region. The Tanzanian national census of 2022 estimated a population size of 1,861,934 for the Kilimanjaro region. Most, 76.2 percent resided in rural areas, while 23.8 percent lived in urban areas with 954,298 (51.3%) being female and 907,636 (48.7%) being male [14]. As of 2022, the Kilimanjaro region is also the eighth most densely populated region with 124 people per square kilometer.

Figure 1. (a) Map of Tanzania showing the regions (Kilimanjaro region- study locations. (b) Map of Kilimanjaro region showing the study locations. Source: https://unitedrepublicoftanzania.com/geography-of-tanzania/regions-of-tanzania-history-geology-website/kilimanjaro-region-districts-history-geology-website/
Traditional healing (TH) in Tanzania is a deeply rooted practice that plays a significant role in the healthcare system, both in urban and rural settings, but predominantly in rural areas. TH refers to the use of indigenous knowledge, beliefs and practices passed down through generations to diagnose, treat and prevent some illnesses [15,16]. It also encompasses a holistic approach to health, addressing not just physical ailments but also spiritual, emotional, and social well-being. There are several types of traditional healers and treatments they use in Tanzania, including: Herbalists who specialize in the use of medicinal plants, extracts, powder, concoctions from roots, leaves, barks, and other natural substances. Furthermore, THs further offer dietary advice and lifestyle changes, based on traditional knowledge of body balance and wellness as well as protective charms and amulets, which are used to prevent illness or misfortune. Spiritual healers who use rituals, prayers, sacrifices, drumming, chanting or burning incense to cleanse spirits or wards off evil, divination, and ancestral communication to diagnose and treat spiritual or supernatural problems. Bone setters treat fractures and musculoskeletal problems. Diviners who use spiritual or mystical means to understand the causes of illness and recommend treatment [17–19].
Recruitment and sample
Between 8 November 2023 and 25 April 2024, using purposive sampling we enrolled HCPs aged 18 and older who had worked for more than two years in their current position, and signed informed consent to participate in the study. This enabled us to align our sample closely with the aims of our research, enhancing the relevance of our findings. HCPs from the Zonal, regional, district and health center facilities in the Kilimanjaro region were identified by the head doctors.
Due to the study team’s prior collaboration with the Traditional and Alternative Medicine Regional Coordinator, she was invited to assist with the recruitment of traditional healers. The Regional Coordinator, appointed by the Council for Traditional and Alternative Medicine Practitioners (CTAMP), is responsible for enforcing regulations, supporting practitioners, and monitoring compliance in accordance with the Traditional and Alternative Medicine Act [20]. Traditional healer selection was purposively based on willingness to participate, active involvement in the local CTAMP chapter, and adherence to organizational guidelines. Eligible participants were required to be registered with the Traditional and Alternative Health Practice Council of Tanzania and practice in Kilimanjaro region, be at least 18 years of age and be able to read and write in Swahili.
Survey questionnaire development
The survey questionnaire was developed by the authors based on information from the literature [21,22], the findings in a previous study [23], and input from experts, including oncologists, gynecologist, reproductive health nurses, and social scientists. Questions included knowledge of risk factors, common symptoms and signs of breast cancer, common methods of early detection, and current treatment modalities for the disease. Additional questions included attitudes towards women with breast cancer and referral practices for further investigations. The questionnaire was reviewed by oncologists in our institution, who were not among the authors. While the questionnaire was developed in English, it was translated into Swahili to facilitate participant understanding. This version was pilot-tested with 10 participants conveniently sampled from a local community from which the study participants were to be recruited. Research assistants received one day of training for the pilot study and one week for the entire study to familiarize themselves with the questions and proper interviewing techniques, and regular cross-checks were performed in the field to ensure data quality. As a result of this pre-test, some of the items on the questionnaire were discarded, mostly due to the ambiguity of those questions. Other questions were revised to ensure that the vocabulary was comprehensible to study participants while retaining the message of the questions. Of the initial 70 items, we retained eighteen core questions on knowledge of risk factors, twelve statements about
cancer, five statements regarding participants practices regarding breast cancer, fifteen items related to barriers to early detection and of perceived obstacles to treatment (Supplementary File).
Data collection
A purposive sampling method was used to recruit both HCPs and THs who expressed interest in participating in the study and were referred to the research assistant, who provided further details about the study and addressed any questions. Providers who chose to participate provided a written informed consent and then completed the questionnaire in a private conference room near the waiting area. Data collection for the entire study was conducted in Swahili by research assistants through face-to-face interactions with participants, and participants completed the self-administered surveys. To protect confidentiality, the questionnaires were anonymized by assigning numbers rather than using participants' names.
Measures
The questionnaire was organized into seven sections: 1) socio-demographic information, including age, education, religion, and marital status, years of experience; 2) knowledge about risk factors for developing breast cancer; 3) knowledge of breast cancer signs and symptoms; 4) attitude towards breast cancer; 5) practice towards breast cancer; 6) barriers to early detection, and 7) barriers to treatment (Supplementary File).
For knowledge of risk factors, each of the 18 items was a question about a risk for developing breast cancer, for example, “Does breast cancer risk increase with advancing age?”, “Can breast cancer be hereditary?”, or “Is high-fat diet a risk factor for breast cancer?”. Every item was scored on a 3-point scale, i.e. “yes”, “no” and “unsure”, with “yes” always being the correct answer.
Knowledge of signs & symptoms was measured with 12 statements about a breast cancer sign or symptom, for example, “Lump in the breast”,” Discharge from the breast”, or “Pain or Soreness in the breast”. Similar to knowledge or risk factors, items were scored on a 3-point scale, i.e., “yes”, “no”, and “unsure”, with “yes” as the correct answer.
Participants’ attitude regarding breast cancer was assessed by asking them to rate 11 specific statements on a 5-point Likert scale of: ‘strongly agree’, ‘agree’, ‘neither agree nor disagree’, ‘disagree’, or ‘strongly disagree’. The following 12 statements were included in the questionnaire: 1) Do you feel sympathy towards Cancer affected patients?, 2) Do you feel hesitant to speak with Cancer patients?, 3) Do you think that Cancer patients are socially marginalized?, 4)Do you think that Cancer patients are avoided by their friends?, 5) Do you think Cancer patients face administrative discrimination in terms of receiving govt. benefits?, 6) Do you think a patient is responsible for his own disease/fate?, 7) If you realize a patient has Cancer, will you disclose that information to others?, 8) If you realize a patient is receiving treatment for Cancer, will you disclose that information to others?, 9) Do you think Cancer patients should think less of themselves due to their condition?, 10) Do you think Cancer patients should be ashamed of themselves due to their condition?, 11) Would you be ashamed of yourself if diagnosed with Cancer?, 12) Is Cancer a serious disease?. Participants were asked to choose one of the following options for each of the statements above:
Participant’s practice regarding breast cancer was assessed by asking them to rate 5 specific statements on a 3-point scale i.e. “yes”, “no” and “unsure”, with “yes” as the correct answer. Following 5 statements were included in the questionnaire: 1)” If you think a patient has cancer, will you try to treat it yourself?”; 2) “If you think a patient has cancer, do you refer him/her to the next level facility e.g., District, Regional hospital? Or any other specialist physician?”; 3) “If you think a patient has Cancer, do you advise the patient to take cancer treatment?”; 4) “Do you educate people on breast cancer during clinic visits?”; 5) “Do you follow-up on a Cancer patient once she gets the official diagnosis?”.
Finally, barriers for detecting breast cancer, as well as perceived barriers to breast cancer treatment, were measured on a two-point scale (“yes”, or “no”) and 3-point scale (“yes”, “no” or “unsure”) respectively. The intent with both scales was to capture the respondents’ perceptions of the barriers and obstacles faced by men and women with any cancer in general. Fifteen barriers to detection were measured on a 3-point scale (“yes”, “no” or “unsure”). The barriers were grouped into three domains: individual, interpersonal and socio-cultural and health system. Examples of relevant questions from each domain include Individual: “Lack of money to pay for clinical consultations”, “Fear of finding something bad”, interpersonal and socio-cultural: “Resistance from a male partner about being checked by a doctor” and “Lack of family support”; and health system: “Long waits to obtain appointments for treatment”, “Fear of treatment side effects”.
Five questions on barriers to treatment were measured on a two-point scale (“yes” or “no”). The barriers were grouped into three domains: individual, interpersonal, and socio-cultural. For example, relevant questions from each domain include individual: “Lack of financial resources to pay for treatment”, “Lack of money to pay for transportation and lodging at the city where treatment is received”, interpersonal and socio-cultural factors: “Fear of treatment side effects” and “Lack of family support” (Supplementary File).
The main practical outcome was referral status, which was measured with a single item: “If you think a patient has Cancer, do you refer him/her to the next level facility e.g., District, Regional hospital? Or any other specialist physician?” rated on a 3-point scale, i.e. “yes”, “no” and “unsure”, with “yes” always being the correct answer (Supplementary File).
Data analysis
The data analysis was conducted using Stata version 18 (Stata Corp, College Station, TX). Categorical variables were summarized using frequencies and percentages, and the mean with standard deviation was used for continuous variables. The difference in proportion of referral status by participant characteristics was compared using a Chi-square test. Due to few responses for some items on the Likert scale, for analysis, ‘strongly agree’ and ‘agree’ were combined as “yes”; similarly, ‘disagree’, ‘strongly disagree’, and “neither agree nor disagree” were combined as “no”.
We used the chi-square test to compare knowledge of breast cancer risk factors, signs and symptoms among HCPs and THs.
The multivariable modified Poisson regression was used to determine the knowledge, attitudes, and socio-demographic factors associated with referral status. Independent variables that were significant in the bivariate model and important ones based on a literature review were included in the final model [21–23]. A P-value of <0.05 with a 95% confidence interval (CI) was considered statistically significant.
Results
A total of 528 participants (308 HCPs and 210 THs) were enrolled in this study, of which n=281, (53.2%) were male and n=247, (46.8%) were female. Ages ranged from 22 to 70 years (mean 37.97(±11.119)) for HCPs and 37 to 100 years (mean 63.38(±13.179)) for THs. While all the HCPs had a college/university level of education, most THs, n=164, (74.6%) had a primary school level education (Table 1).
|
Variable |
Health Care Providers (N=308) |
Traditional Healers (N=220) |
|
Mean Age (±SD) |
37.97 (±11.119) |
63.38 (±13.179) |
|
Minimum Age |
22 |
37 |
|
Maximum Age |
70 |
100 |
|
Age (Years) |
N (%) |
N (%) |
|
20-35 |
159 (51.62) |
0 (0.00) |
|
36-60 |
143 (46.43) |
106 (48.18) |
|
≥60 |
6 (1.95) |
114 (51.82) |
|
Sex |
||
|
Male |
143 (46.43) |
138 (62.73) |
|
Female |
165 (53.57) |
82 (37.27) |
|
Marital Status |
||
|
Single /Never married |
120 (39.0) |
39 (17.7) |
|
Married/Living together |
177 (57.5) |
110 (50.0) |
|
Divorced/Separated/Widowed |
11 (3.5) |
71 (32.3) |
|
Education Level |
||
|
Never attended school |
0 |
49 (22.27) |
|
Primary |
0 |
164 (74.55) |
|
Secondary level |
0 |
5 (2.27) |
|
College/University |
308 (100%) |
2 (0.91) |
|
Level of higher Education |
||
|
Certificate |
51 (16.56) |
|
|
Diploma |
151 (49.03) |
|
|
BSc |
85 (27.60) |
|
|
MSc |
21 (6.82) |
|
|
Residence |
||
|
Urban |
162 (52.60) |
42 (19.01) |
|
Rural |
149 (47.40) |
178 (80.01) |
|
Religion |
||
|
Christian |
270 (87.66) |
65 (29.55) |
|
Muslim |
38 (12.34) |
155 (70.45) |
|
Hospital Working |
||
|
Zonal referral |
67 (21.75) |
|
|
Regional referral |
29 (9.42) |
|
|
District |
130 (42.21) |
|
|
Health Centre |
82 (26.62) |
|
|
Professional |
||
|
Medical doctor |
144 (46.8) |
|
|
Nurses |
164 (53.3) |
|
|
Unit of Work |
||
|
Cancer Care Centre |
17 (5.5) |
|
|
Emergency Department |
98 (31.8) |
|
|
Obstetrics and Gynecology |
61 (19.8) |
|
|
Surgical Department |
42 (13.6) |
|
|
Medical Department |
59 (19.2) |
|
|
Pediatric Department |
30 (9.7) |
|
|
Eye/ENT Department |
1 (0.3) |
|
|
Years of Practice |
||
|
1-4 |
0 |
0 |
|
5-9 |
90 (29.22) |
8 (3.64) |
|
10-15 |
56 (18.18) |
55 (25.00) |
|
16-20 |
46 (14.94) |
37 (16.82) |
|
≥21 |
116 (37.66) |
120 (54.55) |
Two of the enrolled 310 HCPs did not complete the survey due to time constraints. A total of 308 HCPs and 220 THs finally completed the survey.
Knowledge of risk factors
Most n=262, (85.06%) of HCPs had knowledge about the risk of advancing age on breast cancer. The majority (91.88%) were aware that hormone replacement therapy increases the risk of breast cancer.
Fewer than one-fifth (20%) of THs knew that menarche below 11 years was a risk factor for breast cancer and were knowledgeable about having first child at age more than 30 years being a risk factor for breast cancer (Figure 2).
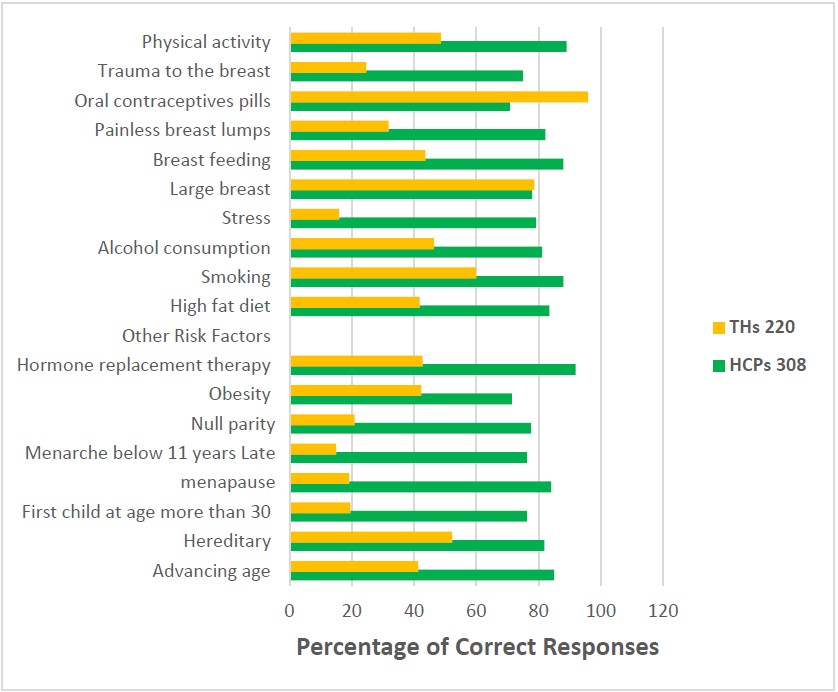
Figure 2. Showing responses and knowledge of breast cancer risk factors of participants (N=528).
Knowledge of the signs and symptoms of breast cancer
The results also highlighted a significant gap in knowledge between the two providers regarding various breast cancer symptoms.
Notably, the top four symptoms recognized by THs are ulceration of the breast 144 (65.45%); swelling or enlargement of the breast 141 (64.09%); inversion/pulling in of nipple 127 (57.73%) and lump in the breast 111 (50.45%). While the three least recognized symptoms by THs included weight loss 62 (28.18%); lump under the armpit 70 (31.82%) and scaling/dry skin on nipple region 83 (37.73%). However, the top four symptoms reported by HCP were lump in the breast 299 (97.08%); discharge from the breast 280 (90.91%); pain or soreness in the breast 271 (87.99%) and swelling or enlargement of the breast 269 (87. 34%). Inversion/pulling in of nipple 221 (71.75%); weight loss 224 (72.73%); change in the size of the breast 228 (74.03%) and ulceration of the breast 229 (74.35%) the other known symptoms for HCPs (Figure 3).
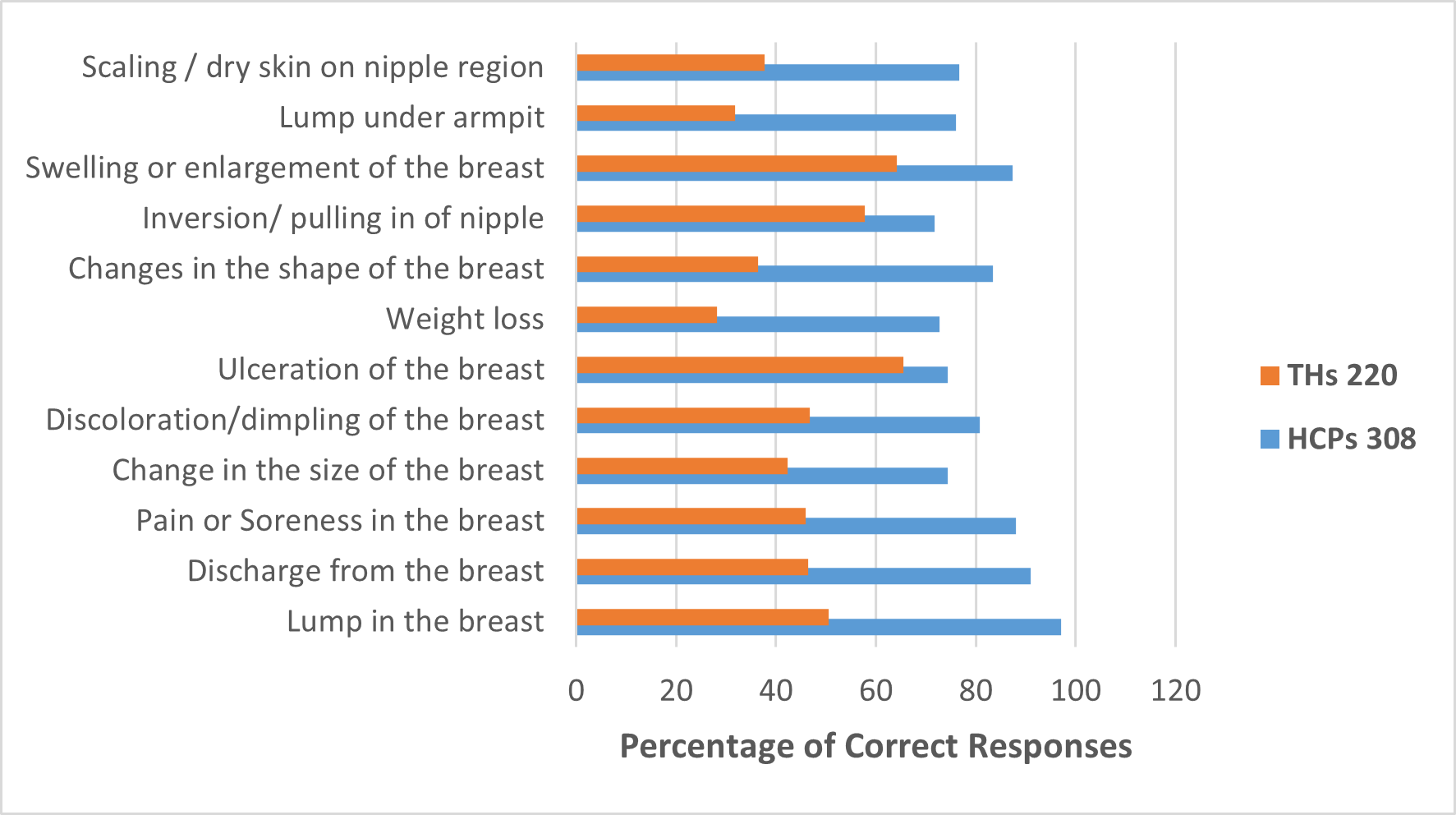
Figure 3. Showing responses and knowledge of breast cancer signs and symptoms of participants (N=528).
Changes in breast shape and nipple inversion were widely recognized by HCPs n=257, (83.44%) and n=221, (71.75%) respectively), but less so among THs, n=80, (36.36%) and n=127, (57.73%), respectively), both demonstrating significant differences. Moreover, swelling or enlargement of the breast was identified by n=269, (87.34%) of HCPs, with n=141, (64.09%) of THs acknowledging this symptom. Lastly, the presence of a lump under the armpit was noted by n=234, (75.97%) of HCPs, contrasted with only n=70, (31.82%) of THs, and scaling or dry skin in the nipple area was recognized by n=236, (76.62%) of HCPs, compared to just n=83, (37.73%) of THs (Figure 3).
Attitudes of HCPs towards breast cancer
In bivariate analysis, HCPs who thought cancer patients are not socially marginalized (54.3%, P-value; 0.045); that patients are not avoided by their friends (56.8%, P-value; 0.005); patients are responsible for their own disease/fate (69.6%, P-value; <0.001), and patients should think less of themselves (100%, P-value; 0.028) were more likely to refer them to the healthcare facilities (Table 2).
|
Variable |
Total |
Referral |
P-value |
|
|
Yes |
No |
|||
|
Afraid of Cancer patients |
||||
|
No (Disagree) |
303 (98.4) |
169 (55.8) |
134 (44.2) |
0.850 |
|
Yes (Agree) |
5 (1.6) |
3 (60.0) |
2 (40.0) |
|
|
Feel hesitant to speak with Cancer patients |
||||
|
No (Disagree) |
306 (99.4) |
172 (56.2) |
134 (43.8) |
0.111 |
|
Yes (Agree) |
2 (0.6) |
0 (0.0) |
2 (100.0) |
|
|
Cancer patients are socially marginalized |
||||
|
No (Disagree) |
248 (80.5) |
139 (56. 0) |
117 (44.0) |
0.045 |
|
Yes (Agree) |
60 (19.5) |
124 (45.7) |
148 (54.3) |
|
|
Cancer patients are avoided by their friends |
||||
|
No (Disagree) |
149 (43.4) |
130 (55.6) |
99 (44.4) |
0.005 |
|
Yes (Agree) |
159 (51.6) |
133 (44.5) |
166 (55.5) |
|
|
Cancer patients face administrative discrimination in terms of receiving govt. benefits |
||||
|
No (Disagree) |
304 (98.7) |
171 (56.2) |
133 (43.8) |
0.211 |
|
Yes (Agree) |
4 (1.3) |
1 (25.0) |
3 (75.0) |
|
|
Cancer patient is responsible for his own disease/fate |
||||
|
No (Disagree) |
193 (62.7) |
92 (47.7) |
101 (52.3) |
<0.001 |
|
Yes (Agree) |
115 (37.3) |
80 (69.6) |
35 (30.4) |
|
|
Disclose that a patient has Cancer to others |
||||
|
No (Disagree) |
262 (85.1) |
142 (54.2) |
120 (45.8) |
0.165 |
|
Yes (Agree) |
46 (14.9) |
30 (65.2) |
16 (34.8) |
|
|
Disclose that a patient is receiving treatment for Cancer to others? |
||||
|
No (Disagree) |
305 (99.0) |
170 (55.7) |
135 (44.3) |
0.704 |
|
Yes (Agree) |
3 (1.0) |
2 (66.7) |
1 (33.3) |
|
|
Cancer patients should think less of themselves due to their condition |
||||
|
No (Disagree) |
303 (98.1) |
166 (55.0) |
136 (45.0) |
0.028 |
|
Yes (Agree) |
6 (1.9) |
6 (100.0) |
0 (0.0) |
|
|
Cancer patients should be ashamed of themselves due to their condition |
||||
|
No (Disagree) |
303 (98.4) |
167 (55.1) |
136 (44.9) |
0.045 |
|
Yes (Agree) |
5 (1.6) |
5 (100.0) |
0 (0.0) |
|
|
Ashamed of yourself if diagnosed with Cancer |
||||
|
No (Disagree) |
220 (71.4) |
117 (53.2) |
103 (46.8) |
0.137 |
|
Yes (Agree) |
88 (28.6) |
55 (62.5) |
33 (37.5) |
|
|
Cancer disease is very serious |
|
|
|
|
|
No (Disagree) |
31 (10.1) |
17 (54.8) |
14 (45.2) |
0.905 |
|
Yes (Agree) |
277 (89.9) |
155 (56.0) |
122 (44.0) |
|
|
Variable |
Total n (%) |
Referral |
P-value |
|
|
Yes |
No |
|||
|
Afraid of Cancer patients |
||||
|
No (Disagree) |
212 (96.4) |
89 (41.9) |
123 (58.1) |
0.338 |
|
Yes (Agree) |
8 (3.6) |
2 (25.0) |
6 (75.0) |
|
|
Feel hesitant to speak with Cancer patients |
||||
|
No (Disagree) |
211 (95.9) |
87 (41.2) |
124 (58.8) |
0.848 |
|
Yes (Agree) |
9 (4.1) |
4 (44.4) |
5 (55.6) |
|
|
Cancer patients are socially marginalized |
||||
|
No (Disagree) |
8 (3.6) |
5 (62.5) |
3 (37.5) |
0.216 |
|
Yes (Agree) |
212 (96.4) |
86 (40.6) |
126 (59.4) |
|
|
Cancer patients are avoided by their friends |
||||
|
No (Disagree) |
80 (36.4) |
44 (55.0) |
36 (45.0) |
0.002 |
|
Yes (Agree) |
140 (63.6) |
47 (33.6) |
93 (66.4) |
|
|
Cancer patients face administrative discrimination in terms of receiving govt. benefits |
||||
|
No (Disagree) |
125 (56.8) |
51 (40.8) |
74 (59.2) |
0.846 |
|
Yes (Agree) |
95 (43.2) |
40 (42.1) |
55 (57.9) |
|
|
A Cancer patient is responsible for his own disease/fate |
||||
|
No (Disagree) |
68 (30.9) |
43 (63.2) |
25 (36.8) |
<0.001 |
|
Yes (Agree) |
152 (69.1) |
48 (31.6) |
104 (68.4) |
|
|
Disclose that a patient has Cancer to others |
||||
|
No (Disagree) |
159 (72.3) |
66 (41.5) |
93 (58.5) |
0.943 |
|
Yes (Agree) |
61 (27.7) |
25 (41.0) |
36 (59.0) |
|
|
Disclose that a patient is receiving treatment for Cancer to others |
||||
|
No (Disagree) |
153 (69.5) |
65 (42.5) |
88 (57.5) |
0.610 |
|
Yes (Agree) |
67 (30.5) |
26 (38.8) |
41 (61.2) |
|
|
Cancer patients should think less of themselves due to their condition |
||||
|
No (Disagree) |
141 (64.1) |
67 (47.5) |
74 (52.5) |
0.013 |
|
Yes (Agree) |
79 (35.9) |
24 (30.4) |
55 (69.6) |
|
|
Cancer patients should be ashamed of themselves due to their condition |
||||
|
No (Disagree) |
207 (94.1) |
83 (40.1) |
124 (59.9) |
0.128 |
|
Yes (Agree) |
13 (5.9) |
8 (61.5) |
5 (38.5) |
|
|
Ashamed of yourself if diagnosed with Cancer |
||||
|
No (Disagree) |
121 (55.0) |
53 (43.8) |
68 (56.2) |
0.417 |
|
Yes (Agree) |
99 (45.0) |
38 (38.4) |
61 (61.6) |
|
|
Cancer disease is very serious |
||||
|
No (Disagree) |
6 (2.7) |
1 (16.7) |
5 (83.3) |
0.213 |
|
Yes (Agree) |
214 (97.3) |
90 (42.1) |
124 (57.9) |
|
For the HCPs, the multivariable modified Poisson regression analysis, revealed that the belief that a patient is responsible for their own disease (aRR=1.26, P-value=0.047), the view that cancer patients face administrative discrimination (aRR=1.53, P-value<0.001) and disclosing information about a patient receiving cancer treatment (aRR=1.24, P-value=0.039) were positive associated with referral (Table 4).
|
Variable |
cRR |
P-value |
aRR |
P-value |
|
Afraid of Cancer patients |
||||
|
No (Disagree) |
1 |
|
1 |
|
|
Yes (Agree) |
1.07 (0.52–2.21) |
0.843 |
1.17 (0.94–1.47) |
0.165 |
|
Cancer patients are socially marginalized |
||||
|
No |
1 |
|
1 |
|
|
Yes |
1.17 (0.94–1.47) |
0.749 |
0.89 (0.73–1.09) |
0.259 |
|
Cancer patients are avoided by their friends |
||||
|
No |
1 |
|
1 |
|
|
Yes |
0.97 (0.81–1.17) |
0.749 |
0.56 (0.11–2.95) |
0.496 |
|
Cancer patients face administrative discrimination |
||||
|
No |
1 |
|
1 |
|
|
Yes |
0.44 (0.0.8–2.44) |
0.351 |
1.53 (1.25–1.87) |
<0.001 |
|
A cancer patient is responsible for his own disease/fate |
||||
|
No |
1 |
|
1 |
|
|
Yes |
1.46 (1.21–1.77) |
<0.001 |
1.26 (1.00–1.60) |
0.047 |
|
Disclose information that patient has Cancer |
||||
|
No |
1 |
|
1 |
|
|
Yes |
1.20 (0.95–1.53) |
0.129 |
1.24 (0.60–2.59) |
0.55 |
|
Disclose information that patient is receiving treatment for Cancer |
||||
|
No |
1 |
|
1 |
|
|
Yes |
1.20 (0.53–2.68) |
0.664 |
1.24 (1.01–1.52) |
0.039 |
|
Be ashamed of yourself if diagnosed with Cancer |
||||
|
No |
1 |
|
1 |
|
|
Yes |
1.18 (0.96–1.44) |
0.121 |
0.92 (0.66–1.27) |
0.606 |
|
Cancer disease is very serious |
||||
|
No |
1 |
|
1 |
|
|
Yes |
1.02 (0.73–1.43) |
0.906 |
0.29 (0.03–2.45) |
0.256 |
Attitudes associated with the referral of breast cancer among traditional healers
In the bivariate analysis, among THs, referral of breast cancer patients to healthcare facilities was positively associated with the belief that a patient is responsible for their own disease fate (cRR=1.46, P-value<0.001) and negatively associated with the belief that cancer patients face administrative discrimination (cRR=0.44, P-value=0.351). No other variables were significantly associated with the referral of breast cancer patients to healthcare facilities.
In the multivariable analysis (Table 5), THs were less likely to refer patients if they thought Cancer patients are socially marginalized (cRR=0.30, aRR=0.30, P-value<0.001), that Cancer patients are avoided by their friends (cRR=0.62, aRR=0.62, P-value=0.004) and that a patient is responsible for their own disease/fate (cRR=0.45, aRR=0.45, P-value< 0.001).
|
Variable |
cRR |
P-value |
aRR |
P-value |
|
Afraid of Cancer patients |
||||
|
No (Disagree) |
1 |
|
1 |
|
|
Yes (Agree) |
0.60 (0.18) |
0.402 |
0.81 (0.25–2.60) |
0.719 |
|
Feel hesitant to speak with Cancer patients |
||||
|
No |
1 |
|
1 |
|
|
Yes |
1.08 (0.51–2.28) |
0.845 |
0.42 (0.19-0.97) |
0.042 |
|
Cancer patients are socially marginalized |
||||
|
No |
1 |
|
1 |
|
|
Yes |
0.54 (0.34–0.86) |
0.010 |
0.30 (0.15–0.59) |
<0.001 |
|
Cancer patients are avoided by their friends |
||||
|
No |
1 |
|
1 |
|
|
Yes |
0.61 (0.45–0.83) |
0.002 |
0.62 (0.45–0.86) |
0.004 |
|
Cancer patients face administrative discrimination |
||||
|
No |
1 |
|
1 |
|
|
Yes |
1.03 (0.75–1.42) |
0.846 |
0.87 (0.64–1.18) |
0.362 |
|
A cancer patient is responsible for his own disease/fate |
||||
|
No |
1 |
|
1 |
|
|
Yes |
0.50 (0.37–0.67) |
<0.001 |
0.45 (0.33–0.62) |
<0.001 |
|
Disclose information that a patient has Cancer |
||||
|
No |
1 |
|
1 |
|
|
Yes |
0.99 (0.69–1.41) |
0.944 |
0.89 (0.63–1.26) |
0.515 |
|
Disclose information that a patient is receiving treatment for Cancer. |
||||
|
No |
1 |
|
1 |
|
|
Yes |
0.91 (0.64–1.30) |
0.616 |
1.07 (0.75–1.54) |
0.700 |
|
Cancer patients should think less of themselves due to their condition |
||||
|
No |
1 |
|
1 |
|
|
Yes |
0.64 (0.44–0.93) |
0.020 |
0.73 (0.49–1.07) |
0.105 |
|
Cancer patients should be ashamed of themselves due to their condition |
||||
|
No |
1 |
|
1 |
|
|
Yes |
1.53 (0.97–2.44) |
0.069 |
1.58(0.97–2.57) |
0.065 |
|
Ashamed of yourself if diagnosed with Cancer |
||||
|
No |
1 |
|
|
|
|
Yes |
0.88 (0.63–1.21) |
0.421 |
|
|
|
Cancer disease is very serious |
||||
|
No |
1 |
0.314 |
|
|
|
Yes |
2.52 (0.42–15.27) |
|
|
|
Comparison of referrals between HCPs and THs
Healthcare providers who think cancer patients face administrative discrimination are 1.53 times more likely to refer patients compared to THs who are 0.87 times less likely to refer cancer patients (aRR:1.53;95% CI:1.25–1.87 vs aRR:0.87;95% CI:0.64–1.18, respectively). Similarly, HCPs who thought that a patient is responsible for their own disease/fate were 1.26 times more likely to refer patients compared to THs who were 0.45 times less likely to refer (aRR:1.26;95% CI:1.00–1.60 vs aRR: 0.45;95% CI:0.33–0.62) (Tables 4 and 5).
Finally, HCPs and THs perceived various barriers to early detection of breast cancer for patients, illuminating the individual, interpersonal and socio-cultural and health system challenges (Supplementary File). Participants largely endorsed all barriers, ranging from individual: ‘Women do not recognize the signs of breast abnormalities’ n=483, (91.5%), to interpersonal ‘Resistance from a male partner about being checked by a doctor’ n=249, (47.2%), and ‘belief that breast cancer detection equals death’ n=482, (91.3%), to health systems: ‘lack of training among medical personnel to detect breast abnormalities’ n=360, (68.2%).
As for barriers to treatment, n=499 (94.5%) of respondents perceived that lack of money to pay for medicines posed significant challenges, while n=492 (93.2%) agreed that fear of treatment side effects was an obstacle. Additionally, fear of rejection from the husband or partner further complicated the situation, with many participants reporting fear of seeking medical help due to societal perceptions n =411, (77.8%) (Supplementary File).
Discussion
Breast cancer presents a significant and growing public health challenge in Tanzania, primarily due to many patients presenting at advanced stages, which in turn leads to high mortality rates. This study investigated the relationship between HCPs’ and THs’ knowledge and attitudes of breast cancer, and their treatment and referral practices. As to our best knowledge this is the first study in Tanzania of associations with referral of breast cancer patients for detection, diagnosis and treatment by HCPs and THs [1–3].
Our findings indicate significant differences between HCPs and THs in their knowledge of the risk factors of breast cancer explored in this study. Traditional healers demonstrated insufficient knowledge of critical risk factors for breast cancer such as advancing age, heredity, and stress, with some risk factors being known by fewer than one in six THs. This indicates a significant knowledge gap among THs. However, a Western biomedical model is not the only lens to view cancer care. So, it’s possible that they do not know some of the basic facts about breast cancer risk, but it’s also possible that they have been told those things and simply don’t believe them because they believe in other causes, which aligns with existing literature from Ethiopia and Congo [24,25]. Studies have revealed that identifying knowledge gaps and addressing these gaps can be effective in improving quality of care provided by THs [26].
Additionally, our results highlight that HCPs’ and THs’ attitudes towards patients with breast cancer correlated with their referral practices, but in opposite directions. For HCPs, endorsement of several negative or stigmatizing attitudes toward people with cancer was associated with increased likelihood of referral for treatment. Among THs, those who believed that cancer patients are socially marginalized, avoided by their friends, or are responsible for their fate were less likely to refer breast cancer patients for additional support. These findings reflect that HCP due to clinical norms and recognition of illness severity referred more. While THs refer less when they hold stigmatizing belief, which takes away empathy, confidence or perceived benefit of seeking medical care. The findings on practitioner attitudes resonate with previous studies conducted in Ethiopia and Palestine, outlining the role of both healthcare and traditional practitioners’ attitudes and biases on the quality of care provided and likelihood to practice [27,28]. Similarly, misinformation and knowledge gaps may perpetuate existing biases towards patients with breast cancer, thereby impacting patient outcomes [27].
On the other hand, the results highlight the relatively higher knowledge and more positive attitudes that HCPs hold towards breast cancer patients, which have potential implications for referral practices, including early detection, diagnosis and treatment. The existence of robust training programs for HCPs with up-to-date empirical data likely empowers HCPs to score higher in these areas. Their THs counterparts may rely more on spiritual beliefs, anecdotal experience and knowledge, thereby demonstrating much different levels of knowledge and attitudes [27,29].
Overall, our findings add context to our qualitative study which shows that lack of adequate breast cancer knowledge and awareness is a very common reason for advanced disease presentation among HCPs and THs [23]. Both studies point to the need for enhancement of their knowledge and awareness to help recognize the signs and symptoms of breast cancer to reduce delays in diagnosis and treatment [30]. Therefore, provide insights that can inform clinical practice, targeted education and training programs, and strengthen referral pathways, and encourage policy initiatives, fostering a more integrated approach to cancer care in the Tanzanian context.
Implications for clinical practice and training
regarding early warning signs and impact on referral practices. This gap calls for the training of THs on knowledge of breast cancer, empowering them to initiate timely referrals of breast cancer patients to specialized care facilities, to correct misinformation, and to minimize biases towards patients [31]. Similar tailored interventions have been utilized and demonstrated positive impact for health issues including sexually transmitted infections and HIV [8,32].
The low levels of knowledge among THs emphasize the potential risks associated with delayed diagnosis due to prolonged reliance on traditional medicine. Since THs are often the first point of contact for many patients, integrating structured education programs and referral protocols into their practice could significantly minimize the know-do gap and improve early detection rates [31].
Collaboration between HCPs and THs should be fostered through workshops, mentorship programs, and awareness campaigns to enhance timely referrals and optimize patient outcomes [16]. This would further serve to strengthen existing referral pathways between various levels of healthcare facilities, but also between THs and HCPs.
To address the stigma associated with breast cancer and biases by practitioners, continued professional development and public health sensitization campaigns will be crucial in changing the negative perceptions and promoting patient-centered care [16,33].
Implications for policymakers
Policymakers should prioritize the development of comprehensive regulations; perspectives from service users, HCPs, THs, and administrators are essential. This will ensure that providers on all levels, but particularly in primary care, receive appropriate guidance on treatment and referral procedures [34,35].
Similarly, regulatory frameworks should be enhanced to acknowledge the role of THs and formalize collaborations between traditional and conventional healthcare providers [36]. Policies should encourage dialogue and partnerships [37].
Additionally, efforts should be made to address systemic barriers such as limited access to diagnostic facilities and financial constraints faced by patients. Policymakers should work towards improving healthcare infrastructure, particularly in rural areas, by increasing the availability of screening and mammography services and on-the-job training for HCPs in primary care. Awareness campaigns led by government agencies, in collaboration with community leaders and local media, could further enhance public knowledge and encourage early health-seeking behaviors [38].
Implications on research
Further qualitative research is needed to explore the cultural and societal factors influencing THs’ knowledge of and attitudes toward breast cancer. Understanding their perspectives in greater depth can help in designing culturally sensitive interventions that encourage safer practices and stronger collaboration between THs and HCPs [39].
Moreover, longitudinal studies could assess the effectiveness of educational interventions targeting HCPs and THs, evaluating how knowledge gains translate into improved referral rates and earlier diagnoses. Investigating patient experiences and barriers to accessing care will also provide valuable insights into how health policies and service delivery can be optimized [40]. A similar approach has been followed in HIV and mental health settings, resulting in such guidance [41].
Finally, expanding research into the role of community engagement in addressing stigma and misinformation about breast cancer is essential. Future studies should examine the impact of community health workers, peer education programs, and digital health solutions in promoting breast cancer awareness and early detection in both urban and rural settings [42–44].
Limitations of the study
One limitation of our study is that this study was conducted at one region, which may not be representative of the other regions in Tanzania. Despite this limitation, this is the first study to be conducted in Tanzania to assess the knowledge, attitudes, and practices regarding breast cancer treatment among HCPs and THs. This study provides important insights on the current knowledge and attitude of referral practices among HCPs and THS which emphasizes the need for targeted education and training programs, and strengthen referral pathways for the breast cancer patients.
Conclusion
This study underscores the urgent need for targeted interventions to address gaps in knowledge, attitudes, and practices regarding breast cancer among HCPs and THs in Tanzania. Strengthening clinical training, developing supportive policies, sensitizing the public to reliable information, and fostering research on cultural and systemic barriers will be critical in improving early detection, timely referrals, and overall patient outcomes. A collaborative approach that integrates traditional and biomedical health practices can pave the way for a more effective and inclusive cancer care system in Tanzania.
Statements & Declarations
Funding
This work was supported by The University of Alabama (UAB), Kilimanjaro Clinical Research Institute (KCRI), NORA Consortium, funded by the German Federal Ministry of Research, Technology and Space 01KA2220 and REACCT-CAN funded by Science for Africa Foundation to the Developing Excellence in Leadership, Training and Science in Africa (DELTAS Africa) program [Del-22-008] with support from Wellcome Trust and the UK Foreign, Commonwealth & Development Office and is part of the EDCPT2 programme supported by the supported by the European Union (Grant number [81295996]) and Global Health Working Group, Martin-Luther-University Halle-Wittenberg. The authors are responsible for the study.
Competing interest
The authors have no relevant financial or non-financial interests to disclose.
Author contributions
The authors made substantial contributions to the manuscript in the following ways: Authors contributed to the study conception and design of the study (E.F.M., L.G & B.T.M.). Material preparation, (E.F.M., L.G. & B.T.M). Data collection (V.K., C.T., F.M & G.M). Analysis was performed by (E.F.M., M.M., L.M and Y.G.). Methodology (E.F.M.). Writing original draft (E.F.M.). Writing, review and editing (B.T.M., K.M., F.B., M.M., G.M., B.M., C.B., B.K., M.J., E.K., B.M., A.P., E.K., G.M., & E.F.M.) Funding acquisition: (B.T.M. & E.F.M.). Resources: (B.T.M., G.M and E.F.M.). Supervision: (B.T.M) All authors read and approved the final manuscript.
Data availability
The datasets generated during and/or analyzed in the current study are not publicly available due to ethical constraints that prevent the public sharing of this data. Open data sharing was not included in the participants' informed consent or the approved ethical protocol for the study.
Additionally, there are confidentiality concerns regarding detailed quantitative data. But are available from the corresponding author on reasonable request.
Ethics approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Local Ethics Committee of KCMC University ethical review board (ref: 2425/Prop No. 1179, 2024), the National Review Board (ref: NIMR/HQ/R.8a/Vol./IX/3773, 2024) and the President’s Office, Regional Administration and Local Government of Tanzania (PO-RALG-ref: AB.307/223/01 dated 27 November 2024).
Consent to participate
Informed consent was obtained from all individual participants included in this study. Their right to withdraw at any time, and assurances of anonymity and data confidentiality were considered. No identifiable participant information was included in the manuscript.
Consent to publish
The authors affirm that human research participants provided informed consent regarding publishing their data.
Acknowledgments
We extend our gratitude to all study participants, heads of respective hospitals, departments, units, health centers, villages and streets in communities where data collection took place for their willingness to take part and provide valuable information that facilitated data collection, as well as to the colleagues, gatekeepers, for their support during this process. Special thanks to Prof. Lily Gutnik for her great support in this work. Also, thanks to Dr. Furaha Serventi, Dr. Oliver Henke, the Oncologists for their expert contributions to the survey tool and Faith Mmary (social worker) from the Oncology unit, for data collection assistance. Kilimanjaro Christian Medical Centre, Kilimanjaro Clinical Research Institute (KCRI) and KCMC University for supporting EM.
References
2. Komen S. Full_Tanzania_Assessment_report.pdf [Internet]. 2017 [cited 2024 Dec 28]. Available from: https://www.komen.org/wp-content/uploads/Full_Tanzania_Assessment_report.pdf.
3. Ferlay J, Colombet M, Soerjomataram I, Parkin DM, Piñeros M, Znaor A, et al. Cancer statistics for the year 2020: An overview. Int J Cancer. 2021 Apr 5.
4. WHO. Cancer - Screening and early detection [Internet]. Geneva: WHO; 2024 [cited 2024 May 29]. Available from: https://www.who.int/europe/news-room/fact-sheets/item/cancer-screening-and-early-detection-of-cancer.
5. Kantelhardt EJ, Cubasch H, Hanson C. Taking on breast cancer in East Africa: global challenges in breast cancer. Curr Opin Obstet Gynecol. 2015 Feb;27(1):108–14.
6. Sakafu LL, Philipo GS, Malichewe CV, Fundikira LS, Lwakatare FA, Van Loon K, et al. Delayed diagnostic evaluation of symptomatic breast cancer in sub-Saharan Africa: A qualitative study of Tanzanian women. PLoS One. 2022 Oct 6;17(10):e0275639.
7. Mekonnen AG, Gebeyehu BT, Woldearegay M. Experience of patients with breast cancer with traditional treatment and healers' understanding of causes and manifestations of breast cancer in North Shewa zone, Ethiopia: a phenomenological study. BMJ Open. 2022 Dec 1;12(12):e063726.
8. Sorsdahl K, Ipser JC, Stein DJ. Interventions for educating traditional healers about STD and HIV medicine. Cochrane Database Syst Rev. 2009 Oct 7;2009(4):CD007190.
9. Asuzu CC, Akin-Odanye EO, Asuzu MC, Holland J. A socio-cultural study of traditional healers role in African health care. Infect Agent Cancer. 2019 Jun 20;14:15.
10. Asiimwe JB, Nagendrappa PB, Atukunda EC, Kamatenesi MM, Nambozi G, Tolo CU, et al. Prevalence of the Use of Herbal Medicines among Patients with Cancer: A Systematic Review and Meta-Analysis. Evid Based Complement Alternat Med. 2021 May 17;2021:9963038.
11. Mwaka AD, Achan J, Adoch W, Wabinga H. From their own perspectives: a qualitative study exploring the perceptions of traditional health practitioners in northern Uganda regarding cancers, their causes and treatments. BMC Fam Pract. 2021 Jul 19;22(1):155.
12. Mujinja PG, Saronga HP. Traditional and Complementary Medicine in Tanzania: Regulation Awareness, Adherence and Challenges. Int J Health Policy Manag. 2022 Aug 1;11(8):1496–1504.
13. Stangeland T, Dhillion SS, Reksten H. Recognition and development of traditional medicine in Tanzania. J Ethnopharmacol. 2008 May 8;117(2):290–9.
14. Tanzania Census. Administrative Units, Population Distribution Report, Tanzania, Volume 1a [Internet]. 2022 [cited 2023 Dec 3]. Available from: https://www.nbs.go.tz/nbs/takwimu/Census2022/Administrative_units_Population_Distribution_Report_Tanzania_volume1a.pdf.
15. Christian L. Traditional Medicine in Tanzania: Bridging the Gap between Ancient Practices and Modern Healthcare [Internet]. Tanzania Digest. 2023 [cited 2025 Jul 9]. Available from: https://www.digest.tz/traditional-medicine-in-tanzania-bridging-the-gap-between-ancient-practices-and-modern-healthcare/.
16. Msoka EF, Dwarampudi S, Billings R, Stone RJ, Mwageni RE, Beavers A, et al. The role of traditional healers along the cancer care continuum in Sub-Saharan Africa: a scoping review. Arch Public Health. 2025 Feb 13;83(1):35.
17. Kayombo EJ. Traditional and alternative medicine in Tanzania: lesson from the exhibition. SAS J Med. 2017;3(1):23–31.
18. University of Bonn. Study in Tanzania shows a traditional diet causes less inflammation [Internet]. Medical Xpress; 2021 [cited 2025 Jul 9]. Available from: https://medicalxpress.com/news/2021-02-tanzania-traditional-diet-inflammation.html.
19. Gessler MC, Msuya DE, Nkunya MH, Schär A, Heinrich M, Tanner M. Traditional healers in Tanzania: sociocultural profile and three short portraits. J Ethnopharmacol. 1995 Nov 3;48(3):145–60.
20. Government of Tanzania. The Traditional and Alternative Medicine Act, 2002. Dar es Salaam: Government Printer; 2002.
21. Chao CA, Huang L, Visvanathan K, Mwakatobe K, Masalu N, Rositch AF. Understanding women's perspectives on breast cancer is essential for cancer control: knowledge, risk awareness, and care-seeking in Mwanza, Tanzania. BMC Public Health. 2020 Jun 15;20(1):930.
22. Makurirofa L, Mangwiro P, James V, Milanzi A, Mavu J, Nyamuranga M, et al. Women's knowledge, attitudes and practices (KAP) relating to breast and cervical cancers in rural Zimbabwe: a cross sectional study in Mudzi District, Mashonaland East Province. BMC Public Health. 2019 Jan 24;19(1):109.
23. Msoka EF, Gutnik L, Cyril AM, Kitali BC, Saria VF, Kwayu JC, et al. Abstract 77: Health Care Providers and Traditional Healers Perspectives on Late Diagnosis of Breast Cancer in Tanzania: A Qualitative Study. Cancer Epidemiology, Biomarkers & Preventio. 2021 Jul 1;30(7_Supplement):77.
24. Workie Limenh L, Emagn Kasahun A, Ayalew Tessema T, Kerie Anagaw Y, Simegn W, Ayenew W. Assessment of traditional healers’ knowledge and utilization of pharmaceutical equipment and medical supplies in the Amhara region, North West Ethiopia. Pharm Biol. 2024 Dec;62(1):261–8.
25. Kyambikwa Bisangamo C, El-Nimr NA, Milabyo Kyamusugulwa P, Wahdan IMH, Gad ZM. Traditional healers' knowledge and infection control practices related to HIV in Bukavu City, Democratic Republic of the Congo. BMC Public Health. 2024 May 27;24(1):1403.
26. Moeta M, Musie MR, Seretlo RJ, Ledimo M, Rasweswe MM, Makhavhu E, et al. Traditional health practitioners’ training needs on biomedical knowledge and skills in a South African township. Afr J Prim Health Care Fam Med. 2023 Nov 1;15(1):e1–9.
27. Gietaneh W, Simieneh MM, Endalew B, Tarekegn S, Petrucka P, Eyayu D. Traditional healers’ roles, and the challenges they face in the prevention and control of local disease outbreaks and pandemics: the case of the East Gojjam Zone in northwestern Ethiopia. Frontiers in Tropical Diseases. 2023 Feb 3;4:978528.
28. Shakhshir M, Alkaiyat A. Healthcare providers' knowledge, attitude, and practice on quality of nutrition care in hospitals from a developing country: a multicenter experience. J Health Popul Nutr. 2023 Mar 7;42(1):15.
29. Berhe KT, Gesesew HA, Ward PR. Traditional healing practices, factors influencing to access the practices and its complementary effect on mental health in sub-Saharan Africa: a systematic review. BMJ Open. 2024 Sep 25;14(9):e083004.
30. Msoka EF, Abraham M, Mulder BC, Beavers A, Gebremariam A, Bright FB, et al. The Perspectives of Healthcare Providers, Traditional Healers, and Other Key Informants on the Late Diagnosis of Breast Cancer in Northern Tanzania: A Qualitative Study. Sciety. 2024. Available from: https://sciety.org/articles/activity/10.21203/rs.3.rs-5313282/v1.
31. Madamombe I. Traditional healers boost primary health care. Africa renewal. 2006 Jan 31;19(4):10–11.
32. Audet CM, Salato J, Blevins M, Amsalem D, Vermund SH, Gaspar F. Educational intervention increased referrals to allopathic care by traditional healers in three high HIV-prevalence rural districts in Mozambique. PLoS One. 2013 Aug 1;8(8):e70326.
33. Solera-Deuchar L, Mussa MI, Ali SA, Haji HJ, McGovern P. Establishing views of traditional healers and biomedical practitioners on collaboration in mental health care in Zanzibar: a qualitative pilot study. Int J Ment Health Syst. 2020 Jan 9;14:1.
34. Frenk J. Dimensions of health system reform. Health Policy. 1994 Jan 31;27(1):19–34.
35. WHO. Linkages. Geneva: World Health Organization; 2018. Available at: https://www.who.int/docs/default-source/primary-health-care-conference/linkages.pdf.
36. Matungwa DJ, Hong R, Kidola J, Pungu D, Ponticiello M, Peck R, et al. Understanding the role of traditional healers in the HIV care cascade: Findings from a qualitative study among stakeholders in Mwanza, Tanzania. PLOS Glob Public Health. 2022 Aug 15;2(8):e0000674.
37. Akhnif EH, Hachri H, Belmadani A, Mataria A, Bigdeli M. Policy dialogue and participation: a new way of crafting a national health financing strategy in Morocco. Health Res Policy Syst. 2020 Sep 29;18(1):114.
38. Mujinja GM, Kida TM. IMPLICATIONS OF HEALTH SECTOR REFORMS IN TANZANIA: POLICIES, INDICATORS AND ACCESSIBILITY TO HEALTH SERVICES. THDR 2014: Background Paper No. 8. ESRF Discussion Paper 62. Available at: https://esrf.or.tz/wp-content/uploads/2021/01/THDR-BP-8.pdf.
39. Schausberger B, Mmema N, Dlamini V, Dube L, Aung A, Kerschberger B, et al. "We have to learn to cooperate with each other": a qualitative study to explore integration of traditional healers into the provision of HIV self-testing and tuberculosis screening in Eswatini. BMC Health Serv Res. 2021 Dec 6;21(1):1314.
40. Madundo K, Perry M, Mwobobia J, Shekibula I, Msoka EF, Tarimo CS, et al. Patient experiences and contextual appropriateness of universal screening for depression and suicide risk in HIV care: a qualitative study in Tanzania. Front Health Serv. 2025 Apr 24;5:1557348.
41. Madundo K, Mwobobia JM, Perry M, Knippler E, Amiri I, Msoka EF, et al. HIV and mental health provider experiences of implementing brief depression and suicide screening among people living with HIV in Tanzania: a qualitative study. PLOS Mental Health. 2025 Mar 13;2(3):e0000268.
42. World Health Organization. Regional Office for the Eastern Mediterranean. Community health workers: a strategy to ensure access to primary health care services. Geneva: World Health Organization; 2016. Available at: https://iris.who.int/handle/10665/249563.
43. Hartzler AL, Tuzzio L, Hsu C, Wagner EH. Roles and Functions of Community Health Workers in Primary Care. Ann Fam Med. 2018 May;16(3):240–5.
44. Vasanthan L, Natarajan SK, Babu A, Kamath MS, Kamalakannan S. Digital health interventions for improving access to primary care in India: A scoping review. PLOS Glob Public Health. 2024 May 14;4(5):e0002645.