Introduction
Obstructive hypertrophic cardiomyopathy (HCM) is a common inherited cardiac disease occurring in approximately 1 in 500 adults worldwide, characterized by left ventricular outflow tract (LVOT) obstruction, symptoms of heart failure, and increased risk of sudden cardiac death [1,2]. Conventional therapies; including beta-blockers, calcium channel blockers, and septal reduction, leave a significant proportion of patients symptomatic, necessitating investigation of novel management strategies [3].
Cardiac myosin inhibitors (CMIs) represent a novel mechanistic class targeting the underlying sarcomeric dysfunction in HCM. Recent phase 3 randomized controlled trials (RCTs) have demonstrated superiority over conventional therapy across functional, symptomatic, and hemodynamic endpoints[4–7]. While prior meta-analyses have evaluated CMI efficacy [8–10], we present an updated synthesis incorporating the most recent trial data, including the MAPLE-HCM trial (aficamten vs metoprolol, 2025), to provide a contemporary evidence base for clinical practice [11,12].
Methods
We conducted a systematic search of PubMed, Scopus, Embase, and Web of Science from inception through September 2025 using the terms: "hypertrophic cardiomyopathy" AND ("cardiac myosin inhibitor" OR "mavacamten" OR "aficamten") AND "randomized controlled trial". Searches were limited to English-language publications in adult human populations. PubMed returned 84 results, Scopus 117, Embase 96, and Web of Science 71 (total 368 records; 112 duplicates removed). After title/abstract screening (n = 256), 31 full texts were assessed for eligibility, yielding 7 RCTs meeting inclusion criteria (see Figure 1 for PRISMA flow diagram). Two independent reviewers (AR, JF) performed screening and data extraction; conflicts were resolved by a third reviewer (AS). Included studies compared CMIs versus placebo or active control in adult patients with HCM and reported patient level outcome data. Observational studies, non-English publications, and non-human studies were excluded.
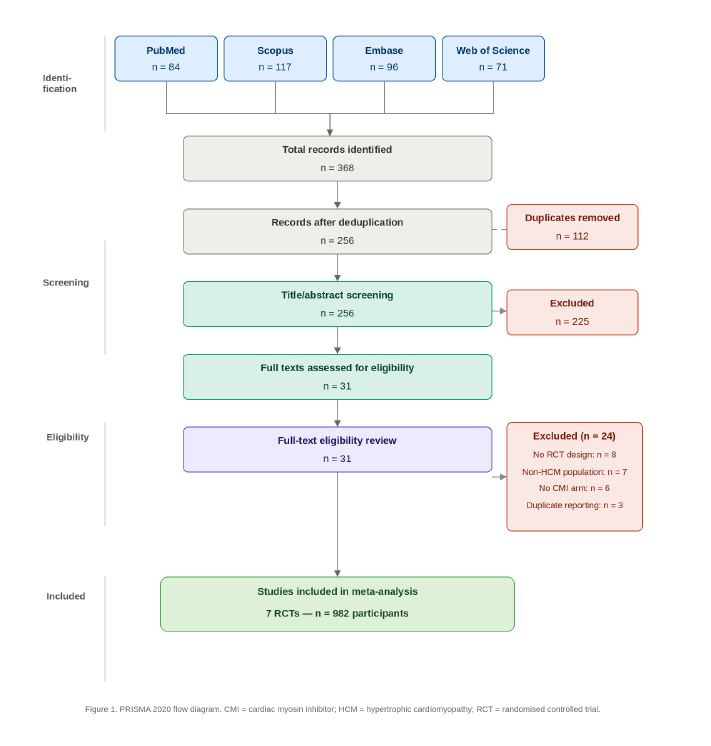
Figure 1. PRISMA flow diagram. Records identified: PubMed (n=84), Scopus (n=117), Embase (n=96), Web of Science (n=71). After removal of duplicates (n=112): 256 records screened. Records excluded at title/abstract level (n=225). Full texts assessed (n=31). Studies excluded at full-text review (n=24; reasons: no RCT design, n=8; non-HCM population, n=7; no CMI arm, n=6; duplicate reporting, n=3). Studies included in meta-analysis: n=7.
Outcomes extracted included LVOT gradients (rest, exercise, Valsalva), LVEF, complete hemodynamic response, NYHA functional class, KCCQ clinical summary score (KCCQ-CSS), peak VO2, and adverse events including atrial fibrillation. Categorical outcomes were pooled as risk ratios (RR) and continuous outcomes as standardized mean differences (SMD), both with 95% confidence intervals (CI), using random-effects models. Heterogeneity was quantified by I²; leave-one-out sensitivity analyses were performed where I² >50%. Analyses used Microsoft Excel 16 and STATA v17.
Results
Seven RCTs comprising 982 participants were included [1–7]: 531 received CMI and 451 received placebo or active control. Study characteristics are presented in Table 1 and pooled meta-analysis results in Table 2.
|
Study (Trial) |
Drug |
N (CMI / Control) |
Comparator |
Follow-up |
HCM Phenotype |
|
Ho et al. 2020 (VALOR-HCM) |
Mavacamten |
112 / 56 |
Placebo |
16 weeks |
Obstructive |
|
Olivotto et al. 2020 (EXPLORER-HCM) |
Mavacamten |
123 / 128 |
Placebo |
30 weeks |
Obstructive |
|
Tian et al. 2023 (EXPLORER-CN) |
Mavacamten |
54 / 54 |
Placebo |
30 weeks |
Obstructive |
|
Maron et al. 2023 (MAVERICK-HCM) |
Mavacamten |
40 / 19 |
Placebo |
16 weeks |
Non-obstructive |
|
Maron et al. 2023 (SEQUOIA-HCM) |
Aficamten |
99 / 83 |
Placebo |
24 weeks |
Obstructive |
|
Maron et al. 2024 (REDWOOD-HCM) |
Aficamten |
123 / 101 |
Placebo |
10 weeks |
Obstructive |
|
Garcia-Pavia et al. 2025 (MAPLE-HCM) |
Aficamten |
87 / 86 |
Metoprolol |
24 weeks |
Obstructive |
|
CMI: Cardiac Myosin Inhibitor; HCM: Hypertrophic Cardiomyopathy; LVOT: Left Ventricular Outflow Tract. |
|||||
|
Outcome |
Studies (n) |
Measure |
Pooled Estimate (95% CI) |
I² |
P value |
Interpretation |
|
Safety Outcomes Any adverse events Serious adverse events Atrial fibrillation |
7 5 5 |
RR RR RR |
1.05 (0.98–1.13) 0.87 (0.55–1.36) 0.94 (0.38–2.37) |
15.1% 0% 0% |
0.315 0.647 0.589 |
No significant difference No significant difference No significant difference |
|
Hemodynamic Outcomes LVOT gradient at rest LVOT gradient (Valsalva) LVOT gradient (exercise) Complete hemodynamic response Change in LVEF |
7 7 2 5 4 |
SMD SMD SMD RR SMD |
−5.76 (−10.35 to −1.17) −5.83 (−10.74 to −0.91) −0.65 (−1.56 to 0.26) 6.50 (1.47–28.78) −2.33 (−4.01 to −0.65) |
98.9% 99.2% — 76.7% 96% |
<0.05 <0.05 NS <0.05 <0.05 |
Significantly reduced with CMI Significantly reduced with CMI Non-significant trend Strongly favors CMI Greater LVEF reduction with CMI; attenuated in mavacamten subgroup |
|
Functional/QoL Outcomes NYHA class improvement ≥1 KCCQ-CSS score Peak VO? |
7 5 4 |
RR SMD SMD |
2.17 (1.84–2.55) 2.90 (1.06–4.74) 4.99 (−0.01 to 9.98) |
13.8% 98.9% 99.6% |
<0.001 <0.05 0.050 |
Strongly favors CMI Significantly improved with CMI Directionally favorable; high heterogeneity |
|
CI: Confidence Interval; CMI: Cardiac Myosin Inhibitor; I²: Heterogeneity Statistic; KCCQ-CSS: Kansas City Cardiomyopathy Questionnaire Clinical Summary Score; LVEF: Left Ventricular Ejection Fraction; LVOT: Left Ventricular Outflow Tract; NS: Not Significant; RR: Risk Ratio; SMD: Standardized Mean Difference; VO2: Oxygen uptake |
||||||
Safety
There was no statistically significant difference in overall adverse events (RR 1.05, 95% CI 0.98–1.13; I² = 15.1%; P = 0.315), serious adverse events (RR 0.87, 95% CI 0.55–1.36; I² = 0%; P = 0.647), or atrial fibrillation (RR 0.94, 95% CI 0.38–2.37; I² = 0%; P = 0.589) between CMIs and controls. Prespecified subgroup analyses by drug type, comparator, and HCM phenotype were not significant for any safety endpoint.
Hemodynamic outcomes
CMIs significantly reduced LVOT gradients at rest (SMD −5.76, 95% CI −10.35 to −1.17; I² = 98.9%) and during Valsalva (SMD −5.83, 95% CI −10.74 to −0.91; I² = 99.2%). Exercise LVOT reduction was directionally favorable but non-significant (SMD −0.65, 95% CI −1.56 to 0.26). Complete hemodynamic response strongly favored CMIs (RR 6.50, 95% CI 1.47–28.78; I² = 76.7%), with heterogeneity eliminated on leave-one-out sensitivity analysis. CMIs were associated with greater LVEF reduction (SMD −2.33, 95% CI −4.01 to −0.65; I² = 96%), attenuated and non-significant in mavacamten-only analysis (SMD −1.99, 95% CI −4.56 to 0.58).
Functional and quality-of-life outcomes
NYHA class improvement by ≥1 class strongly favored CMIs (RR 2.17, 95% CI 1.84–2.55; I² = 13.8%). Quality of life (KCCQ-CSS) was significantly better with CMIs (SMD 2.90, 95% CI 1.06–4.74; I² = 98.9%). Peak VO2 was directionally favorable (SMD 4.99, 95% CI −0.01 to 9.98) but characterized by very high heterogeneity (I² = 99.6%).
Conclusion
This updated meta-analysis demonstrates that CMIs provide clinically meaningful and statistically significant improvements in functional status, quality of life, and LVOT hemodynamics in patients with HCM, without a significant increase in serious adverse events or atrial fibrillation. The observed LVEF reduction was heterogeneous, attenuated with mavacamten specifically, and supports structured echocardiographic monitoring rather than precluding use.
These findings, contextualized within the growing evidence base of over 1,600 recent publications [8–12], confirm CMIs as effective, targeted, disease-modifying therapy, particularly in obstructive HCM phenotypes. Ongoing trials evaluating class effects, non-obstructive phenotypes, and long-term outcomes will further refine patient selection and therapeutic strategy[11,12].
Disclosures
The authors report no conflicts of interest. No external funding was received for this study.
References
2. Desai MY, Owens A, Geske JB, Wolski K, Naidu SS, Smedira NG, et al. Myosin Inhibition in Patients With Obstructive Hypertrophic Cardiomyopathy Referred for Septal Reduction Therapy. J Am Coll Cardiol. 2022 Jul 12;80(2):95–108.
3. Garcia-Pavia P, Maron MS, Masri A, Merkely B, Nassif ME, Peña-Peña ML, et al. MAPLE-HCM Investigators. Aficamten or Metoprolol Monotherapy for Obstructive Hypertrophic Cardiomyopathy. N Engl J Med. 2025 Sep 11;393(10):949–60.
4. Tian Z, Li L, Li X, Wang J, Zhang Q, Li Z, et al. Effect of Mavacamten on Chinese Patients With Symptomatic Obstructive Hypertrophic Cardiomyopathy: The EXPLORER-CN Randomized Clinical Trial. JAMA Cardiol. 2023 Oct 1;8(10):957–65.
5. Maron MS, Masri A, Nassif ME, Barriales-Villa R, Arad M, Cardim N, et al. SEQUOIA-HCM Investigators. Aficamten for Symptomatic Obstructive Hypertrophic Cardiomyopathy. N Engl J Med. 2024 May 30;390(20):1849–61.
6. Maron MS, Masri A, Choudhury L, Olivotto I, Saberi S, Wang A, et al. REDWOOD-HCM Steering Committee and Investigators. Phase 2 Study of Aficamten in Patients With Obstructive Hypertrophic Cardiomyopathy. J Am Coll Cardiol. 2023 Jan 3;81(1):34–45.
7. Olivotto I, Oreziak A, Barriales-Villa R, Abraham TP, Masri A, Garcia-Pavia P, et al. EXPLORER-HCM study investigators. Mavacamten for treatment of symptomatic obstructive hypertrophic cardiomyopathy (EXPLORER-HCM): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2020 Sep 12;396(10253):759–69.
8. Lim J, Kim HK. Cardiac myosin inhibitors in hypertrophic cardiomyopathy. J Cardiovasc Imaging. 2025 Dec;33(1):7.
9. Ostrominski JW, Guo R, Elliott PM, Ho CY. Cardiac Myosin Inhibitors for Managing Obstructive Hypertrophic Cardiomyopathy: JACC: Heart Failure State-of-the-Art Review. JACC Heart Fail. 2023 Jul;11(7):735–48.
10. Huynh K. Cardiac myosin inhibitors for the treatment of obstructive and non-obstructive HCM. Nat Rev Cardiol. 2025 Nov;22(11):840.
11. Lee MMY, Goldie FC, Henderson AD, Masri A, Olivotto I, Coats CJ. Efficacy and safety of cardiac myosin inhibitors in obstructive hypertrophic cardiomyopathy: Systematic review and comprehensive frequentist and Bayesian meta-analyses of Phase 3 randomized controlled trials. Prog Cardiovasc Dis. 2026 Jan-Feb;94:16–26.
12. Aman A, Akram A, Akram B, Maham M, Bokhari MZ, Akram A, et al. Efficacy of cardiac myosin inhibitors mavacamten and aficamten in hypertrophic cardiomyopathy: a systematic review and meta-analysis of randomised controlled trials. Open Heart. 2025 Feb 23;12(1):e003215.