Abstract
Purpose: To present a challenging case of tubercular uveitis in an asymptomatic patient, featuring unilateral occlusive vasculitis with a frosted branch angiitis phenotype and bilateral serpiginous-like choroiditis.
Methods: Case report with clinical photography.
Results: Routine fundus examination of an asymptomatic 26-year-old Pakistani man revealed a retinal vasculitis with frosted branch angiitis phenotype in the right eye and bilateral serpiginous-like choroiditis. A positive QuantiFERON-TB Gold assay, tuberculin skin test and a chest computed tomography resulted in the diagnosis of presumed tuberculous origin of the posterior uveitis. Four-drug anti-tubercular therapy combined with systemic corticosteroids were initiated. A paradoxical immune-mediated worsening followed, requiring an increase of systemic corticosteroid therapy. An accompanying vitreous hemorrhage was initially managed with intravitreal bevacizumab. However, persistent vitreous opacities and limited visual improvement necessitated a phacovitrectomy with intravitreal triamcinolone acetonide. Two weeks postoperatively mild visual improvement was observed, although inflammatory activity and occlusive vasculitis persisted. Administration of an additional dexamethasone intravitreal implant resulted in complete resolution of intraocular inflammation. The final BCVA of the right eye improved to 20/25 in the following months and remained stable two years after the initial presentation.
Conclusions: This case illustrates the therapeutic complexity of tubercular uveitis with phacovitrectomy and intravitreal dexamethasone implant proving effective in achieving disease control of paradoxical worsening.
Keywords
Dexamethasone intravitreal implant, Frosted branch angiitis, Occlusive vasculitis, Paradoxical immune-mediated worsening, Serpiginous-like choroiditis, Tuberculosis, Vitrectomy
Introduction
Intraocular tuberculosis can present with a broad spectrum of clinical manifestations, ranging from anterior to posterior uveitis, often associated with tubercular granulomas, serpiginous-like choroiditis and sometimes even endophthalmitis. Diagnosis remains challenging, particularly in the absence of systemic symptoms. Supportive diagnostic tools include tuberculin skin test, interferon-gamma release assays such as QuantiFERON-TB or T-SPOT TB, and radiologic evidence of active or healed pulmonary lesions on chest radiography or computed tomography. Management of intraocular tuberculosis is equally complex due to its variable presentation, which may involve both direct mycobacterial infection as well as immune-mediated inflammatory responses [1,2].
We report a diagnostically challenging case of a patient without symptoms, presenting with presumed tuberculous occlusive vasculitis characterized by a frosted branch angiitis-like appearance and serpiginous-like choroiditis.
Case Presentation
A 26-year-old Pakistani man presented for a routine ophthalmologic examination required for certification to obtain a taxi driver’s license. The patient reported no visual complaints and denied any previous ophthalmologic history. His general medical history was unremarkable, aside from seasonal allergic rhinitis for which he used an oral antihistamine. On examination, best corrected visual acuity (BCVA) was 20/60 in the right eye and 20/17 in the left eye. Anterior segment examination was normal in both eyes. Fundus examination of the right eye revealed widespread retinal vasculitis involving 360° of the peripheral retina, with multiple retinal hemorrhages, cotton wool spots, optic disc edema, and an inferior frosted branch angiitis-like appearance (Figure 1A). Additionally, the superotemporal macular region demonstrated retinal atrophy with pigmentary changes in a serpiginous pattern. In the left eye, more extensive areas of serpiginous-like chorioretinal atrophy were observed in the macular and mid-peripheral regions, with sparing of the fovea (Figure 1B). Optical coherence tomography revealed intraretinal edema in the central macular area in the right eye (Figure 2A), while the left eye showed no signs of edema. Fluorescein angiography of the right eye confirmed periphlebitis and active vasculitis (Figure 2B). In contrast, no vasculitis or disc edema was observed in the left eye (Figure 2C). The chorioretinal lesions in both eyes appeared clinically inactive. A comprehensive uveitis workup revealed a positive QuantiFERON-TB Gold assay and a strongly positive tuberculin skin test (20 x 20 mm induration) in a patient with no history of Bacillus Calmette-Guérin vaccine. Hematologic and serologic investigations were within normal limits or negative, including complete blood count, syphilis serology, HIV, toxoplasma serology, HLA-B51, antinuclear antibody, antineutrophil cytoplasmic antibodies, angiotensin-converting enzyme and C-reactive protein. Cytomegalovirus and varicella-zoster virus serologies were IgM negative and IgG positive. Erythrocyte sedimentation rate and serum lysozyme were mildly elevated (34 mm/hr and 19.2 mcg/mL, respectively). Chest computed tomography revealed extensive mediastinal lymphadenopathy with partial central necrosis and no calcification, without evidence of pulmonary parenchymal involvement. Diagnosis of presumed tuberculous retinal vasculitis with frosted branch angiitis phenotype in the right eye and bilateral serpiginous-like choroiditis was made. While awaiting confirmatory results, topical prednisolone acetate eye drops three times daily in the right eye were initiated. Following the establishment of the presumptive diagnosis, a standard four-drug anti-tubercular therapy (ATT) regimen was started by the pulmonologist, consisting of isoniazid (300 mg once daily) and rifampicin (600 mg once daily) for a total duration of 6 months, in combination with pyrazinamide (1500 mg once daily) and ethambutol (1600 mg once daily) during the initial 2 month intensive phase of treatment. One week later, systemic corticosteroid therapy was introduced with oral prednisolone 60 mg daily in a tapering schedule. One month into treatment, the patient presented to the emergency department with acute vision loss in the right eye, reduced to hand motion. Ophthalmic examination revealed dense premacular vitreous opacities, progression of retinal hemorrhages, and frosted branch angiitis in the peripheral retina (Figure 1C). B-scan ultrasonography confirmed dense vitreous debris at the posterior pole with an attached retina. Aqueous humor polymerase chain reaction (PCR) testing for herpes simplex virus, varicella-zoster virus, cytomegalovirus and Toxoplasma gondii was negative. The clinical picture was consistent with a paradoxical immune-mediated worsening following the initiation of ATT. Systemic corticosteroids were increased again to prednisolone 60 mg daily, resulting in mild clinical improvement over the subsequent two weeks. However, this was followed by the development of a vitreous hemorrhage in the right eye. Intravitreal bevacizumab was administered. Due to persistent vitreous opacities and lack of visual improvement after two weeks, a 27-gauge pars plana phacovitrectomy was performed with intravitreal injection of triamcinolone acetonide (4,0%). Cataract extraction was indicated due to numerous inflammatory and red blood cells in the anterior vitreous adherent to the posterior lens capsule, as well as the expected early cataract formation following intraocular corticosteroid therapy. Intraoperative findings included extensive retinitis, multiple intraretinal hemorrhages, and vitritis. Vitreous samples were PCR-negative for Mycobacterium tuberculosis. Two weeks after surgery, there was mild visual improvement, although the inflammatory activity and occlusive vasculitis persisted. A dexamethasone intravitreal implant was administered, leading to a significant reduction in inflammation (Figures 1D, 2D, and 2E). The BCVA of the right eye improved to 20/25 in the following months and remained stable two years after the initial presentation, with no further medication required at the two-year follow-up.
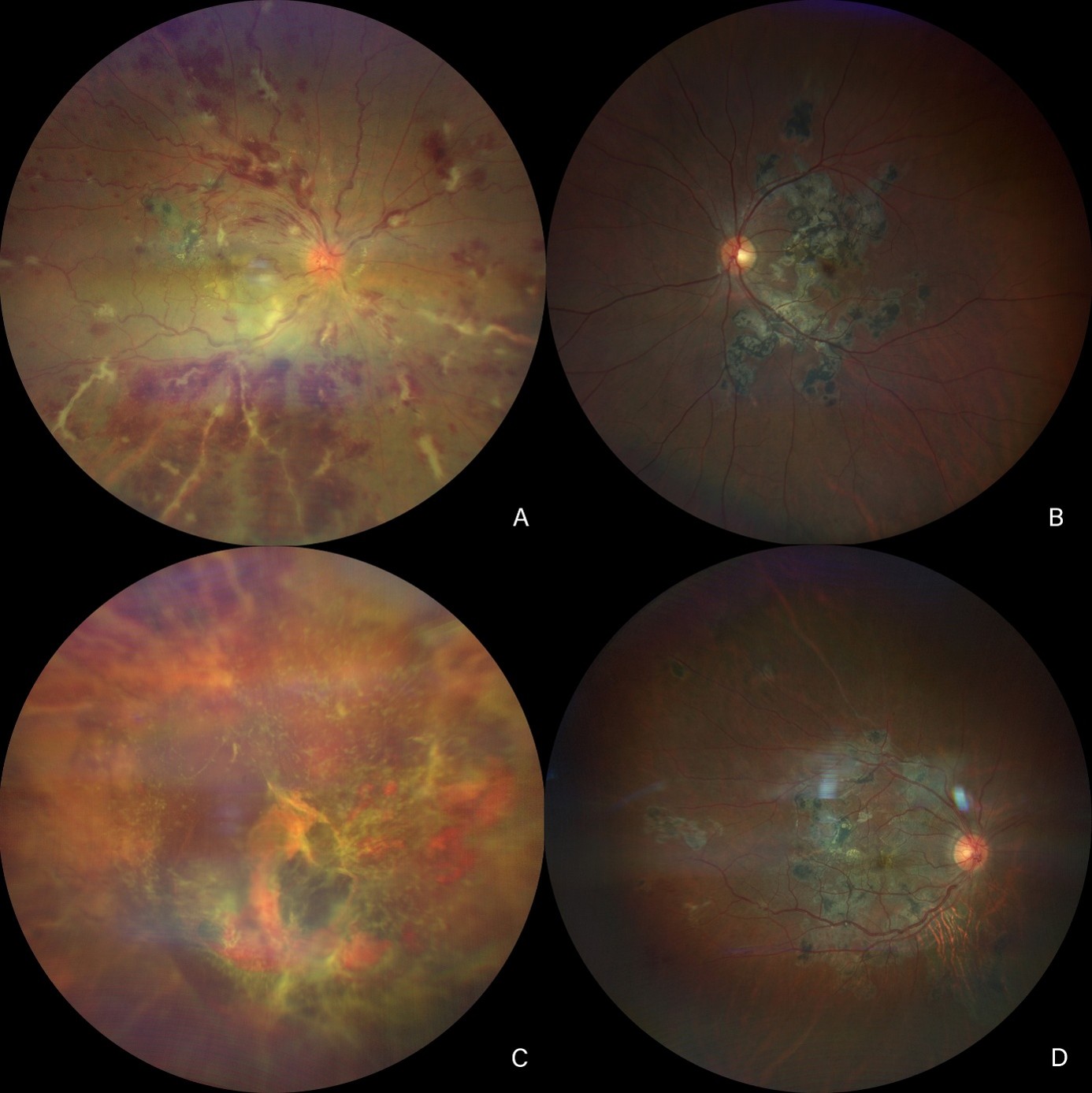
Figure 1. Colour fundus photography of the right eye (A) and left eye (B) at presentation. (C)
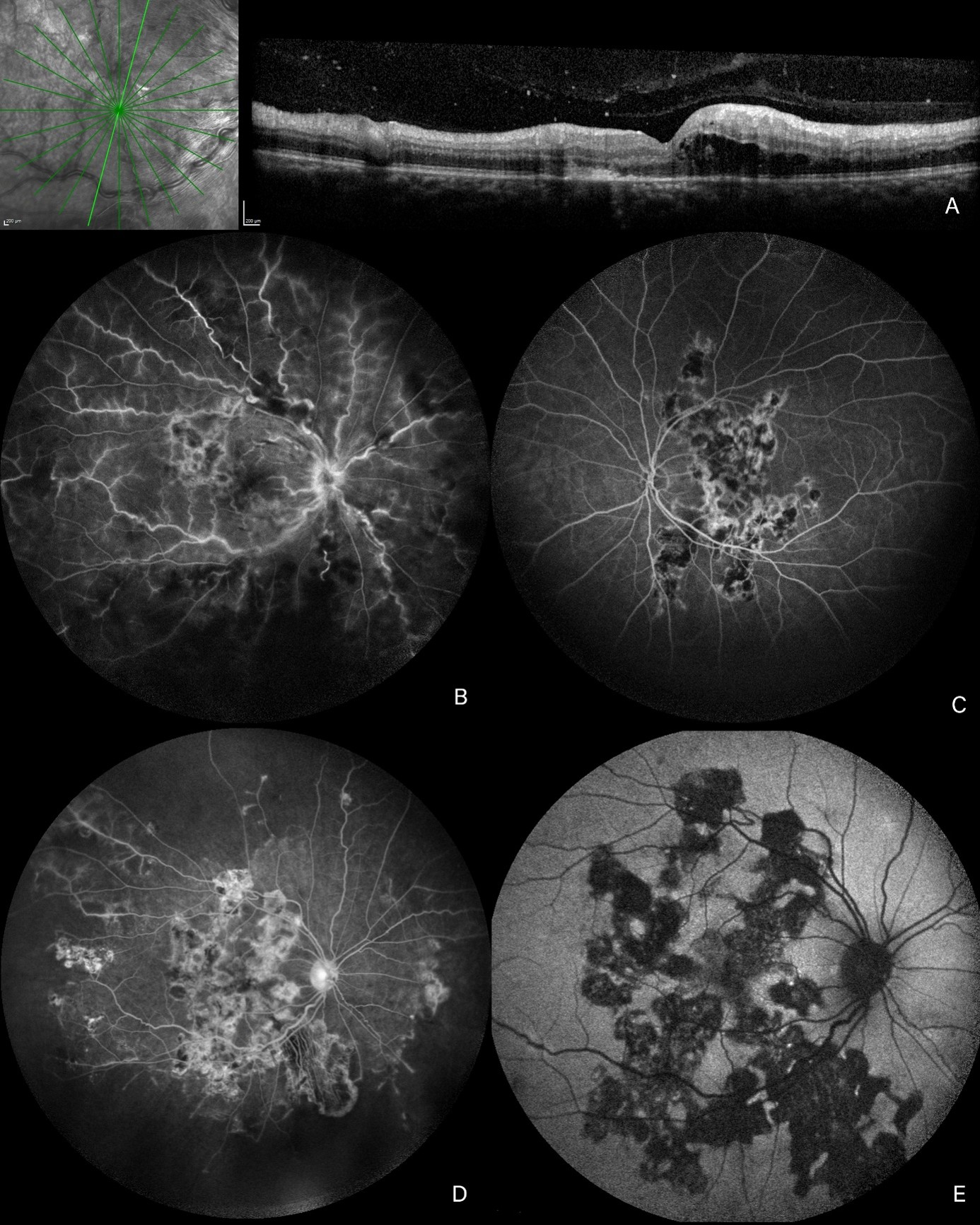
Figure 2. Optical coherence tomography of the right eye at presentation (A). Fluorescein angiography of the right eye
Discussion
Ocular tuberculosis may arise from a direct infection or from indirect, immune-mediated inflammation triggered by mycobacterial antigens. Retinal pigment epithelial (RPE) cells are thought to play a key role in this process. Beyond their well-known function in phagocytosing and clearing the shed outer segments of the photoreceptors, RPE cells can also act as phagocytes for mycobacterial bacilli. Importantly, Mycobacterium bacilli may persist within RPE cell phagosomes, potentially provoking a T-cell mediated hypersensitivity reaction. This immune response may underlie the development of tubercular retinal vasculitis (TRV) and tubercular serpiginous-like choroiditis (TB-SLC) [1,3,4]. In our patient, we observed a mixed clinical picture of presumed tubercular uveitis with an asymmetrical course. In the right eye there was occlusive vasculitis with a frosted branch angiitis-like appearance, along with tubercular serpiginous-like choroiditis (TB SLC) that initially appeared inactive. In the left eye there was TB SLC that remained inactive throughout the entire follow-up period. TB SLC is a common manifestation of tubercular uveitis. Mycobacterium bacilli are aerobic organisms and so preferentially localize to the choroid, which has an abundant oxygen supply. TB SLC involves not only choroid and choriocapillaris but also RPE. The choroidal lesions typically begin in the posterior pole as yellowish-white placoid lesions with slightly elevated margins and progress centrifugally. Older lesions exhibit central pigment clumping and atrophy of both the underlying choroid and the overlying retina. These lesions are usually multifocal. In most patients, the fovea is initially spared [1,4,5]. In our patient’s right eye, the retinal vasculitis manifested as fulminant hemorrhagic vasculitis extending 360°, with extensive retinal hemorrhages, periphlebitis with widespread perivascular exudates, and both disc and macular edema. The more aggressive vasculitis in the right eye may reflect the inherently asymmetric nature of ocular tuberculosis. Focal hematogenous seeding of mycobacterial antigens could have resulted in a higher local antigenic load, thereby driving a stronger T-cell–mediated hypersensitivity response in the right eye. The perivascular exudates in the right eye resembled frosted branch angiitis, initially most prominent inferiorly and extending superiorly after four weeks.
Frosted branch angiitis is a rare form of vasculitis characterized by perivascular immune complex deposition along the retinal venules in the midperiphery, giving the appearance of frosted tree branches. Although it can be idiopathic, it has also been described secondary to viral infections such as herpes simplex and cytomegalovirus, as well as to tuberculosis [6,7]. Tubercular retinal vasculitis (TRV) commonly presents as retinal periphlebitis in otherwise healthy young adult men. It may be accompanied by choroiditis and vitritis. TRV is considered to have a dual etiology, involving both direct Mycobacterium tuberculosis infection and an immune-mediated component [8,9]. Despite the dramatic fundus appearance in the right eye, our patient was asymptomatic at initial presentation. This is typical in TB serpiginous-like choroiditis (TB SLC), as the fovea is often initially spared. As long as a small island of functioning fovea remains, patients may be unaware of symptoms despite extensive scarring and pigmentation [4]. Similarly, during the active phase of vasculitis, patients often remain asymptomatic until a vitreous hemorrhage occurs. According to the Collaborative Ocular Tuberculosis Study criteria, our patient met the definition for presumed tubercular uveitis. The fundus findings were suggestive of both TRV and TB SLC. He had positive Mantoux and QuantiFERON tests, as well as a chest CT consistent with tuberculosis. He also originated from an endemic region. Other causes of uveitis were excluded [2]. On this basis, four-drug ATT was initiated. As described by Shukla [8], corticosteroids are recommended in TRV when the uveitis is sight-threatening, particularly in cases of posterior, severe, hemorrhagic vasculitis with vitritis and macular edema—all of which were present in our patient. In addition, both TRV and TB SLC may have an autoimmune inflammatory component, and paradoxical worsening is not uncommon. A paradoxical reaction may occur after ATT due to the release of bacterial endotoxins upon lysis, which amplifies the immune response. This phenomenon is more likely when there is a high antigenic load, such as with larger TB SLC lesions [1,3,10]. Despite ATT and systemic corticosteroid treatment, our patient developed a severe paradoxical reaction. Because of further clinical deterioration and an obscured fundus view, a phacovitrectomy was performed. Kaza [11] has noted that vitrectomy can be safely performed in uveitis cases to help control vitreous inflammation by removing inflammatory cells and debris, thereby facilitating healing and improving visual outcomes. During vitrectomy, a vitreous sample for Mycobacterium tuberculosis testing can be obtained; in our case, the sample was negative, likely due to the paucibacillary nature of tubercular uveitis [1,8,11]. Phacovitrectomy and intravitreal triamcinolone acetonide (4.0%) did not suffice to control the uveitis. Because the active TRV and TB SLC were unilateral, systemic corticosteroids with their associated side effects could be avoided by using local therapy. The dexamethasone intravitreal implant is highly effective in controlling intraocular inflammation in both infectious and non-infectious uveitis [3,8]. Three weeks after the intravitreal dexamethasone implant was administered, disease progression ultimately halted and the uveitis quieted. Visual acuity improved to 20/25 owing to preservation of the central island of intact macular architecture at the fovea and remained stable at 20/25 two years after the initial presentation.
This report highlights the importance of the continuation and search for a good treatment to save as much vision as possible.
Conflicts of Interest
None.
Funding
None.
References
2. Agrawal R, Gunasekeran DV, Grant R, Agarwal A, Kon OM, Nguyen QD, Pavesio C, et al. Clinical Features and Outcomes of Patients With Tubercular Uveitis Treated With Antitubercular Therapy in the Collaborative Ocular Tuberculosis Study (COTS)-1. JAMA Ophthalmol. 2017 Dec 1;135(12):1318–27.
3. Agarwal A, Handa S, Aggarwal K, Sharma M, Singh R, Sharma A, et al. The Role of Dexamethasone Implant in the Management of Tubercular Uveitis. Ocul Immunol Inflamm. 2018;26(6):884–92.
4. Bansal R, Gupta A, Gupta V, Dogra MR, Sharma A, Bambery P. Tubercular serpiginous-like choroiditis presenting as multifocal serpiginoid choroiditis. Ophthalmology. 2012 Nov;119(11):2334–42.
5. Lyons LJ, Singh MK, Carvounis PE, El-Annan J. MULTIMODAL IMAGING OF AN INTRARETINAL TUBERCULAR GRANULOMATOUS NEURORETINITIS. Retin Cases Brief Rep. 2022 May 1;16(3):382–4.
6. Agarwal M, Biswas J. Unilateral frosted branch angiitis in a patient with abdominal tuberculosis. Retin Cases Brief Rep. 2008 Winter;2(1):39–40.
7. Gurnani B, Balamurugan S, Kanakath A, Kaur K, Gupta A, Chaudhary S. First clinical case series of frosted branch angiitis: A diagnostic algorithm is suggested. Clin Case Rep. 2023 Aug 25;11(9):e7778.
8. Shukla D, Kalliath J, Dhawan A. Tubercular Retinal Vasculitis: Diagnostic Dilemma and Management Strategies. Clin Ophthalmol. 2021 Dec 15;15:4681–8.
9. Putera I, La Distia Nora R, Rombach SM, van Hagen PM, Dik WA. Pathogenesis of tubercular retinal vasculitis: An ongoing quest. J Clin Tuberc Other Mycobact Dis. 2026 Jan 14;42:100583.
10. Basu S, Nayak S, Padhi TR, Das T. Progressive ocular inflammation following anti-tubercular therapy for presumed ocular tuberculosis in a high-endemic setting. Eye (Lond). 2013 May;27(5):657–62.
11. Kaza H, Modi R, Rana R, Panda KG, Barik MR, Ali MH, et al. Effect of Adjunctive Pars Plana Vitrectomy on Focal Posterior Segment Inflammation: A Case-Control Study in Tuberculosis-Associated Uveitis. Ophthalmol Retina. 2018 Nov;2(11):1163–9.