Abstract
Background: Superior Mesenteric Vein (SMV) syndrome is an extremely rare cause of duodenal obstruction, resulting from external compression of the third portion of the duodenum by the SMV against the aorta. Due to its rarity and clinical similarity to Superior Mesenteric Artery (SMA) Syndrome, SMV syndrome may be misdiagnosed.
Case presentation: We present a 41-year-old male with progressive postprandial epigastric pain, nausea, vomiting, and 20 kg weight loss over six months. Imaging revealed compression of the duodenum by the SMV, with a normal aortomesenteric angle and distance, confirming the diagnosis of SMV Syndrome. Despite initial conservative management, including dietary modifications, positional changes, and nutritional support, symptoms persisted. The patient underwent laparoscopic duodenojejunostomy, leading to significant symptom relief and weight gain.
Conclusion: This case, the third reported in the literature, emphasizes the importance of contrast-enhanced CT with venous phase imaging for accurate diagnosis. Given the similarities with SMA Syndrome, a stepwise treatment approach is recommended, with surgery reserved for refractory cases. Increased awareness and further research are needed to optimize the management of this rare condition.
Keywords
Superior Mesenteric Vein Syndrome, Duodenal Obstruction, Duodenojejunostomy
Introduction
Superior Mesenteric Artery (SMA) syndrome is a well-known cause of duodenal obstruction, impairing gastric emptying, resulting from compression of the third portion of the duodenum between the SMA and the aorta due to a decreased aortomesenteric angle and distance [1,2]. In contrast, Superior Mesenteric Vein (SMV) syndrome is an exceptionally rare entity, in which the SMV compresses the third portion of the duodenum against the aorta, leading to gastric stasis and mechanical obstruction [3,4].
While both conditions share similar clinical manifestations, including postprandial epigastric pain, nausea, vomiting, early satiety, and unintentional weight loss, their underlying pathophysiology is distinct. Accurate radiological evaluation is crucial for distinguishing SMV syndrome from other conditions, yet standard imaging protocols may not adequately assess venous structures. Since only two previous cases of SMV syndrome have been documented in the literature [3,4].
Due to the extreme rarity of SMV syndrome, there is no established consensus on its treatment. However, despite the differences in their etiology, both SMV syndrome and SMA syndrome result in narrowing and obstruction at the fourth portion of the duodenum, leading to nearly identical clinical presentations. Given these similarities, a treatment algorithm similar to that used for SMA syndrome could be applied to the management of SMV syndrome [3].
In the first stage, it is essential to confirm the diagnosis of SMV syndrome by ruling out other differential diagnoses, as in SMA syndrome and Median Arcuate Ligament Syndrome (MALS). During the diagnosis of SMV syndrome, it is essential to thoroughly evaluate all patient data, especially to distinguish it from SMA syndrome [2,4,5]. Once the diagnosis of SMV syndrome is established, a treatment approach similar to that used in SMA syndrome should be followed. As in the treatment of SMAS, conservative treatment is initially recommended for SMV syndrome also. If this approach is unsuccessful, surgical intervention is considered. Conservative treatment consisting of gastrointestinal decompression, correction of electrolyte abnormalities, and nutritional support using either total parenteral nutrition (TPN), nasojejunal feeding or oral supplementation [3,6]. More frequent, liquid-based meals, leaning forward or adopting a lateral decubitus position after eating, and performing abdominal massage ‘’the Hayes technique’’, which involves applying pressure below the umbilicus in a backward and upward direction, may also alleviate symptoms by improving the passage through the constricted duodenum [7,8].
Depending on the severity of the disease, if the patient is in poor general condition, hospitalization may be required to stabilize the patient's overall health. If supportive therapy fails to achieve adequate improvement, surgical intervention should be considered [2]. In the surgical treatment of SMV syndrome, laparoscopic duodenojejunostomy, which is the most performed procedure in the surgical management of SMA syndrome, has also been reported to be successfully performed [3].
With this case report, we aim to share the detailed diagnostic and treatment process of our SMV syndrome case, which is the third reported case in the literature.
Case Presentation
A 41-year-old male presented with a six-month history of progressive postprandial epigastric pain, nausea, and vomiting. His symptoms had worsened over time, leading to a significant weight loss of 20 kg during this period. He described the pain as epigastric, radiating to the back, and exacerbated by food intake, with temporary relief after vomiting. The patient has no history of chronic disease, malignancy or previous abdominal surgery. On physical examination, the patient's BMI was 17.1 (Weight: 52 kg, Height: 1.74 m). He appeared cachectic, with mild epigastric tenderness but no palpable masses or organomegaly.
Initial workup
Routine laboratory investigations, including complete blood count, liver and renal function tests, electrolyte levels, and inflammatory markers, were all within normal limits. Abdominal ultrasound showed gastric distension but no other abnormalities. Upper gastrointestinal endoscopy revealed marked dilation of the stomach and the first three portions of the duodenum, with an apparent narrowing at the transition between the third and fourth portions of duodenum due to external compression (Figure 1A). There was no evidence of ulceration, intrinsic obstruction, or malignancy. A contrast-enhanced abdominal computed tomography (CT) scan in appropriate phases revealed: The fourth part of the duodenum is compressed between the superior mesenteric vein and the aorta, causing significant narrowing at this point, which severely restricts passage (Figures 1B and 1C). The stomach and duodenum proximal to the obstructed segment are significantly dilated. Additionally, both the stomach and the proximal duodenum are excessively sagging downward (Figure B). No signs of any kind of tumor, vascular malformation, or intra-abdominal mass. The aortomesenteric angle 33°, and the aortomesenteric distance was 15 mm (Figure 1D), which indicates that this case does not correspond to SMA syndrome. Given the radiological findings and the clinical picture, a diagnosis of SMV syndrome was established.
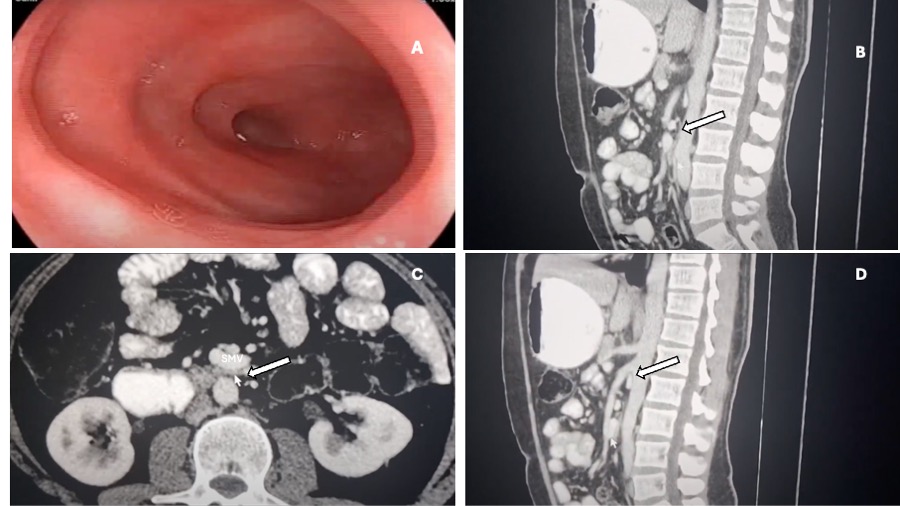
Figure 1. Endoscopic and abdominal computed tomography (CT) imaging A) Dilated second and third parts of the duodenum with narrowing observed towards the fourth part. B) Compression of the duodenum between the SMV and the aorta. C) Sagittal view showing the duodenum compressed between the SMV and the aorta. D) Image demonstrating a wide aortomesenteric angle and distance.
Treatment approach
After the patient was diagnosed with SMV syndrome, a conservative treatment approach was followed for approximately one month, including dietary adjustments, positional therapy, massage, electrolyte, and vitamin supplementation. However, due to the lack of improvement in the patient's condition, continued weight loss, and worsening symptoms over the past week, surgery was decided upon.
Surgical management
Informed consent for laparoscopic duodenojejunostomy was obtained from the patient. After a 10-hour fasting period, the patient was taken to surgery under general anesthesia. The patient was positioned on the operating table in a supine position with arms extended. A urinary catheter and nasogastric tube were placed. First, a 10 mm trocar was inserted into the abdomen through the umbilicus. The abdominal cavity was insufflated with carbon dioxide, and the camera was introduced. Under direct vision, a 12 mm trocar was inserted through the left inguinal region, a 5 mm trocar through the right inguinal region, and another 5 mm trocar at the level of the umbilicus, lateral to the rectus muscle (Figure 2A).
The omentum and transverse colon were retracted upward, while the small intestines were pulled downward. The peritoneum in this area was incised to access the duodenum. In SMAS patients, at this stage, the third part of the duodenum is usually clearly visible without opening the peritoneum. However, in this patient, the duodenum was not visible and was deeply located in the retroperitoneum. After incising the peritoneum, the retroperitoneal tissues were dissected to access the duodenum. The third and fourth parts of the duodenum were freed from the surrounding structures (Figure 2B). The duodenum was significantly dilated and had descended downward, extending behind the ileocolic vessels. A side-to-side anastomosis was performed between a jejunal loop located 50 cm distal to the Treitz ligament and the third part of the duodenum using a Tri-Stapler cartridge (CovidienR) (Figure 2C). The stapler opening was closed in two layers, and the staple line was reinforced with additional sutures (Figure 2D). After closing the mesenteric defect, a drain was placed next to the anastomosis, and the operation was completed. You can watch the full surgery video with all details from start to finish on the author’s YouTube channel. (https://youtu.be/742uVbmXIKs?si=wE0UOAgxWIAGq8oM )
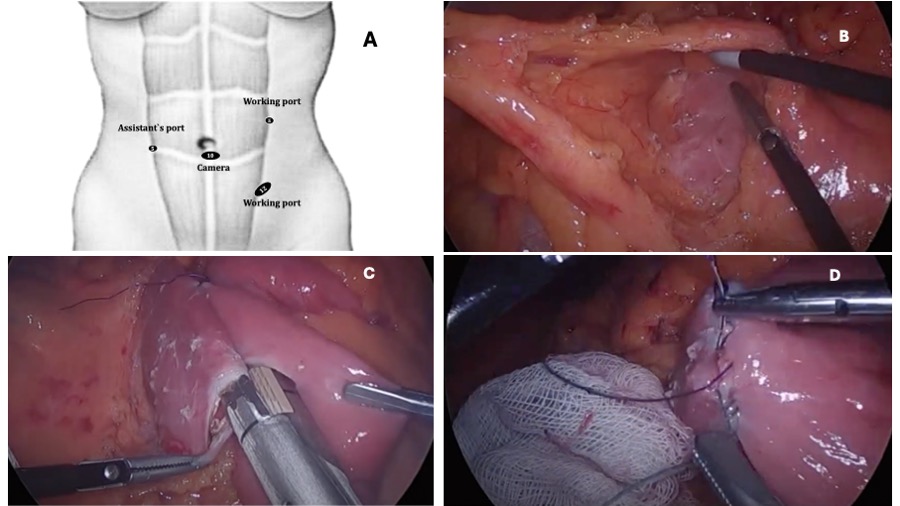
Figure 2. Laparoscopic duodenojejunostomy procedure steps in SMV syndrome. A) Trocar entry positions. B) Dissection and release of the third part of the duodenum, which is embedded in the retroperitoneum, by freeing the thickened peritoneum and surrounding fibrous tissue. C) Creation of a side-to-side anastomosis between the jejunum and the third part of the duodenum using a stapler. D) Closure of the stapler opening in two layers and reinforcement of the stapler line with additional sutures.
Postoperative course
The patient had an uneventful postoperative recovery. The patient was followed up on postoperative day 10, as well as at months 1, 6 and 12. It was observed that the patient had no complaints related to the surgery, preoperative symptoms had decreased by 90%, eating had become significantly easier, and the patient had regained approximately 11 kg during this period.
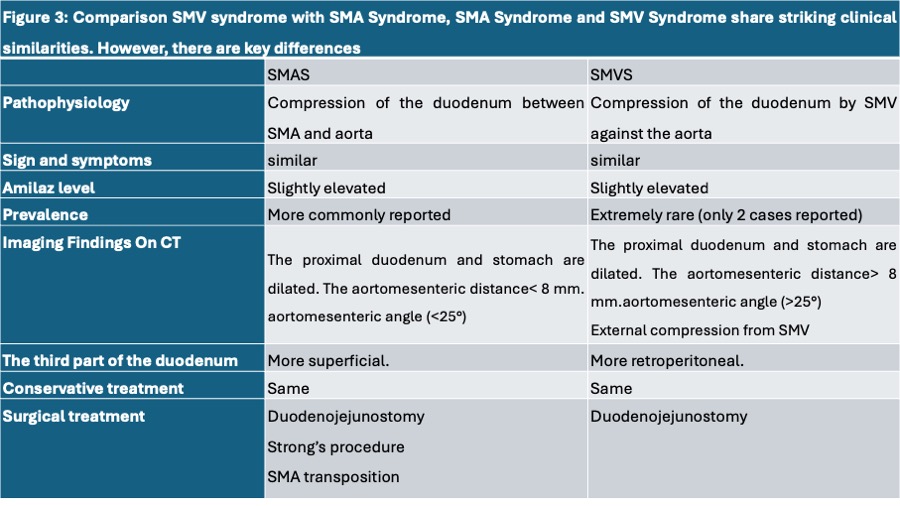
Figure 3. Comparison SMV syndrome with SMA syndrome.
Discussion
SMV syndrome is an extremely rare cause of duodenal obstruction, it may be misdiagnosed due to its similarity to SMA syndrome. While SMA syndrome occurs due to compression of the duodenum between the SMA and the aorta, SMV syndrome results from external compression by the SMV. In SMA syndrome, a reduced aortomesenteric angle (<25°) and/or aortomesenteric distance (<8 mm) is a key diagnostic finding [2], whereas in SMV syndrome, the aortomesenteric angle remains normal, but venous compression is evident. Routine imaging studies, particularly standard CT protocols, often focus on arterial structures, potentially overlooking venous compression. Therefore, contrast-enhanced CT with careful venous phase evaluation is essential to differentiate SMV syndrome from other causes of duodenal obstruction [3], If the patient has signs and symptoms of SMAS but the aortomesenteric angle and distance are not narrowed, the possibility of SMV syndrome should be considered, and an abdominal CT scan should be performed in the venous phase. SMA syndrome, Nutcracker syndrome, and MALS syndrome are conditions in which multiple compression syndromes may coexist in the same patient. In other words, the presence of one compression syndrome increases the likelihood of the occurrence of others. In such cases, treatment priorities and protocols become highly significant [8].
In SMV syndrome, as in SMA syndrome, conservative supportive therapy is initially provided. If this treatment is unsuccessful, the duodenojejunostomy is recommended [3,4]. Apart from this surgery, there is no available information on the use of surgical techniques such as release of the ligament of Treitz (Strong’s procedure), or SMV transposition, which are applied in SMAS treatment [2], for the treatment of SMV syndrome.
The successful outcome in this case reinforces the role of laparoscopic duodenojejunostomy as a definitive treatment for SMV syndrome. Given the extreme rarity of SMV syndrome, increased awareness among clinicians and radiologists is crucial for accurate diagnosis and timely intervention.
Although only two cases of SMV syndrome have been reported in the literature to date and the information on this condition remains insufficient, we would like to share our intraoperative observations, which differ from those in patients with SMA syndrome. In our case, the third portion of the duodenum was found to be much more deeply embedded within the retroperitoneum. In patients with SMA syndrome, the third part of the duodenum is typically clearly visible and dilated upon lifting the transverse colon. However, in our patient with SMV syndrome, the third part of the duodenum was not visible without performing dissection, as it was buried within the retroperitoneal space.
Conclusion
SMV syndrome is an extremely rare cause of duodenal obstruction. Accurate diagnosis requires contrast-enhanced CT with venous phase imaging. While conservative management is the first-line approach, laparoscopic duodenojejunostomy is an effective surgical option for refractory cases. This case, the third reported in the literature, highlights the need for increased clinical awareness and further research to establish standardized management guidelines.
References
2. Yetişir F, Çelik ME, Taşkın YE, Özdemir O, Kurt Ö, Tiken R, et al. Laparoscopic Duodenojejunostomy for the Treatment of Superior Mesenteric Artery Syndrome: Analysis of 91 Patients. Indian J Surg. 2025 Feb 14.
3. Ahmad KS, Alenazi NA, Essa MS, Alrushdan MS, Al-Shoaib AM. Laparoscopic Duodenojejunostomy for Superior Mesenteric Vein Syndrome Associated with Nutcracker Phenomenon: The First Case Report. Am J Case Rep. 2019 Jul 27;20:1108–13.
4. Dross PE, Molavi S, Chan A, Latshaw R, Chhabra P. Unusual etiologies for vascular duodenal compression mimicking the superior mesenteric artery (SMA) syndrome: the SMA-like syndrome. Journal of Gastrointestinal and Abdominal Radiology. 2019 Dec;2(02):140–6.
5. Yetisir F, Babayeva A, Güzel K. Laparoscopic surgical treatment of median arcuate ligament syndrome with the retrograde division technique: a case report. Annals of Clinical Gastroenterology and Hepatology. 2022 May 18;6(1):21–4.
6. Mathenge N, Osiro S, Rodriguez II, Salib C, Tubbs RS, Loukas M. Superior mesenteric artery syndrome and its associated gastrointestinal implications. Clin Anat. 2014 Nov;27(8):1244–52.
7. Baltazar U, Dunn J, Floresguerra C, Schmidt L, Browder W. Superior mesenteric artery syndrome: an uncommon cause of intestinal obstruction. South Med J. 2000 Jun;93(6):606–8.
8. Akopov AL, Artioukh DY. Good surgeon: A search for meaning. Turk J Surg. 2017 Jun 1;33(2):49–50.
9. Yetişir F, Tekindur Ş, Akın Y, Kurt Ö, Tiken R, Çelik ME. Simultaneous laparoscopic median arcuate ligament release and duodenojejunostomy for treatment of concurrent MALS and SMAS: a novel classification and surgical approach. Eur Surg. 2025 May 22;57:163–71.